

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
the detection rate of thyroid nodules has increased with advancements in the imaging technology, so has the importance of accurate diagnosis in the management of thyroid lesions. Ultrasonography (US)-guided fine-needle aspiration (FNA) is considered the gold standard for initial diagnosis and offers both high sensitivity and specificity (12). Nevertheless, it is unexceptional to encounter indeterminate or unsatisfactory FNA results (3). The Bethesda System for Reporting Thyroid Cytopathology recommends repeat FNA for any nodule with initially non-diagnostic or indeterminate cytology results (4). However, a significant percentage of repeat cytology was re-diagnosed with the same non-diagnostic or indeterminate results, up to 50% and 43%, respectively (45678). Several recent studies have shown that core needle biopsy (CNB) significantly reduces the number of non-diagnostic or indeterminate results when compared to a repeat FNA (8910111213141516). Recently, the Korean Society of Thyroid Radiology recommended that CNB can be considered as an alternative to repeat FNA for thyroid nodules with previous non-diagnostic or indeterminate cytology results (17).
In terms of CNB techniques, Nasrollah et al. (14) suggested a new sampling technique in the US-guided biopsy which acquires not only tissue within the nodule but also the nodular margin with extension into the extra-nodular tissue. Previously, we have demonstrated that employment of the new sampling technique led to an increase in the diagnostic yields for well-circumscribed and indeterminate thyroid nodules (18). So far, there is little consensus on the indications for which lesions pre-evaluated by FNA and imaging findings, would benefit from this new modified CNB procedure.
In the present work, we have extended our previous study to evaluate the diagnostic value of the modified CNB technique on a larger scale with the inclusion of a spectrum of pathological diagnoses. The main purpose of this study was to evaluate the usefulness of the modified CNB technique, which acquired samples from the center of the lesion, the capsule or periphery, and the surrounding parenchyma. Therefore, we evaluated whether the modified CNB technique could allow pathologists to make more conclusive and informative diagnoses in each of the six categories of the Bethesda System. Subsequently, the diagnostic concordance between the CNB and matched thyroidectomy specimens were analyzed in detail.
Go to : 
MATERIALS AND METHODS
Patients
This is a retrospective study of 842 patients who underwent thyroid CNB at Samsung Medical Center, Seoul, Korea from August 2002 to March 2015. Of the total, both FNA and CNB were performed in 623 patients (74.0%) and CNB alone was performed in 219 patients (26.0%). Before May 2013, a conventional CNB technique targeting only the lesion was performed. Since May 2013, a new modified CNB technique, which included the lesion and the surrounding parenchyma, has been employed for all thyroid nodules sampling at our institution. Therefore, for comparison, we divided patients into two groups as conventional group (before May 2013; n = 329) and new modified technique group (after May 2013; n = 513). Thyroidectomy was performed in 320 (38%) of the 842 patients. This retrospective study was approved by the Institutional Review Board of our institution, and the need for informed consent was waived.
FNA Cytology
The FNA procedure was performed by skilled interventional radiologists using a 22- or 23-gauge needle attached to a 10-mL syringe under US guidance (19). US findings were classified into four categories according to recommendations by the Korean Society of Thyroid Radiology published in 2011 (Table 1) (20). US images of 18 patients from outside hospital were not available for review. On an average, 2–4 passes were performed for each nodule. Aspirates were smeared onto glass slides and immediately fixed in 95% alcohol for Papanicolaou and hematoxylin and eosin (H&E) staining.
