

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
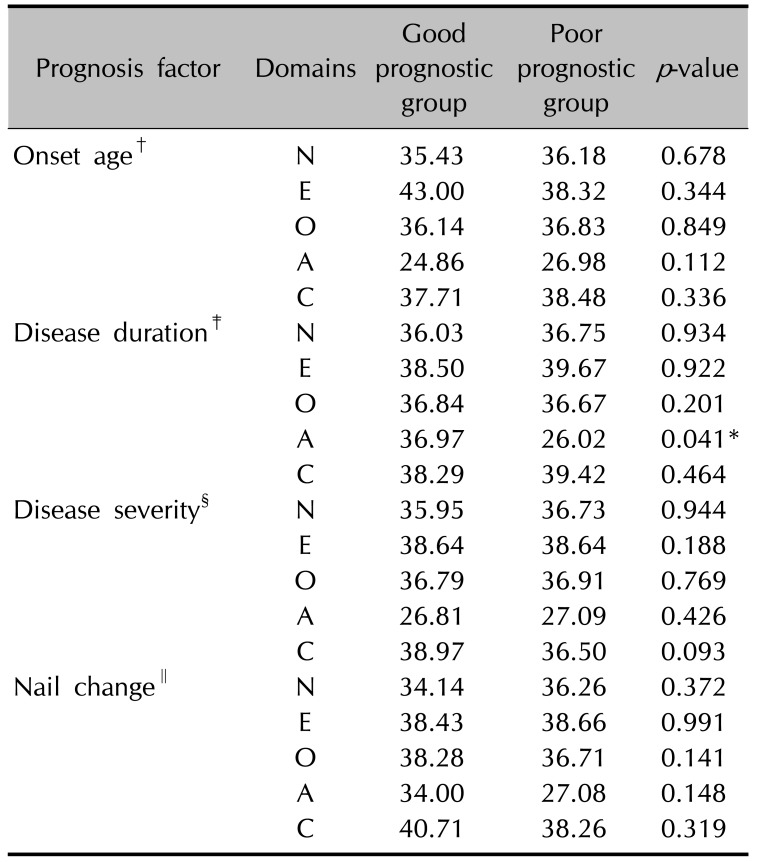
Alopecia areata (AA) can be affected by various etiologic factors including immunological and endocrine abnormalities, as well as genetic factors or psychiatric disturbances. In the context of psychiatric disturbances in patients with AA, there have only been a few studies focusing on personality traits. We guess most dermatologists have prejudice about personality trait that AA patients may have negative personality traits such as antisocial, hysterical, and anxious ones, though they can be primary or secondary. Güleç et al.1 reported that certain personality traits can modulate the onset of AA. Additionally, Carrizosa et al.2 used Minnesota Multiphasic Personality Inventory to show that AA patients express more depressive, hysterical and anxious feelings than healthy subjects. However, Alfani et al.3 recently reported that patients with AA do not have specific personality traits, as shown through an assessment using the International Personality Disorder Examination. Considering these findings, the personality traits associated with AA seems to be equivocal. Therefore, we aimed to clarify whether there are specific personality traits associated with AA patients to evaluate the correlation between prognostic factors of AA and personality traits under the assumption that these patients have a specific personality traits and that negative prognostic factors of AA can affect the formation of more negative personality traits than positive ones. One hundred patients with AA and 100 healthy subjects (control group) were included in this study. Between the two groups, there were no statistical differences in terms of sex, age or ethnicity that might reasonably be expected to have an influence on the onset of AA. After age- and sex-matching the subjects from the two groups, both patients with AA and healthy controls had consultations at our dermatologic clinic. Before the start of the study, all subjects were screened for comorbid psychiatric conditions and none of them had ever had a psychiatric diagnosis4. All subjects were asked to fill-out a NEO-Five Factor Inventor (NEO-FFI) questionnaire, the most commonly used psychological personality inventory and was developed and revised by De Fruyt et al.5. This inventory can be used to assess five personality domains of neuroticism (N), extraversion (E), openness (O), agreeableness (A) and conscientiousness (C) through a more convenient and valid method compared to that used in the original five-factor approach. All statistical analyses were performed through 2-sample t-tests using PASW Statistics ver. 18.0 software (IBM Co., Armonk, NY, USA). Comparison were made not only between the scores of the AA and control groups but also between those of 2 AA groups based on AA prognostic factors; onset age around adolescence (≤13 vs. >13 years)678, duration (≤2 vs. >2 years)9, severity (≤50% vs. >50% involvement of scalp)10, and involvement of nails7. Contrary to our expectations, the E (p=0.013) and A (p<0.001) domains of the NEO-FFI were more dominant in the AA group than in controls. Furthermore, no significant difference were found between the prognostic factors of AA and personality traits, except for a significantly lower trait A value for patients whose disease duration was over 2 years. Overall, there was no significant difference between the personality of the AA and control groups, as a whole (Table 1). Although the questionnaires and the populations from which patients and controls were selected for this study differed from those used in previous studies, we believe that our results are meaningful because they are supported by 2 distinct comparisons, namely, between AA and control groups and between 2 AA groups with different AA prognostic factors. This is the first trial that has attempted to define the relationship between personality traits associated with AA and prognostic factors of AA. Considering our findings, we conclude that negative personality traits such as such as antisocial behavior, hysteria, and anxiety are not characteristic features of patients with AA. Therefore, we agree with Alfani et al.3 in believing that patients with AA do not have specific personality traits. Thus, we need to get rid of prejudice that patients with AA have negative or specific personality traits during treatment from present study.
 XML Download
XML Download