

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Migraines are a common, disabling primary headache disorder, affecting approximately 15% of people worldwide (1). In about one-third of migraineurs, a headache is accompanied or preceded by an aura (2). Migraine aura is thought to be caused by cortical spreading depolarization followed by cortical spreading depression, which results in a variety of symptoms that corresponds with an affected cortex (3). Typical symptoms of an aura are homonymous visual symptoms, less often followed by one-sided somatosensory symptoms (tingling or numbness pricking) and dysphasia (4). Recently, language disturbances, memory problems and dyspraxia during an aura were recorded in 65% of patients (5). The reason that migraine aura is limited to visual symptoms (e.g., excitation of occipital cortex) in some patients yet in others is extended with somatosensory and/or dysphasic symptoms (e.g., spreading depolarization to other cortical regions) is not clear. The differences between these two migraineurs with aura (MA) subtypes is supported by a higher prevalence and frequency of interictal microembolic signals in the visual, migraineurs who experienced only visual aura (MVA) compared to migraineurs who had visual, somatosensory and dysphasic symptoms (MVA+) (6).
Magnetic resonance imaging (MRI) studies have suggested a relationship between migraines and an altered gray matter structure (78). Previous studies strongly suggested that MA is related to a dysfunctional cortex during (9), and also between migraine attacks (10). Previous research found reduced cortical surface area in the inferior temporal gyrus and decreased gray matter volume in the superior temporal gyrus, inferior frontal gyrus, and precentral gyrus (111213). A few studies have assessed cortical thickness in migraineurs with conflicting results (813141516). While certain studies found an increased cortical thickness of the primary sensorimotor cortex (8) or motion-processing visual areas (fifth and third visual cortex) (16), another study displayed no cortical thickness abnormalities (14). A recent study found concomitant cortical thickness and functional MRI differences between patients with migraine and control subjects were correlated with the frequency of attacks (15). However, a small number of migraineurs were included in those studies, as well as the lack of differentiation between patients with migraine without aura and migraine with aura or different MA subtypes. Further research is required for more conclusive results.
In the present study, a group of MA in the interictal phase of the disorder were investigated. The purpose of this study was to investigate the cortical gray matter in migraineurs with an aura with a surface-based morphometry approach. Attention was focused on 1) comparing the cortical morphometric features between migraineurs and healthy controls, 2) comparing the cortical morphometric features between subgroups (MVA+ and MVA) in migraineurs, and 3) correlating cortical morphometric features in migraineurs with characteristics of the disease.
Go to : 
MATERIALS AND METHODS
Participants
All migraineurs with an aura who visited the Headache Center at the Neurology Clinic, from the beginning of 2013 to the end of 2015, were considered as participants of this study. The diagnosis of migraine with aura was based on the International Classification of Headache Disorders criteria (beta version) (4). The inclusion criteria were as follows: 1) 18–60 years of age; 2) suffering from episodic migraines for more than one year before the first office visit; and 3) had completed a baseline headache diary. Exclusion criteria included a presence of other neurological or cardiovascular diseases, structural abnormalities on their previous MRI scans, motor and brainstem aura symptoms, chronic migraine (headache occurring on 15 or more days per month for more than three months), and patients who were on, or had a history of taking, any prophylactic medications. Eligible patients signed an informed consent to participate in the study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Selected patients were interviewed by an experienced headache investigator about their demographic characteristics and disease symptoms. According to data from migraine diaries and interviews, patients were subdivided into MVA+ and MVA during the aura, for additional and more profound analysis.
Thirty healthy subjects (HS) were voluntarily recruited from clinical staff and balanced with migraineurs in terms of sex, age, educational years, and hand predominance. HS were examined by a general practitioner and neurologist due to the need to exclude metabolic and neurologic diseases. Also, those in the HS group have never experienced any other type of a headache, except infrequent tension-type headaches, and had no family members who suffered from a migraine. All participants were screened and examined by a neurologist to ensure that they met the inclusion/exclusion criteria.
Further, participants were referred to a special hospital for prevention and treatment of cerebrovascular diseases (SHPTCD) in order to undergo MRI scans (three-dimensional [3D] T1-weighted spin echo [T1W] and T2-weighted spin echo [T2W]). All participants gave their written informed consent. Also, all patients were migraine-free at least three days before and after the MRI scan. The research protocol of this study was approved by the Review Boards of the SHPTCD and the Neurology Clinic.
