

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Twenty-nail dystrophy (TND) of childhood was first used by Hazelrigg et al.1 to describe an idiopathic nail dystrophy in six children, which began insidiously in early childhood, and was characterized by longitudinal ridging and roughness. TND as also been referred to as ‘trachyonychia’, a term that is well suited to the clinical appearance of the affected nails234. The quality of life of patients with TND is generally decreased due to the resulting deformation of nails. The exact etiology of TND remains unclear.
Many treatment modalities are used in order to prevent nail destruction and reduce resolving duration. Therapeutic modalities such as topically-applied psoralen-ultra violet A (PUVA), triamcinolone acetonide injections, topical steroid, and systemic agents include prednisolone, anti-malarials, and etretinate in TND have been tried5678910111213. However, these treatments have low efficacies. In addition, injections are painful and thus are difficult to administer to children. Thus, a standard treatment for TND has not yet been established.
Cyclosporine is a common therapeutic agent that selectively inhibits T-cell activation, has been successfully used for various skin diseases and continues to play an important role in the field of dermatology1415. Although one recent study has reported the effects of low-dose cyclosporine in 15 patients with TND, no large-scale trial has yet been conducted16. We estimated that cyclosporine reduces spongiotic dermatitis of nail matrix by inhibiting T cell activation in TND. And pantothenic acid complex-based dietary supplement (Pantogar®; Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany) is used as a dietary supplement that helps nail growth17. Combination therapy commonly has been done when treatment effect of monotherapy is not enough. Therefore we used combination therapy based on the two above mechanisms.
The aim of the present study was to evaluate the effectiveness of oral cyclosporine in patients with TND by comparing combination therapy of cyclosporine and pantothenic acid complex-based dietary supplement and pantothenic acid complex-based dietary supplement alone.
Go to : 
MATERIALS AND METHODS
Subjects
We retrospectively reviewed the medical records and clinical photographs of 82 patients with TND who were visited from January 2000 to August 2016 at the Department of Dermatology, Hanyang University Seoul Hospital. The study was approved by the institutional review board of Hanyang University Seoul Hospital and informed consent was obtained (HYUH 2016-11-023). All patients presented with longitudinal ridging, fissuring, small regular pits, roughness, thinning, and hyperkeratotic cuticles on one or more nails and were physically healthy without any associated disease (Table 1). A total of 38 patients with TND were treated with oral cyclosporine with a pantothenic acid complex-based dietary supplement, whereas 44 patients were treated with the pantothenic acid complex-based dietary supplement alone.
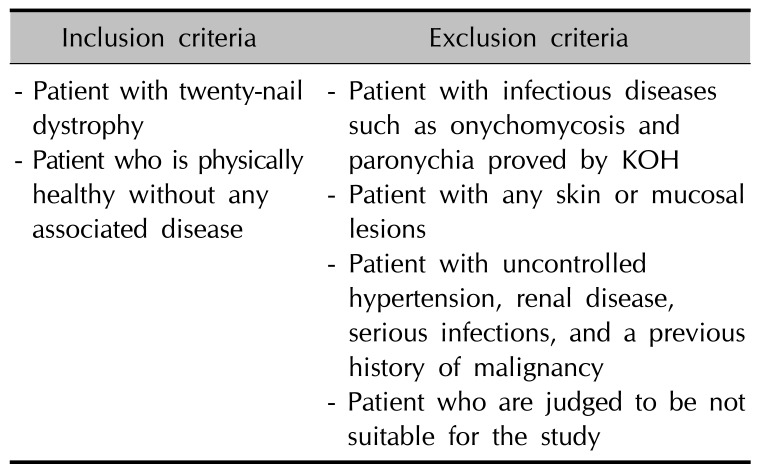
Table 1
Inclusion and exclusion criteria
![]()
Methods
1) Patient characteristics
We examined demographic information such as sex, age, body weight, disease duration, fingernail or toenail involvement, treatment history (e.g., intralesional steroid injections, topical steroids, nail operations), treatment duration, and follow-up period.
2) Cyclosporine and pantothenic acid complex-based dietary supplement (Pantogar®) regimen and follow-up
Due to ethical reasons, all 82 patients with TND were treated with a pantothenic acid complex-based dietary supplement (Pantogar®, 2~4 capsule/day) that helps nail growth. Of these 82 patients, 38 patients were also treated with cyclosporine. Patients who did not receive oral cyclosporine were assigned to the control group. During the treatment period, other treatments such as local steroid injection, PUVA, and systemic steroids were not administrated concurrently. All patients visited the Department of Dermatology regularly (once every 2 to 4 weeks). The cyclosporine dosage (100 mg, 25 mg/capsule, Cipol-N®; Chongkundang, Seoul, Korea) was adjusted to 3~5 mg/kg per day at each visit according to the patient's treatment response. Blood pressure was checked at every visit. Laboratory examination, including complete blood cell count, liver function test, kidney function test, and lipid profile, were performed before initiation of cyclosporine treatment and every 12 to 16 weeks thereafter.
