

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alopecia areata (AA) is an autoimmune disease of the hair follicles leading to inflammatory, non-cicatricial hair loss. The estimated lifetime prevalence of AA is 1%∼2%1, and it affects all age groups with no preference for gender or ethnicity2. According to the treatment guideline suggested in 2010 by Alkhalifah et al.3, topical or intralesional corticosteroid is the accepted therapeutic option for pediatric or mild AA patients. Similarly, Messenger et al.4 also suggested that potent or intralesional corticosteroids are the most efficient therapeutic modality in limited patchy hair loss. However, possible adverse effects of potent corticosteroids, such as skin atrophy or telangiectasia are sometimes difficult, if not impossible, to reverse, and intralesional corticosteroid injection might not be suitable when dealing with young AA patients due to its painful nature. In some extreme cases, anaphylaxis in patients receiving intralesional corticosteroid for treatment of AA has been reported56.
Since introduced by Huang et al.7, the therapeutic efficacy of superficial cryotherapy in AA has been studied by various studies7891011. It is on this basis that we performed this active-controlled, half-scalp study on 19 patients with multiple, bilateral AA patches. Through this study, we investigated whether superficial cryotherapy had a significant effect on the treatment of mild AA. Also, we studied whether superficial cryotherapy has additional beneficial effects on conventional AA treatments such as topical steroids, and whether it could be a meaningful alternative treatment option if conventional AA treatment cannot be applied.
MATERIALS AND METHODS
Study design and subjects
This is a single-institution, investigator-initiated, prospective, split-scalp study with AA patients who had multiple and symmetrically distributed alopecia patches on both sides of their scalp. Exclusion criteria included any other medical condition of the scalp, and the use of any other medication or intervention. As a matter of the treatment duration, patients who had not successfully been treated for ≥1 months were also excluded. For each patient, essential background data were collected, such as age, sex, age of onset, and total duration of disease. All patients were evaluated and enrolled in the study at the Wonju Severance Christian Hospital, Wonju, Korea. This study was approved by the Yonsei University Wonju Severance Christian Hospital Institutional Review Board (IRB no. CR316010). Informed consent was obtained from all subject prior to the study.
Treatment and follow up
As a conventional treatment of AA, all subjects were allowed to apply a 0.25% prednicarbate solution to all AA patches on both sides of the scalp. Supplementarily, every patient was assigned to receive superficial cryotherapy on AA patches on the right side of the scalp, every 2 weeks at the hospital. Superficial cryotherapy was performed by spraying liquid nitrogen 3∼4 times on each AA patch for 2∼3 seconds per application, using Cryopro® (Cortex Technology, Hadsund, Denmark).
At every visit of each patient, subjective indices were evaluated. If the disease course was cosmetically acceptable, subjectively satisfactory to the patient, or hair regrowth was observed by the physician at or before the primary endpoint (4 months after starting superficial cryotherapy) and maintained for ≥1 month, the patient was considered a responder.
If a subject was considered a responder, then superficial cryotherapy was performed on both AA patches thereafter. If AA worsening was observed despite superficial cryotherapy and the application of prednicarbate solution at or before the primary endpoint, the subject was assigned to other AA treatment modalities such as diphenylcyclopropenone (DPCP) application.
Evaluation of clinical efficacy using gross photographs
At the initial visit and the primary endpoint, paired photographs were taken in both sides of the scalp, and were then evaluated by 3 different dermatologists. Each investigator assigned a Severity of Alopecia Tool (SALT) score to each patients using paired photographs, according to the scale developed by Olsen et al.12 and Olsen13. The mean SALT score the baseline and at the primary endpoint were compared. To evaluate the reproducibility of SALT scores, intraclass correlation coefficient (ICC) of SALT scores were calculated among 3 investigators using IBM SPSS Statistics software ver. 21.0 (IBM Co., Armonk, NY, USA) at the baseline, and at the primary endpoint14.
Phototrichogram analysis
On the first visit, the distance from the acoustic meatus to the nearest patch margin toward the vertex was recorded. At the first visit and the primary endpoint, the total number and mean thickness of terminal/vellus hairs was measured with a Folliscope® (Lead M Co., Seoul, Korea) on the fixed site recorded in the medical record. The number of total terminal/vellus hairs per unit area was measured with one unit defined as a 70-mm2 circular area. The thickness of the thickest 5 terminal/vellus hairs was measured with a 200× lens, and averaged to represent the overall average terminal/vellus hair thickness.
Statistical analysis
Statistical analyses including Wilcoxon signed-rank test, Mann-Whitney test, and the calculation of ICC was performed by using IBM SPSS Statistics software ver. 21.0. In calculating ICC, ICC with two-way model, consistency type, average-measures unit, and mixed effects were used. p<0.05 was accepted as significant.
RESULTS
Demographics
Nineteen patients with AA were enrolled in the study between January 2015 and October 2015, and 15 (8 male, 7 female; mean age 41.6 years) were successfully treated for ≥1 months. The mean onset age for AA was 41.4 years. The time from diagnosis to superficial cryotherapy initiation was 1∼36 months (mean, 6.3). The total number of AA patches was 2 to 14 (mean, 6.6). The total number of weeks of superficial cryotherapy treatment ranged from 4 to 32 (mean, 11.6). A summary of patient characteristics is listed in Table 112.
Clinical improvement assessed by patients and physicians
Therapeutic efficacy was analyzed in 15 of 19 patients who had received superficial cryotherapy on the right side of their scalps for ≥1 months (≥2 applications). In 73.3% of the patients (11 of 15), regrowth of terminal hair was observed by the dermatologist and maintained for ≥1 month at or before the primary endpoint, and the patient was cosmetically satisfied during the following period. The first signs of clinical improvement were observed at weeks 4 to 11, mean 10.4. Out of 11 responders, complete recovery on the treated side was observed in 2 (13.3% of total subjects). One of the 15 (6.7%) patients experienced aggravation of AA, which led to a change in the treatment regimen to DPCP application.