Surface-Based Morphometry
The magnetic resonance (MR) examinations of patients and the HS group were performed using a 1.5T MRI scanner (Signa™, GE Healthcare, Milwaukee, WI, USA) and an eight-channel head coil. All recordings were made on the same MRI machine over a period of two months. The imaging protocol consisted of a T2W in an axial plane (echo time [TE], 105.8 ms; repetition time [TR], 5700 ms; flip angle [FA], 90 degrees, 24 slices with 0.47 × 1 × 5 mm voxels; slice thickness, 5 mm; acquisition matrix, 512 × 512) and 3D T1 weighted fast spoiled gradient-echo (T1-3D-FSPGR) series (TE, 3.60 ms; TR, 8.12 ms; FA, 15 degrees; 248 continuous slices with 0.47 × 0.47 × 1.4 mm voxels; slice thickness, 1.4 mm; acquisition matrix, 512 × 512; field of view, 256 × 256 mm2). T2W images were only used to confirm that there is no pathological finding on participants' scans. The MR images of all participants were reviewed by a board-certified neuroradiologist for any structural abnormalities and reported as normal without any white matter hyper-intensities.
Images were transferred to a PC workstation and converted to the Neuroimaging Informatics Technology Initiative using the dcm2nii software. Only T1W fast field echo volumetric images were included in the analysis. In the first step, images were checked for orientation using the fslreorient2std routine from the FSL 5.0 package. A freesurfer (version 5.3.0) analysis was performed on a HP 350 server (Intel Xeon 1800 Mhz, 8 cores, 16 GB RAM) using recon-all script for automatic cortical reconstruction and segmentation of brain structures. The average run time (with the parallelization option used) was 6 hours. The details about Freesurfer and its routines can be found elsewhere (1718). After finalization of the script, segmentation of the brain structures was manually inspected by an experienced neuroradiologist, who was blinded to subject status, to ensure that gray and white matter boundaries were correctly delineated before final surfaces were built using the reconall2 script. In order to prepare obtained surfaces for statistical analyses, smoothening was applied using the recon-all with qcache option added.
Statistical Analysis
Subject demographics and migraine with aura characteristics were reported using descriptive statistics and compared amongst the subject groups and subgroups using an independent samples t test (two-tailed) and Mann-Whitney U or chi-squared tests, as appropriate. Statistical significance levels were set at a p value of less than 0.05.
Vertex-by-vertex analyses were completed using the FreeSurfer tool QDEC for general linear model (GLM) analysis to establish differences in cortical morphometric features (cortical thickness, cortical surface area, cortical volume and cortical depth of sulci) between migraine patients and HS, as well as between migraineurs with MVA+ and MVA, while controlling for the effect of age and sex to avoid spurious results. Also, the QDEC program was used to assess the correlation between the morphometric features and patients' clinical characteristics. Cortical maps were smoothed using a smoothing kernel of a 10 mm full width at half maximum. Statistical significance levels were set at a p value of less than 0.001. Moreover, we considered significant only those clusters which also were broadly equal to or greater than 30 mm2. The statistics for the clusters were reported (e.g., the size of the cluster, cluster p value, and peak vertex coordinates in the Talairach space). A cluster-wise correction for multiple comparisons was performed using the Monte Carlo correction (significance level, 0.05; two-tailed). All analyses were performed on each hemisphere separately. Results were Bonferroni corrected for the testing of two hemispheres.
Go to :
RESULTS
Migraineurs with aura did not differ significantly from HS relative to age, sex, and hand predominance. The demographic and clinical features of 48 patients (MA) and 30 HS, as well as migraineurs subgroups, are provided in Table 1.
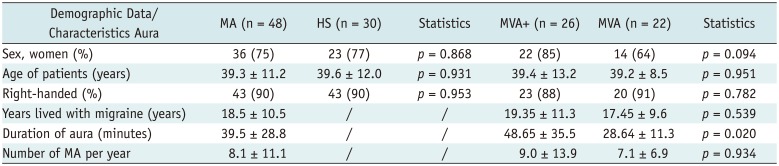
Table 1
Comparison of Demographic Data of MA (Including Aura Features) and HS
![]()
Cortical Thickness Analysis
After correction for multiple comparisons, the GLM did not display any difference between MA and HS (Table 2), as well as between the MVA+ and MVA groups (Table 3). Considering all of the migraine patients, the corrected GLM results demonstrated that there was not a significant correlation between the cortical thickness and frequency of migraine attacks or duration of disease.