3) Clinical photographs
The extent of clinical improvement was evaluated using clinical photographs that focused on the fingernail or toenail plates. Ten fingernail or toenail plates were assessed when either fingernails or toenails were involved. All twenty nails were evaluated when both fingernails and toenails were involved. Clinical photographs of the nail plate surface were captured with a digital camera (Canon DS 126201; Canon, Tokyo, Japan) at each visit. Clinical photographs were evaluated by two dermatologists. Dermatologists blindly evaluated patients' photographs without looking at patients' information. Nail plate surfaces were classified as almost clear (>75% improvement of nail dystrophy), marked improvement (>50% improvement), moderate improvement (>25% improvement), slight improvement (0%~25% improvement), no change or worse.
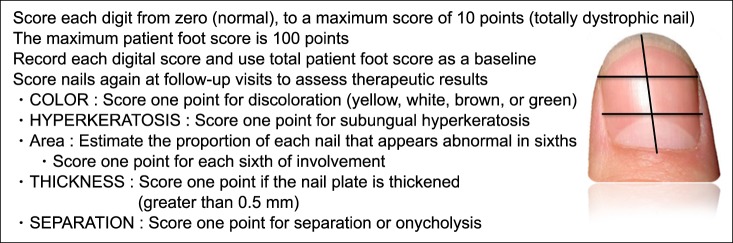
The Cleveland Foot and Ankle Clinic developed a clinical onychomycosis nail severity scoring system called the CHATS system, which is a system for scoring the severity of onychomycosis in the fingernail and toenail18. Since a standard TND severity scoring system has not yet been established, we used the CHATS system. The CHATS score (C, abnormal coloration; H, hyperkeratosis beneath the nail; A, area of involvement; T, thickening; and S, subungual separation or onycholysis) of each patient was evaluated using the clinical photographs9. One point is assigned for each of the above criteria, except for the area of involvement, which can be assigned up to six points if the entire nail plate is involved (Fig. 1).
4) Dermatology Life Quality Index
The Dermatology Life Quality Index (DLQI) score of each patient was evaluated. At the time of visiting to the hospital, patient's quality of life was recorded in the medical charts. A few questions that were not recorded in the charts were collected through telephone interview. The DLQI questionnaire includes a total of 10 questions related to symptoms, feelings, daily activities, leisure activities, work/school, personal relationships and treatment19. Each question was answered on a 4-point Likert scale (not at all, 0 points; a little, 1 point; a lot, 2 points; and very much, 3 points). The questionnaire yielded a possible maximum score of 30 points. A higher score indicates greater impairment of life quality.
5) Statistical analysis
Data were analyzed with IBM SPSS Statistics ver. 22.0 for Windows (IBM Co., Armonk, NY, USA). Differences in demographic data between the two groups were analyzed using the t-test, the Mann-Whitney U-test, and the chi-square test. The examined covariates included age, sex, body weight, disease duration, site of involvement, treatment history, treatment duration, and follow-up period. Two-way ANOVA using site of involvement as covariate was performed to analyze the significance of differences in treatment efficacy, changes in DLQI score, and changes in CHATS scores between the two groups. p-values <0.05 were defined as statistically significant.
Go to :
RESULTS
Demographic analysis
The patient demographic and descriptive variables are shown in Table 2. A total of 82 patients who were diagnosed with TND were included in this study. The cyclosporine therapy group consisted of 16 males and 22 females with a mean age of 41.55±18.66 years. The control group consisted of 18 males and 26 females with a mean age of 43.41±20.15 years. Body weight, disease duration, treatment history, treatment duration, and follow-up period were not significantly different between two treatment groups. Fingernail involvement was observed more often in cyclosporine therapy group than the control group; this difference was statistically significant (p=0.006, Table 2).