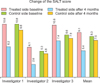
At baseline, the mean SALT score was 17.4% (ICC, 0.675; 95% confidence interval [CI], 0.405∼0.835; Fig. 1). At the primary endpoint, the mean SALT score was 12.9% (ICC, 0.913; 95% CI, 0.840∼0.956). On the treated side of the scalp, mean SALT score decreased by 40.7% (from 9.1 to 5.4, p=0.282) after 4 months of superficial cryotherapy. On the control side, change in the SALT score during the same period was 9.6% (from 8.3 to 7.5, p=0.348). In addition, the difference in SALT score between the treated and control sides were statistically not significant, both at the baseline (9.1 vs. 8.3, p=0.074) and the primary endpoint (5.4 vs. 7.5, p=0.093).
Terminal hair count as assessed by phototrichogram
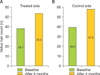
Application of superficial cryotherapy led to hair regrowth in AA lesions, compared with those on the control side, as assessed by 3 different independent dermatologists (Fig. 2). On the treated side of the scalp, the total count of terminal hair was increased 1.6-fold (from 95.6 to 159.5, p=0.005), compared to the control side, with no significant change in the terminal hair count (from 122.6 to 135.0, p=0.285; Fig. 3). When compared in a perspective of treated and control side, the mean number of terminal hair of the treated side was higher than that of the control side at the primary endpoint, without statistical significance (159.5 vs. 135.0, p=0.093).
Vellus hair count and hair thickness as assessed with phototrichograms
On the treated and control sides of the scalp, vellus hair count was 1.4- and 1.4-fold increased, respectively, without statistical significance (p=0.066 and 0.123, respectively; Fig. 4). At the primary endpoint, the mean number of vellus hair of the treated side was lower than that of the control side, without statistical significance (53.5 vs. 57.9, p=0.169).
Hair thickness showed a small decrease compared with baseline on both sides of the scalp, but was not statistically significant (p=0.185 and 0.610, respectively; Fig. 5). At the primary endpoint, the mean hair thickness of the treated side showed no significant difference to that of the control side (0.059 vs. 0.060, p=0.959).
DISCUSSION
Because of its destructive nature, cryotherapy with liquid nitrogen has been used primarily to treat cancerous skin lesions15. After Huang et al.7 introduced cryotherapy for treatment of AA in 1986, Lei et al.8 suggested the possibility of expanding its indication. Lei et al.8 suggested that when the exposure to liquefied nitrogen is limited to a few seconds (“superficial” cryotherapy), reactive vasodilation and an associated increase in blood flow may improve microcirculation and nutritional status around hair follicles. According to the study by Lee et al.10, superficial cryotherapy can induce clinical improvement of AA by blocking a yet unrevealed pathophysiologic process associated with abnormal melanocytes with large and bizarre melanosomes, found around the hair follicles of AA patients. Recently, Radmanesh and Azar-Beig16 suggested cold-induced inflammation may alter the immunologic process and structural components of the hair follicle responsible for AA. Despite these hypotheses, there is currently no established theory of how superficial cryotherapy works in the treatment of AA. Even in some aspect, superficial cryotherapy has a conflicting mechanism with the traditional AA treatments, in terms of inflammation induction and suppression. However, the therapeutic efficacy of superficial cryotherapy has been proven in various previous studies. Lei et al.8 demonstrated clinical improvement of AA lesions in 97.2% of patients after superficial cryotherapy, and Kim et al.9 showed that superficial cryotherapy induced regrowth of terminal hair in 66.7% of patients. According to a large-scale retrospective study by Hong et al.17, 68.6% of 153 AA patients achieved marked recovery of AA including terminal hair regrowth within 12 weeks. Owing to its non-destructive and minimally painful nature, superficial cryotherapy has also proven its therapeutic efficacy in treatment of AA involving fragile areas other than the scalp, such as the eyebrow1819.
Based on the results of previous retrospective studies, we sought to demonstrate the therapeutic efficacy of superficial cryotherapy as an adjuvant therapeutic option, combined with traditional topical steroid application. In this prospective, split-scalp study, 11 of 15 patients (73.3%) experienced improvement in disease indicated by regrowth of terminal hair or subjective satisfaction, including 2 patients out of 11 responders (13.3% of total subjects) who had total recovery of the AA patch on the treated side. Along with clinical improvement, the number of terminal hair on the treated side increased 1.6 times with statistical significance, with no significant change observed in the control side.
Assuredly, hasty conclusions should be avoided considering that spontaneous remissions have been reported to occur in 34%∼50% of patients within 1 year and the effects of topical steroids used in combination cannot be ignored2021. However, it cannot be overlooked that positive treatment results obtained in previous retrospective studies were also observed in our prospective study. This consistent trend can be interpreted as implying that superficial cryotherapy has a meaningful therapeutic efficacy in treatment of AA. Also, considering the relatively small subject size of this study, the possibility cannot be ruled out that positive results that were not statistically significant in this study will be validated in subsequent large-scaled prospective studies.
We have shown that superficial cryotherapy could be a meaningful adjuvant treatment option for AA patients through this prospective study. Considering that it is less painful and easier to perform, superficial cryotherapy is especially worthy of application to patients with mild AA who have difficulty with conventional treatment such as intralesional steroid injection. Further studies with a larger subject group and more investigations focused on the pathophysiology in treatment of AA are necessary.




 XML Download
XML Download