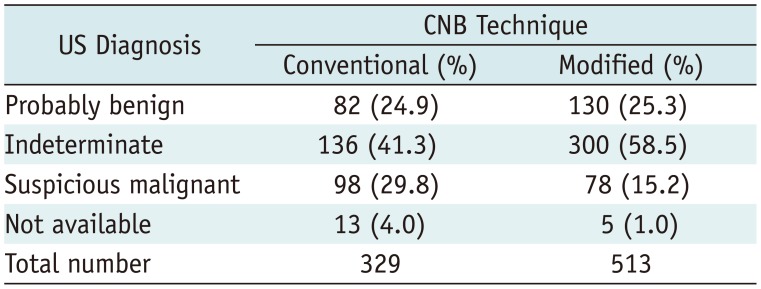
Table 1
Preoperative US Diagnosis of Thyroid Nodules according to Biopsy Techniques
![]()
CNB Procedure
After administration of a local anesthesia (1% lidocaine), an US-guided CNB was performed using a disposable 18-gauge, double-action, spring-activated needle (1.1-cm excursion) (TSK Ace-cut; Create Medic, Yokohama, Japan) by a freehand technique. The routine number of CNB cores was 2 or 3 in both the groups (18). In the conventional CNB method, two to four samples were obtained from the internal portion of the targeted lesion (18). On the other hand, in the modified CNB technique, one sample was obtained from the intra-nodular portion and the other samples (one or two) were obtained from the capsular portion including nodule and normal tissue (18). In the modified group, each biopsy specimen was placed in a separate bottle of formalin and labeled to facilitate the identification of each biopsy core. US-guided CNB procedures were performed by four expert radiologists specialized in the thyroid diagnosis with 8–14 years of experience. None of the patients exhibited any significant complications in both the groups. Perinodular hemorrhage occurred in two patients in the modified group, but the condition was subsided after manual compression. Patients complained of no pain during multiple biopsies under local anesthesia and compliance was good.
The individual biopsy cores were embedded into separate paraffin blocks, labeled according to the location of biopsy, and stained with H&E (Fig. 1). Any instance of complication or side effect was recorded in medical records.
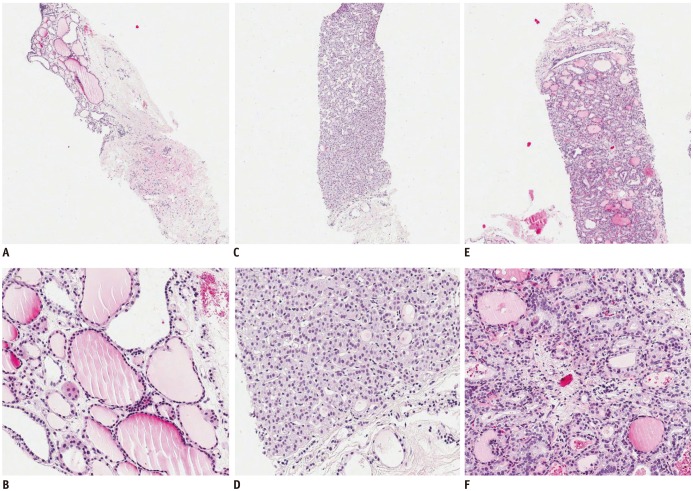
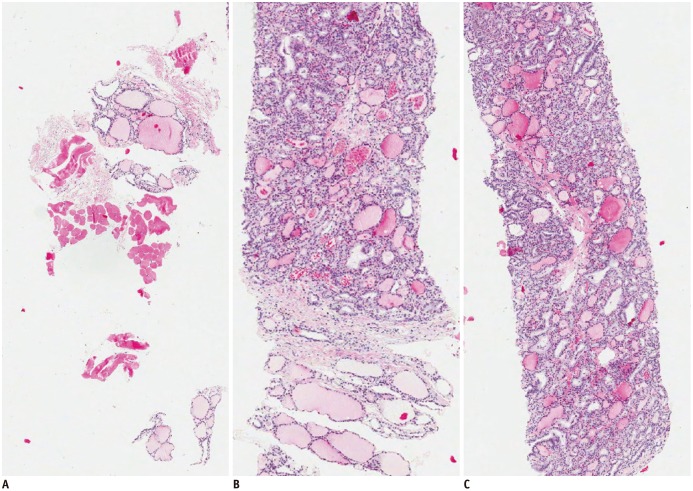 | Fig. 1Core biopsy specimens using modified CNB technique, H&E staining (× 40).This case was diagnosed as follicular variant of papillary thyroid carcinoma.