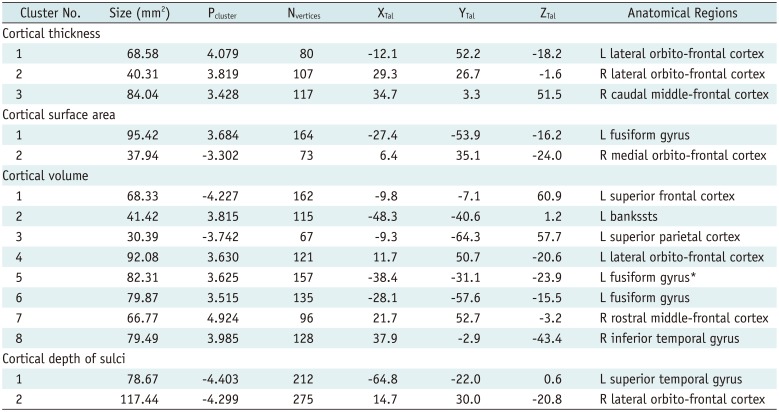
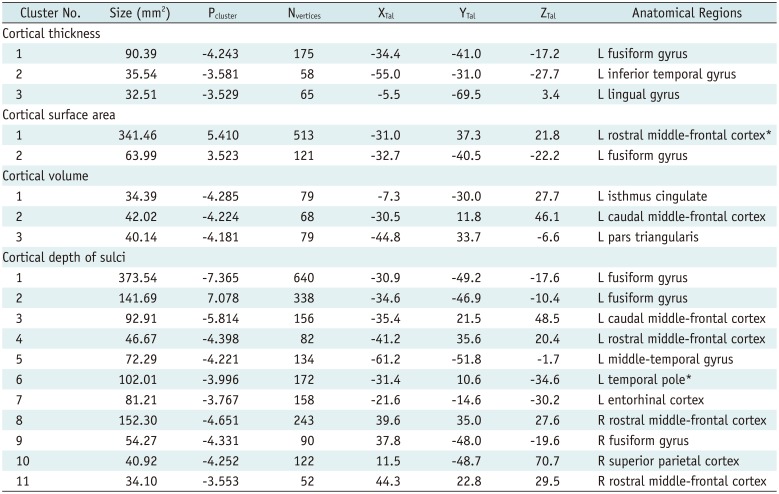
Table 2
Clusters of Significant Differences in Cortical Morphometry between MA and HS
*Surviving Monte-Carlo correction. bankssts = cortical areas around superior temporal sulcus, L = left, Nvertices = vertex number at maximum, Pcluster = maximum −log10 (p value) in cluster, R = right, XTal = Talairach coordinates for X axis, YTal = Talairach coordinates for Y axis, ZTal = Talairach coordinates for Z axis
![]()
Table 3
Clusters of Significant Differences in Cortical Morphometry between MVA+ and MVA
![]()
Cortical Surface Area Analysis
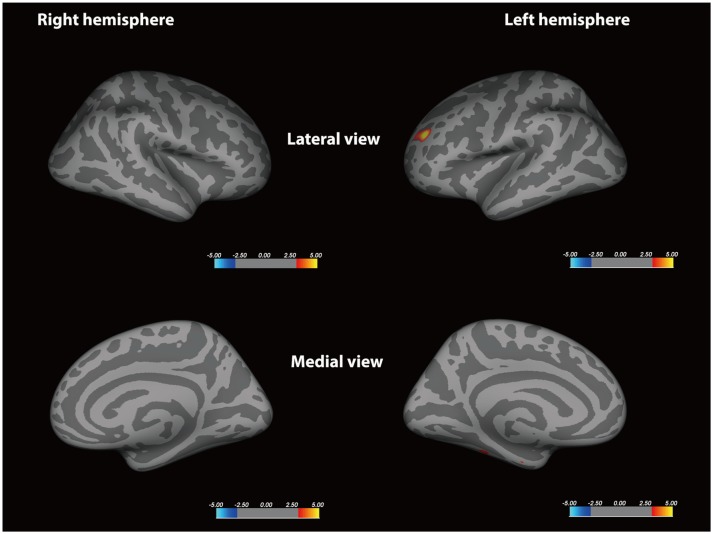
The corrected GLM did not exhibit any difference between MA and HS (Table 2, Fig. 1). Compared to the MVA group, the corrected GLM yielded a left rostral middle frontal cortex as significantly reduced in the MVA+ group (p < 0.001), which is exhibited in Table 3 and Figure 2. Considering all of the migraine patients, the corrected GLM did not find a significant correlation between the cortical surface area and frequency of migraine attacks or duration of disease.
