

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the third most frequent cause of cancer deaths (12). Asian patients account for 80% of HCC victims worldwide (3). According to current treatment guidelines curative therapy such as: liver transplantation, surgical resection (SR) and radiofrequency ablation (RFA) are the mainstays of treatment for HCC within the Milan criteria (defined as one HCC nodule < 5.0 cm or a maximum of three nodules < 3.0 cm). Among these, liver transplantation remains the ideal option at earlier stages, yet this choice is greatly limited by the shortage of organ donors. SR might improve the patient's survival benefit (5-year survival > 70.0%) (4), but only 15–20% of patients with HCC are candidates for surgery because of either underlying chronic liver disease resulting in poor hepatic reserve or a multifocal distribution of tumor nodules (56). RFA is considered a viable alternative to SR in patients with early HCC, especially those who have impaired liver function (7). For patients with a tumor < 3.0 cm in diameter, ablation is an efficient and safe treatment that provides overall survival rate (OS) similar to those achieved with SR. However, with increasing tumor size (3.0–5.0 cm), local tumor progression from incomplete ablation is a negative prognostic factor in patients with HCC treated with RFA (8910).
Transarterial chemoembolization (TACE), as a palliative therapy, has been widely accepted for the treatment for HCC. Some studies (1112) have shown that TACE can increase the therapeutic effect of RFA, especially in large HCCs. The data from a previous meta-analysis indicates that the combination of TACE and RFA is more effective than RFA monotherapy in the treatment of patients with HCC (1314). However, whether the combination treatment of TACE plus RFA can achieve better results compared with SR for HCC within the Milan criteria is still uncertain.
Some studies have suggested the effectiveness of TACE plus RFA was associated with better recurrence-free survival rate (RFS) and OS than SR in HCC (15), while other studies reported opposite results (1617). Still other studies found that TACE plus RFA is safe and as effective as SR for patients with HCC (1819202122). This study was to meta-analytically compare combined TACE plus RFA and SR for treatment of HCC within the Milan criteria.
Go to : 
MATERIALS AND METHODS
Retrieval of Published Studies
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement. To identify relevant studies, we comprehensively searched PubMed, Embase, Web of Science, and Cochrane Library from January 2006 to August 2017. We used a combination of the terms such as “hepatocellular carcinoma” or “liver cancer,” “surgical resection” or “hepatectomy,” “radiofrequency ablation” and “transarterial chemoembolization.” A limit was set on randomized controlled trials (RCTs), cohort studies, or case-control studies that were designed to the compare clinical efficacy and safety of TACE plus RFA with those of SR for HCC within the Milan criteria. Language restrictions were not imposed in this search.
Inclusion and Exclusion Criteria
To be enrolled in this meta-analysis, clinical studies were required to fulfill the following inclusion criteria: 1) study design: the trials had to have comparative data on clinical efficacy or safety of TACE plus RFA treatment with SR in the treatment of HCC within the Milan criteria (defined as one HCC nodule < 5.0 cm or a maximum of three nodules < 3.0 cm); 2) characteristics of patients: trials were required to have relatively integrated basic characteristics of enrolled patients such as; age, percentage of males, trial design, tumor size, tumor number, Child-Pugh class, and Eastern Cooperative Oncology Group performance status; 3) outcomes: reported at least one item of the results of OS or RFS or the average length of hospital stay or major complications (which was defined as an event that led to substantial morbidity and disability, increased the level of care, hospital admission, or substantially lengthened hospital stay); 4) year of publication: from January 2006 to August 2017. The exclusion criteria were reviews without original data, expert opinions, abstracts, editorials, letters, case reports, and studies lacking control groups.
Data Extraction
Data extraction was independently conducted by two reviewers utilizing a standardized approach, with any disagreements settled by a discussion of the respective study data and adjudicated by a third reviewer. From each study, the following data was extracted: publication details (name of the first author, year of publication, and country) and study characteristics (study design, average age, percentage of men, treatment, tumor size, Child-Pugh grade, OS, RFS, and major complications). Major complications were defined as an event that led to substantial morbidity and disability, increased level of care required, resulted in hospital admission, or substantially lengthened the hospital stay. All other complications were considered minor.