Biopsy specimens were retrieved from surrounding normal parenchyma (A), capsular portion of nodule (B), and intra-nodular target (C). CNB = core needle biopsy, H&E = hematoxylin and eosin
|
Cytological and Histological Analysis
The results of the FNA, CNB, and thyroidectomy for each case were retrieved from the electronic medical record. In addition, we retrospectively reviewed available data on age, sex, and complications after the procedure. The results of FNA were reclassified according to the Bethesda System for Reporting Thyroid Cytopathology. Bethesda category III was specifically divided into atypia of undetermined significance/follicular lesion of undetermined significance group showing architectural atypia (AUS/FLUS-A) and AUS/FLUS group showing cytological atypia (AUS/FLUS-C). However, results of the CNB samples were descriptive and varied. In order to evaluate CNB in terms of ability to provide a more conclusive and informative diagnosis, all the cases were reclassified into four categories: category 1, non-diagnostic; category 2, inconclusive; category 3, inconclusive but informative (ICBIF); and category 4, conclusive. Category 3 (ICBIF) referred to cases in which one specific diagnosis was suggested using the terminology ‘favor’, ‘suspicious for’ or ‘suggestive of,’ along with the list of differential diagnosis. On the other hand, cases were classified into category 2 (inconclusive) when only histological description or list of differential diagnosis was given. For example, the diagnosis of ‘follicular proliferative lesion, suggestive of follicular adenoma’ belonged to category 3 and the diagnosis of ‘follicular proliferative lesion, follicular adenoma vs. nodular hyperplasia’ belonged to category 2. Subsequently, we compared the diagnostic conclusiveness in the conventional and modified CNB groups.
Next, we evaluated the concordance of the final diagnoses by comparing the results obtained via CNB and thyroidectomy. The diagnosis of surgical specimens was made by several pathologists who were unaware of the results of CNB. Follicular-patterned lesions, which included nodular hyperplasia, follicular neoplasm (FN), and follicular variant of papillary thyroid carcinoma (FVPTC) were analyzed in separate subgroups (21). When surgical resections revealed a diagnosis of follicular adenoma or follicular carcinoma, the cases pre-diagnosed in CNB as FN were considered concordant, and the ones pre-diagnosed as FVPTC or nodular hyperplasia were considered discordant. However, in case of the category 2 CNB diagnosis (descriptive pre-diagnosis with a list of several differential diagnoses), it was considered concordant when any of the differential diagnoses matched the final surgical diagnosis.
Statistical Analysis
Fisher's exact test was used to evaluate the statistical significance of the CNB conclusiveness and the concordance of diagnoses obtained using CNB and thyroidectomy samples. Regarding the diagnostic ability, we evaluated whether the proportion of more informative and conclusive diagnoses (categories 3 and 4) increased compared to the diagnoses of categories 1 and 2. Statistical analysis was performed using SAS (SAS Institute Inc., Cary, NC, USA) software (version 9.4), and p < 0.05 was considered statistically significant.
Go to :
RESULTS
A total of 842 patients (181 male and 661 female, mean age 52 years) underwent thyroid CNBs. Of these patients, 623 (74%) underwent FNA before the CNB. The initial FNA was followed by the conventional biopsy method in 235 patients, while the new modified multiple-core biopsy method was used in 388 patients. The preoperative US diagnoses of thyroid nodules in the two groups are summarized in Table 1. The results of initial FNA in the two groups are summarized in Table 2. Thyroidectomy was performed in 320 (38%) of the 842 patients; 134 patients (40.7%) from the conventional technique group and 186 patients (36.3%) from the modified technique group. The size of thyroid nodules ranged from 5 mm to 63 mm. The final diagnosis corresponding to each thyroidectomy specimen is summarized in Table 3. A malignant tumor was the final diagnosis in 79.1% of the conventional technique group and 57.5% of the modified technique group.