 | Fig. 1Freesurfer whole-brain vertex-wise analysis of cortical surface area.Statistical maps controlling for effect of age and sex display decreasing (red color) and increasing (blue color) patterns in MA patients relative to HS group. Color bar shows logarithmic scale of p values (−log10). In order to visually demonstrate widespread changes, significant thresholds were set at p < 0.001, uncorrected. MA = migraineurs with aura, HS = healthy subjects
|
 | Fig. 2Freesurfer whole-brain vertex-wise analysis of cortical surface area.Statistical maps controlling for effect of age and sex display decreasing (red color) patterns in MVA+ patients relative to MVA group. Color bar shows logarithmic scale of p values (−log10). In order to visually demonstrate widespread changes, significant thresholds were set at p < 0.001, uncorrected. MVA = migraineurs who experienced only visual aura, MVA+ = migraineurs who had visual, somatosensory and dysphasic symptoms
|
Cortical Volume Analysis
Compared with the control group, the corrected GLM yielded the left fusiform gyrus as significantly reduced in the MA group (p < 0.001), which is displayed in Table 2. Compared to the MVA group, the corrected GLM yielded a left rostral middle frontal cortex as significantly reduced in the MVA+ group (p < 0.001), which is displayed in Table 3. Considering all of the migraine patients, the corrected GLM did not find a significant correlation between the cortical volume and frequency of migraine attacks or duration of disease.
Cortical Depth of Sulci Analysis
The corrected GLM did not display any significant difference between MA and HS (Table 2, Fig. 3). Compared to the MVA group, the corrected GLM yielded an increased sulcal depth of the left temporal pole in the MVA+ group (p < 0.001), which is provided in Table 3 and Figure 4. Considering all of the migraine patients, the corrected GLM did not find a significant correlation between the sulcal depth and frequency of migraine attacks or duration of disease.
 | Fig. 3Freesurfer whole-brain vertex-wise analysis of sulcal depth in cortex.Statistical maps controlling for effect of age and sex display increasing (blue color) and decreasing (red color) patterns in MA patients relative to HS. Color bar shows logarithmic scale of p values (−log10). In order to visually demonstrate widespread changes, significant thresholds were set at p < 0.001, uncorrected.
|
 | Fig. 4Freesurfer whole-brain vertex-wise analysis of sulcal depth in cortex.Statistical maps controlling for effect of age and sex display increasing (blue color) and decreasing (red color) patterns in MVA+ patients relative to MVA group. Color bar shows logarithmic scale of p values (−log10). In order to visually demonstrate widespread changes, significant thresholds were set at p < 0.001, uncorrected.
|
Go to :
DISCUSSION
The literature is replete with reports of morphologic changes in migraine, without consensus for which areas are consistently involved or strong hypotheses as to why there might be spatial variability of brain morphology in these patients. The main finding of the present study was that cortical morphology in migraineurs, possibly not only differs from HS, but also differs between the MVA+ and MVA groups. While migraineurs had cortical volume changes mostly in the temporal lobe relative to HS, the MVA+ group predominantly had an increased sulcal depth in the frontal and temporal lobes compared to the MVA group. The frequency and duration of the disease did not correlate with any morphometric feature of the cerebral cortex of migraineurs.
Previous studies have suggested structural differences in gray matter in MAs compared to the healthy control group. However, the identified differences have been quite variable across these studies (813). These divergences are suggested to be attributed to small and heterogeneous samples of participants, substantial methodological differences, as well as due to demographic and clinical differences among patients. To contribute to this topic, this study investigated a relatively large group of MA and subsequently analyzed the difference in the cortical morphology among patients with MVA+ and those who had an only visual aura. In this study, no solid evidence for differences of cerebral cortical thickness between MA and age and sex-balanced HS was found. The correlation between gray matter reduction in the anterior cingulate cortex or frontal lobes and frequency of migraine attacks found by some studies (1219) was not confirmed by our investigation.
