

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Bullous pemphigoid (BP) is an autoimmune subepidermal blistering disease that commonly affects elderly people. BP is characterized by erythematous tense bullae; however, clinical presentations of BP can occur polymorphically. A variety of atypical variants have been reported that have unusual clinical features, but histological and immunofluorescence (IF) findings indicative of BP123. Vesicular BP is a rare variant first described by Bean et al.3 in 1976. Unlike typical BP with large, tense, serous or hemorrhagic bullae, the vesicular variant presents with multiple small tense vesicles with a symmetric distribution, which is clinically similar to dermatitis herpetiformis (DH). Here we report a case of vesicular BP in a young male patient.
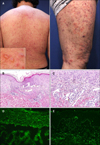
A 23-year-old male presented with a 2-month history of multiple grouped vesicles and excoriations with severe pruritus over the whole body including face (Fig. 1A). Most lesions were erosions with crusts, but intact vesicles with several millimetres in diameter were also found. The lesions were symmetric, involving the extensor surfaces more severely. The mucous membranes, palms and soles were spared. Skin biopsy showed subepidermal bullae with neutrophil and occasional eosinophil infiltration (Fig. 1B, C). Indirect IF using salt-split skin showed linear immunoglobulin (Ig)G deposition on the epidermal side (Fig. 1D). Direct IF revealed linear IgG, IgA and complement 3 depositions along the basement membrane zone (Fig. 1E). Based on these clinical and immunopathological findings, the patient was diagnosed with vesicular BP. The skin lesions were effectively controlled with oral methylprednisolone (12 mg/d) and dapsone (50 mg/d), which were tapered without relapse. The patient remains in complete remission off therapy two years after treatment.
Vesicular BP is a BP variant primarily reported in the elderly13, but it sometimes appears in children as well2. Blistering of the skin occurs; however, the lesions are smaller and distributed symmetrically, as seen in DH. The diagnosis of the present case was challenging considering the young age of the patient and the atypical clinical findings. The onset of DH is younger than BP4 and the patient's clinical symptoms were similar to DH. Diagnostic confirmation was obtained via histologic and IF studies. Histologic findings of subepidermal separation with eosinophil infiltration, direct IF findings of linear IgG deposition along the basement membrane zone, and indirect IF findings of IgG deposition on the epidermal side of salt-split skin supported a diagnosis of vesicular BP. In this patient, neutrophil infiltration was more prominent than eosinophil, which is uncommon in typical BP. Less is revealed about inflammatory cell composition of vesicular BP, and further investigation is needed.
Vesicular BP has a milder course than typical BP5, but systemic corticosteroid treatment is needed in some cases. The efficacy of methotrexate or minocycline for vesicular BP has been reported previously12. In this case, the patient responded well to low-dose corticosteroids and dapsone.
BP can present with extremely polymorphic features, and diagnosis can be challenging. A thorough evaluation with histologic and IF examination is needed for accurate diagnosis and appropriate treatment of these atypical clinical BP variants.
 XML Download
XML Download