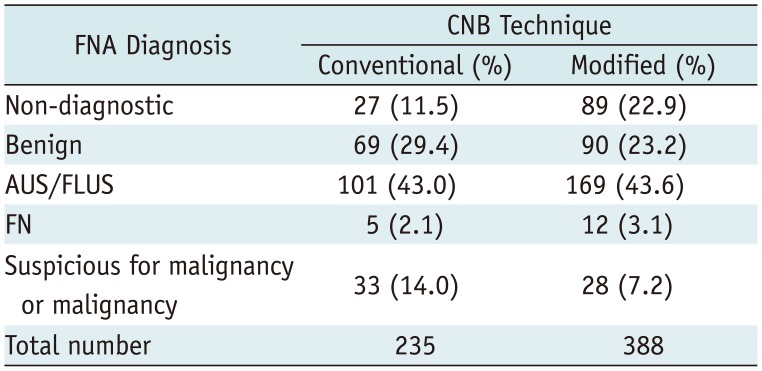
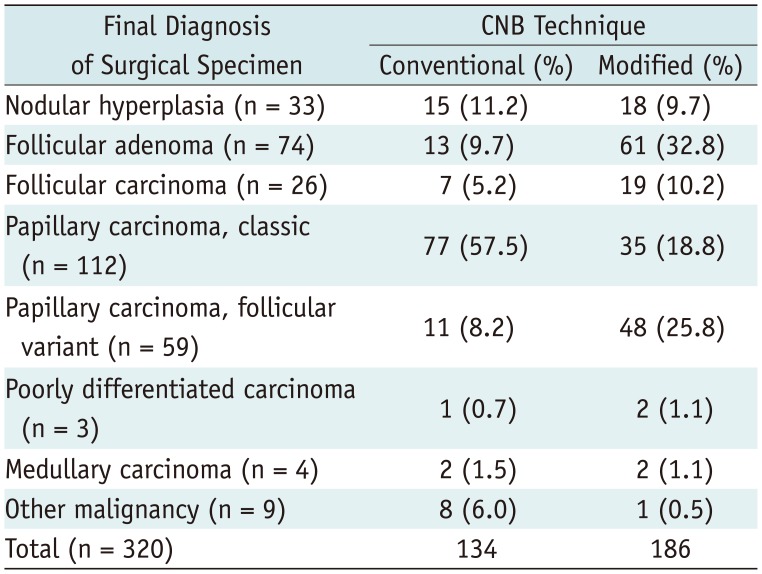
Table 2
Previous FNA Diagnosis of Conventional and Modified CNB Groups
![]()
Table 3
Final Surgical Diagnosis of Conventional and Modified CNB Groups
![]()
Diagnostic Conclusiveness of CNB: Conventional vs. Modified Technique
Overall, the proportion of more informative diagnoses (i.e., categories 3 and 4) was equivalent in the two groups (77% in the conventional technique group and 75% in the modified technique group) (p = 0.408) (Table 4). In detail, no statistically significant difference was found in the diagnostic conclusiveness between the two groups in any of the subcategories of FNA results (Table 4). However, the rate of categories 3 and 4 increased in the unsatisfactory group (70% vs. 81% in the conventional and modified technique groups, respectively), AUS/FLUS-A (73% vs. 82%), and FN group (60% vs. 91%), although no statistical significance was observed (Table 4). The rate of categories 3 and 4 did not increase in the AUS/FLUS-C group (Table 4).
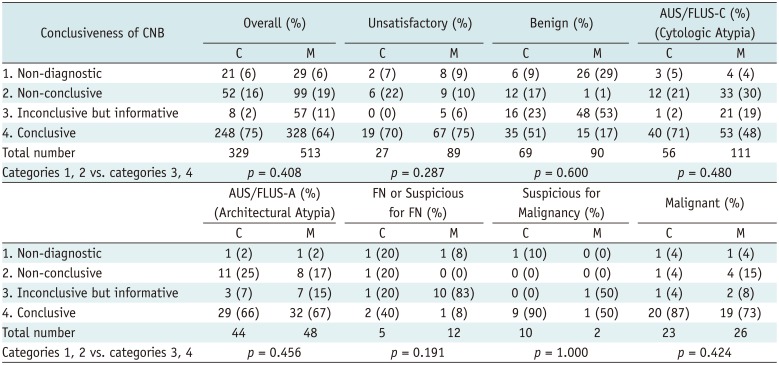
Table 4
Diagnostic Conclusiveness of CNB in Conventional vs. Modified CNB Groups
![]()
Diagnostic Concordance of CNB: Conventional vs. Modified Technique
The diagnostic concordance of the CNB and thyroidectomy specimen results were evaluated in the two groups and the results are summarized in Tables 5 and 6. The overall rate of discordance and concordance rates were 17% and 83%, respectively, in the conventional group. After the introduction of the modified technique, the rate changed to 12% and 88%, respectively; however, this was not a statistically significant change (p = 0.194).