Compared with the HS group, the MA had a reduced volume of the left fusiform gyrus. Given that an abnormality of the fusiform gyrus could lead to visual dysgnosia or prosopagnosia (2021) and grapheme-colour and tone-colour synesthetes have been found on voxel-based morphometry to have decreased gray matter volume in the left anterior fusiform gyrus (22), this study's findings support the opinion that a migraine is a condition associated with the global dysfunction of multisensory integration and memory processing (23). Also, this study's result could be correlated with the findings of a functional MRI (fMRI) study (24) that found that an increased activation of the left fusiform gyrus and interpreted it as an integrative zone that is participating in the mental imagery process related to the retrieval of pain perception.
It remains to be investigated whether these morphological cortical differences have an influence on migraine pathophysiology or are a consequence of the clinical presentation of a migraine with aura (e.g., represent adaptive neural plasticity of the central pain processing network) (25).
The division of those suffering from MA into MVA and MVA+ subgroups is in accordance with the presumed origin of cortical spreading depression (26). In this study, we quantified and compared surface-based measures in migraineurs who had MVA+ and those who had an only visual aura scanned during the interictal period. The results of this study demonstrated that patients with MVA+ had reduced cortical surface area and cortical volume of the left rostral middle frontal cortex, relative to patients with MVA. Regardless of the underlying cellular mechanism of these changes, the genetic factors influencing the cortical surface area have been found to be largely independent of the factors controlling cortical thickness (27). Moreover, since gray matter volume is a product of thickness and surface area, bearing in mind that there were no differences in cortical thickness which aligned with a previous study (13), differences in the local gray matter volume can be explained by the variation in surface area or due to the folding pattern. Overall results suggest that such morphological differences might indicate a congenital condition rather than a consequence of repeated migraines with aura attacks. Further, pediatric migraineurs also exhibit gray matter volumetric abnormalities as an adult population who suffers from a migraine supporting hypothesis of individual predisposition of morphological changes in gray matter (28). We can only speculate that different morphological features in the migraineurs subgroups allow some patients to experience disturbances of higher cortical functions during the aura.
An interesting finding of this study was the possible influence of cortical folding on a phenotype of those with migraines with aura. The MVA+ group exhibited an increased sulcal depth over most of the left hemisphere compared to the MVA group. A previous study indicated that the cytoarchitecture of gyri and sulci is greatly different in the human brain (29). Moreover, a multimodal diffusion tensor imaging/fMRI study suggested that the sulcal part of the cortex is more related to shorter connections that communicate directly with their neighboring gyri and indirectly exchange information with distant regions through gyri (30). Because of a variety of symptoms that are associated with MVA+, it is difficult to determine a specific difference in the sulcal depth between the MVA+ and MVA groups. Nevertheless, knowing the functions of the left middle temporal gyrus and temporal pole, we can speculate that increased sulcal depth in these regions somehow influences the appearance of dysphasia or dysnomia during the aura. In addition, it is known that the morphological features of the cortex in one region could have an influence on the morphological features of structurally and functionally connected regions (31). This hypothesis should be further investigated because of the possible use of the sulci depth parameter as a valuable tool in understanding the pathophysiology of higher cortical dysfunctions during an aura.
Cortical volume and surface area abnormalities were related to aura phenotype but not to disease duration and attack frequency, which is aligned with previous studies (111314). This result further strengthens the possible explanation that migraineurs have a different brain structure compared to healthy people due to their genetic background (32).
There are some limitations of this study. The subcortical gray matter and their correlations with cortical thickness were not investigated. Migraine-specific volume alteration in brainstem is documented (19); therefore, future studies of cortical morphology in MA should differentiate the influence of the subcortical gray matter on the types of migraine aura. Also, scales to measure depression, anxiety, pain intensity, and cognitive function during a headache were not measured; hence, the influence of these factors on cortical thickness was not assessed.
To summarize, subtle morphometric differences exist between the MA and HS groups in multiple regional cortical areas. Overall, the changes in the morphometric gray matter evidenced in the present study between the MA and HS groups seem to be the result of a balance between an individual predisposition and disease-related processes. Further, those suffering from MVA+ have different morphometric features in the left frontal and temporal lobe relative to MVA patients, which could be a source of the distinct symptoms and serve as potential biomarkers of the different MA subtypes. There were no correlations between morphometric features and the frequency of migraine attacks or duration of disease. Longitudinal studies are warranted for investigations of the dynamic interplay between the cortical structure and disease progression, especially for identifying the role of these changes in the clinical manifestations of migraine aura.
Go to :
 XML Download
XML Download