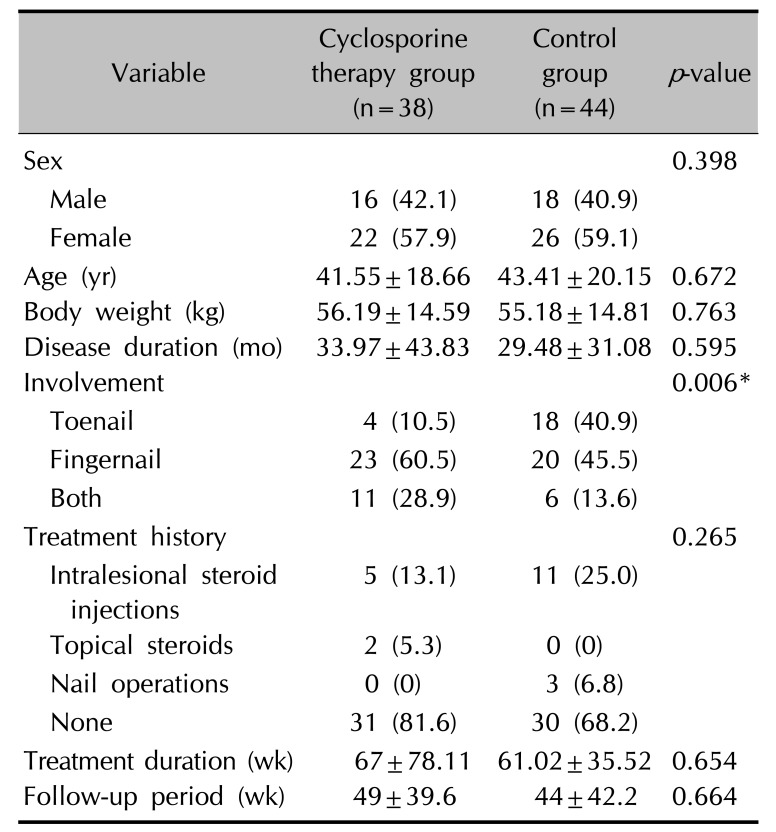
Table 2
Patient characteristics
![]()
Treatment efficacy
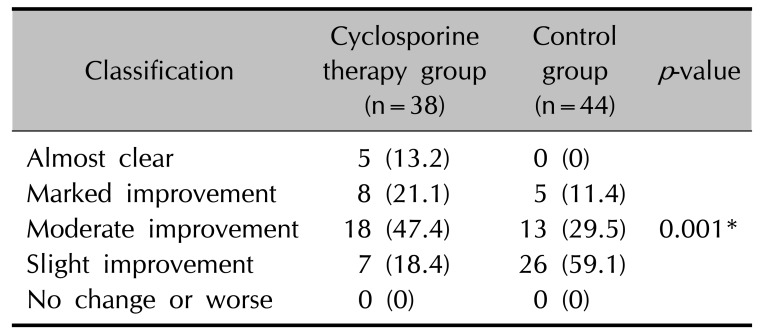
Patients who were treated with combination therapy using oral cyclosporine with the pantothenic acid complex-based dietary supplement showed better outcomes than those who were treated with the pantothenic acid complex-based dietary supplement alone (Fig. 2). The extent of clinical improvement was evaluated using clinical photographs. Of the 38 patients in the cyclosporine therapy group, nail plate roughness had almost cleared up in 5 patients (13.2%), 8 patients (21.1%) presented with marked improvement, 18 patients (47.4%) showed moderate improvement, and 7 patients (18.4%) showed slight improvement after treatment. No patients in the control group were almost clear of nail plate roughness. Five of the 44 patients in the control group (11.4%) showed marked improvement, 13 patients (29.5%) showed moderate improvement, and 26 patients (59.1%) showed slight improvement. No patient in either of the groups was scored as “no change” or “worse”. The cyclosporine therapy group had more patients whose nail roughness was almost clear, or whose improvement was marked or moderate than the control group. There was a statistically significant difference between the two groups (p=0.001, Table 3).
 | Fig. 2(A~D) Images of the fingernails in a 62-year-old woman showed ‘almost clear’ after cyclosporine therapy (treatment duration: 6 months). (E~H) Images of fingernails and toenails in a 70-year-old woman showed ‘no change’ after treating with the pantothenic acid complex-based dietary supplement only (treatment duration: 7 months).
|
Table 3
Comparison of therapeutic efficacies in the combination therapy group versus the control group
![]()
While the mean CHATS score in the cyclosporine therapy group was decreased by 13.45 (from 30.95 to 17.45), the mean score in the control group was decreased by 8 (from 29.43 to 21.43); this difference was statistically significant (F[1,76]=21.392, p<0.001; Table 4).

Changes of DLQI according to the treatment
The mean pretreatment DLQI score in the cyclosporine therapy group was 16.16. After treatment, the mean DLQI score was significantly decreased to 7.9. The mean DLQI score in the control group was decreased from 15.5 to 10.2 after treatment. The pretreatment to post-treatment change in DLQI score was greater in the cyclosporine therapy group than the control group; this difference was statistically significant (F[1,76]=3.047, p=0.085; Table 4).
Adverse effects of cyclosporine
Adverse effects of cyclosporine were reported in 4 of the 38 patients (10.53%) and consisted of gastrointestinal symptoms such as nausea and abdominal discomfort. All reported adverse effects were mild. Other severe adverse reactions and laboratory abnormalities were not observed in this study.