Table 5
Diagnostic Concordance Rates between CNB and Final Surgical Resection Specimen in All Specimen, and Papillary Carcinoma
![]()
Table 6
Diagnostic Concordance Rates between CNB and Final Surgical Resection Specimen in Follicular-Patterned Lesion of Thyroid
![]()
The concordance rate was also evaluated for each histological diagnosis. Remarkably, there was a statistically significant increase in the concordance rate for follicular-patterned lesions, i.e., nodular hyperplasia, FN, and FVPTC (p = 0.033) (Table 6, Fig. 2). The concordance rate increased from 83% (38 of 46 patients) in the conventional technique group to 94% (137 of 146 patients) in the modified technique group. While the concordance rate of follicular carcinoma significantly increased (57% in the conventional group to 100% in the modified group), that of nodular hyperplasia decreased (93% in the conventional group to 61% in the modified group) (Table 6). There was no significant increase in the concordance rate for PTC (Table 5). When analyzed according to PTC subtype, FVPTC also revealed an improved concordance rate subsequent to the implementation of the modified method. The concordance rate increased from 73% (8 of 11 patients) to 98% (47 of 48 patients), which was statistically significant (p = 0.018) (Table 6).
Finally, the results of the CNB were compared with the final surgical diagnoses and the sensitivity and specificity of the CNB technique were calculated. For follicular-patterned lesions, the sensitivity increased (88.6–99.0%) and specificity decreased (75.8–64.8%) in the modified technique group.
Go to :
DISCUSSION
Core needle biopsy has been suggested as an alternative to repeat-FNA for indeterminate or unsatisfactory thyroid nodules on previous FNA (172223). CNB has advantages in differentiating encapsulated FN from the non-neoplastic nodule, especially when the new modified CNB technique is applied (17). In this study, we showed that the new modified CNB technique increased diagnostic concordance and sensitivity for follicular-patterned lesions (nodular hyperplasia, FN, and FVPTC) when compared to the conventional technique. The overall concordance rate of the surgical diagnosis was not significantly increased in the modified technique group. However, there was a statistically significant increase in the concordance rate of the diagnosis of follicular-patterned lesions.
The modified CNB technique holds significant potential in the diagnosis of FN. We showed that the diagnostic concordance rate significantly increased in follicular carcinoma. In addition, there an increasing trend of concordance in follicular adenoma was observed, despite no statistical significance. Unlike FNA and conventional CNB, the modified CNB technique allows evaluation of the capsule as well as the background thyroid (17). We made a separate paraffin block for each core and labeled the origin of each sample accordingly in the modified CNB group (24). This facilitated the pathologists' assessment of each lesion, which in turn led to a more accurate diagnosis.
On the other hand, the discordant rate of nodular hyperplasia increased in the modified group (39%) compared to the conventional group (7%), which led to the decreased specificity of the overall follicular-patterned lesion in the modified group. For surgically confirmed nodular hyperplasia cases, there was one discordant case in the conventional group, in which the CNB diagnosis was PTC. On the other hand, the CNB diagnoses of all the discordant cases in the modified group were FN. The purpose of the modified CNB technique was to increase the diagnostic accuracy of FNs, by allowing evaluation of the capsule. Although FN is characterized by encapsulation, nodular hyperplasia may also have focal areas of capsulation with micro-follicular proliferation, similar to those of FN; therefore our paradoxical outcome demonstrating little concordance among nodular hyperplasia may be attributed to selection bias of the modified CNB containing more areas of FN-like features compared to conventional CNB.