Go to :
DISCUSSION
TND is usually idiopathic, i.e., it may occur without any associated dermatological disease2. TND may be associated with various dermatological conditions including lichen planus, psoriasis, and alopecia areata, rare associations with vitiligo and incontinentia pigmenti have also been reported20212223. In our study, we focused on idiopathic TND that is not associated with any other dermatological condition. Inflammation of the nail matrix may produce TND. Most patients with TND show spongiotic dermatitis, with mild inflammation associated with lymphocytic exocytosis of the proximal nail fold and proximal nail matrix. Cyclosporine has a selective effect on T-cell proliferation by inhibiting the synthesis of interleukin-214. Cyclosporine acts primarily as a systemic immune modulator by binding cyclophilin and blocking calcineurin24. Cyclosporine is currently used by dermatologists in the management of psoriasis and atopic dermatitis. The therapeutic efficacy of cyclosporine in TND has been reported previously16.
Lee et al.16 reported that low dose cyclosporine administration (2.0~3.5 mg/kg per day) may be beneficial in the management of TND and in improving quality of life. In the above study, the clinical improvement was evaluated by using the clinical photos. The evaluation was classified as complete resolution, significant improvement (>50% improvement of fingernail dystrophy), slight improvement (<50% improvement), or no change. All patients with TND (n=15) presented with slight improvement of fingernail plate roughness after one month. After 6 months of treatment, 13 patients (86.7%) showed significant improvement of TND and two patients maintained slight improvement (13.3%). The mean pretreatment DLQI score was 18.1. After treatment, the mean DLQI score was significantly decreased to 9.5. However, the above study has small sample size and no comparable control group was included. Furthermore, the above study only evaluated clinical improvement of fingernails, and excluded toenails. In the present study, to evaluate the effectiveness of cyclosporine in patients with TND, a total of 38 patients with TND were treated with combination therapy using oral cyclosporine with Pantogar® and 44 patients were treated with Pantogar®. The therapeutic efficacy in each group was retrospectively evaluated using medical records and clinical photographs. The pretreatment to post-treatment DLQI change was greater in the cyclosporine therapy group (p=0.085). This result demonstrates that cyclosporine administration may be beneficial in improving the quality of life in patients with TND. The cyclosporine therapy group had more patients who were almost clear of nail roughness or whose improvement was rate as marked or moderate compared to the control group (p=0.001). The mean CHATS score in the cyclosporine therapy group decreased by 13.45 after treatment, but decreased by only 8 in control group. This difference was statistically significant (p<0.001). No severe adverse reactions to cyclosporine were observed in this study. Most of patients were satisfied about the clinical improvement after 6 months of treatment. Referencing the above out result, authors recommend that administrate 3~5 mg/kg cyclosporine per day in TND for about 6 months or longer.
We hypothesize that the therapeutic effectiveness of cyclosporine in TND results from its dramatic effects on T-cell function, as well as on pro-inflammatory cytokine release. In this manner, cyclosporine might suppress the spongiotic dermatitis and lymphocytic infiltration of the nail matrix observed in patients with TND.
The adverse effects of cyclosporine are, for the most part, dose-dependent and related to therapy duration25. Gastrointestinal discomfort is a common side effect of cyclosporine administration. Cyclosporine is contraindicated in patients with uncontrolled hypertension, renal disease, serious infections, and a previous history of malignancy, excluding basal cell carcinoma25. In our study, we excluded patients with any of the above diseases. Moreover, laboratory abnormalities or severe adverse reactions were not observed during the cyclosporine treatment period. Four of the 38 patients (10.53%) reported nausea and abdominal discomfort; however, these symptoms were mild and were alleviated by taking digestive medication. Using the recommended monitoring protocols has been shown to result in a significant decrease in the incidence of cyclosporine-related toxicities25.
Although this is the first report to assess the treatment efficacy of cyclosporine in patients with TND and to use a control group, there are some limitations to our study. First, the TND nail severity score may be less accurate due to use of a nail severity scoring system for onychomycosis. Second, our results may be subject to recall bias, since the pretreatment DLQI score was estimated retrospectively after treatment. Third, the studied population was from a small geographic area and thus our results may not be generalizable to a larger population. Fourth, our study was performed at a single-center, meaning that it may subject to selection bias. It was also a retrospective study and there may have been multiple confounding factors for which could not control. Future large, randomized, controlled multicenter trials are required to validate the correlations we report here.
In conclusion, our results show that cyclosporine is an effective treatment option for TND. Since few studies have assessed TND treatments, our study is of note in that it was conducted using a relatively large number of patients with TND. Furthermore, our study is a milestone because few studies have reported the effects of cyclosporine in TND.
Go to :
 XML Download
XML Download