In terms of PTC, there was no significant increase in the overall concordance rate when the modified CNB technique was employed. Classic PTC is usually easily diagnosed in a single core biopsy specimen if it is properly sampled. Notably, however, FVPTC revealed an improved concordance rate subsequent to introduction of the modified biopsy technique. Together with FN and nodular hyperplasia, FVPTC is one of the main differential diagnoses for well-circumscribed lesions in the US. Making a diagnosis of FVPTC from an FNA sample is challenging for pathologists because of its wide spectrum of cytological presentations (25). The BRAF test is also of limited value in the diagnosis of FVPTC (26). In particular, the biopsy results of encapsulated FVPTC are frequently reported as indeterminate cytology because of its characteristically patchy and mild nuclear atypia (27). In such cases, the modified CNB technique can increase the detection of nuclear atypia characteristic of FVPTC, as these areas tend to be located in the subcapsular area, as per our experience.
We expected improvement in the overall diagnostic conclusiveness towards a confirmative diagnosis, regardless of diagnostic concordance with surgical specimens in the modified CNB technique; rather, a decrease in the proportion of conclusive diagnoses (category 4) and an increase in the proportion of ICBIF (category 3) was observed in the modified group. We presumed that this may have been caused by selection bias. The proportion of FN and FVPTC, which are more difficult to ascribe to a conclusive diagnosis compared to classic PTC, was higher in the modified technique group than the conventional group. Apart from selection bias, the conclusive diagnosis of FN via CNB is impossible. The histological diagnosis of FN is made only after a complete and thorough evaluation of the capsulation of a nodule on the final surgical specimen (28). Therefore, the possibility of nodular hyperplasia is always present for a follicular proliferative lesion, even in micro-follicular proliferative lesions which are highly suspicious for FN.
The proportion of FVPTC diagnosed in surgical specimens has increased since the employment of modified CNB technique. The clinical value of an accurate preoperative FVPTC diagnosis, however, is debatable. Recently, an increase in the frequency of FVPTC has been reported since the introduction of AUS/FLUS category into the Bethesda classification system and the wide establishment of the disease entity of FVPTC (4). In our institution, the increased preoperative diagnosis of FVPTC also seemed to mirror a subsequent increase in operative interventions for these lesions. While the distinction between nodular hyperplasia and neoplastic lesions (FN, FVPTC) is definitely useful, the diagnostic value of a preoperative distinction between FN and encapsulated FVPTC is uncertain. Clinically, encapsulated FVPTC has a very low risk of adverse outcomes, and some argue that FVPTC should be called “noninvasive follicular thyroid neoplasm with papillary-like nuclear features,” considering its indolent nature (27). The treatment options for FN and encapsulated FVPTC are similar. Compared to classic PTC, patients with encapsulated FVPTC are unlikely to benefit from total thyroidectomy or radioactive iodine ablation treatment (27). We assume that more accurate preoperative diagnosis of encapsulated FVPTC could deescalate the performance of unnecessary total thyroidectomy for this lesion and believe that more detailed preoperative histological information can assist surgeons in making a better preoperative plan.
This study has limitations as a retrospective study. First, we compared two groups treated at different time periods, and indications of CNB and thyroidectomy were not identical in the two groups. Second, certain cases in conventional study group contained the capsule, but the presence of capsule was not histologically evaluated. Third, the number of acquired cores varied between the cases and not only the differences in method of biopsy may affect diagnostic ability, but also the number of cores acquired (29). Large-scaled prospective studies are warranted to establish and validate indications of the modified CNB technique.
In conclusion, it is proposed that the modified CNB sampling technique, which acquires three samples including the lesion, its capsule or peripheral tissue, and the surrounding parenchyma, can increase the diagnostic concordance of follicular-patterned lesions.
Go to :
 XML Download
XML Download