Statistical Analyses
To obtain an overall comparison of the efficacy of TACE plus RFA versus that of SR, standard meta-analysis techniques were used. All analyses were performed on dichotomous outcomes. We analyzed dichotomous variables using the estimation of odds ratios (OR) with a 95.0% confidence interval (CI). Pooled OR with 95% CI were calculated with TACE plus RFA as the base category using either the fixed-effects model or the random-effects model. For each meta-analysis, the chi-squared (χ2) and I2 tests were first calculated to assess the heterogeneity of the included trials. p < 0.05 or I2 > 50.0% were considered significant. For p > 0.05 or I2 < 50.0%, the assumption of homogeneity was deemed invalid and the random-effects model was used; otherwise, data were assessed using the fixed-effects model. The quality of the case-control studies was evaluated according to the Newcastle-Ottawa scales. The quality of the RCTs was evaluated according to the revised Jadad's scale (2324). Statistical analysis was performed using the Review Manager (ver. 5.2) from the Cochrane Collaboration (http://ims.cochrane.org/revman). Results were deemed significant at a p < 0.05.
Go to :
RESULTS
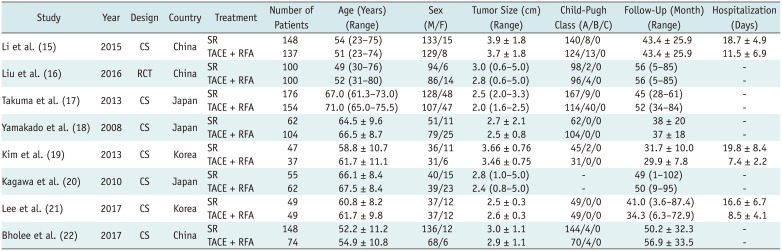
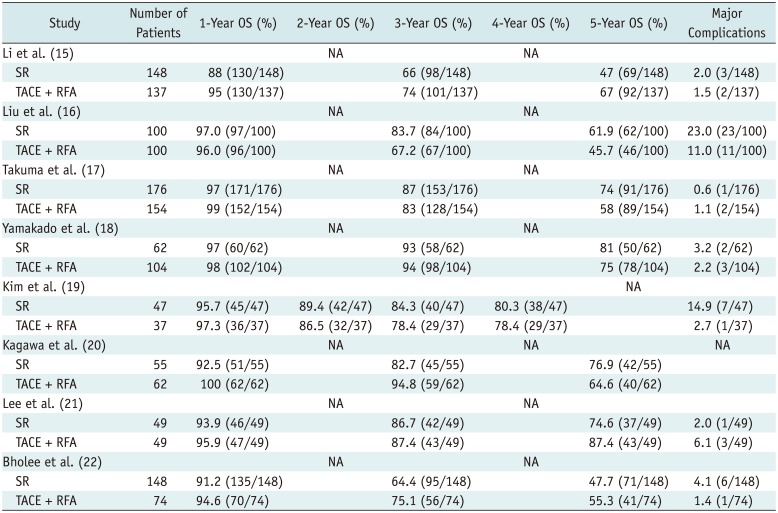
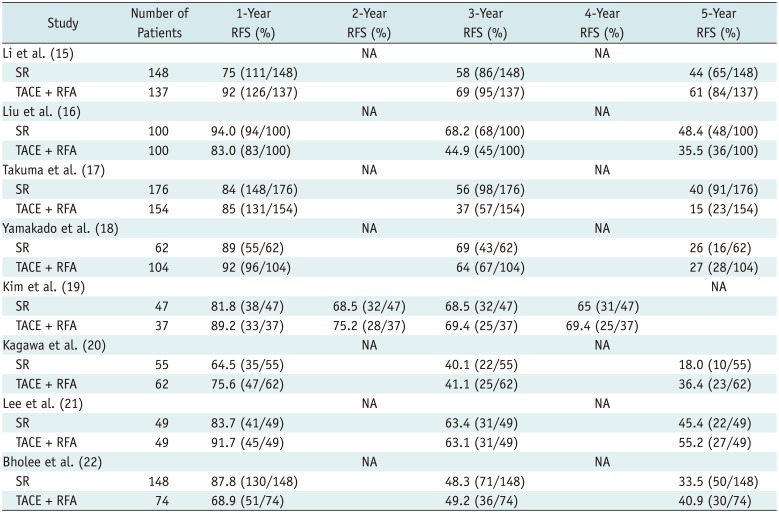
Our search yielded 64 studies. After reviewing each abstract or original publication and extracting data from the publications, seven case-control studies and one RCT were included in our meta-analysis (1516171819202122) that comprised 1502 patients, of which 785 were treated with SR and 717 with TACE plus RFA. The flow diagram of the article selection process is shown in Figure 1. The baseline characteristics of the trials, included in the meta-analysis, are listed in Table 1. The OS, RFS, and major complications of the patients in all the included trials are summarized in Tables 2 and 3.
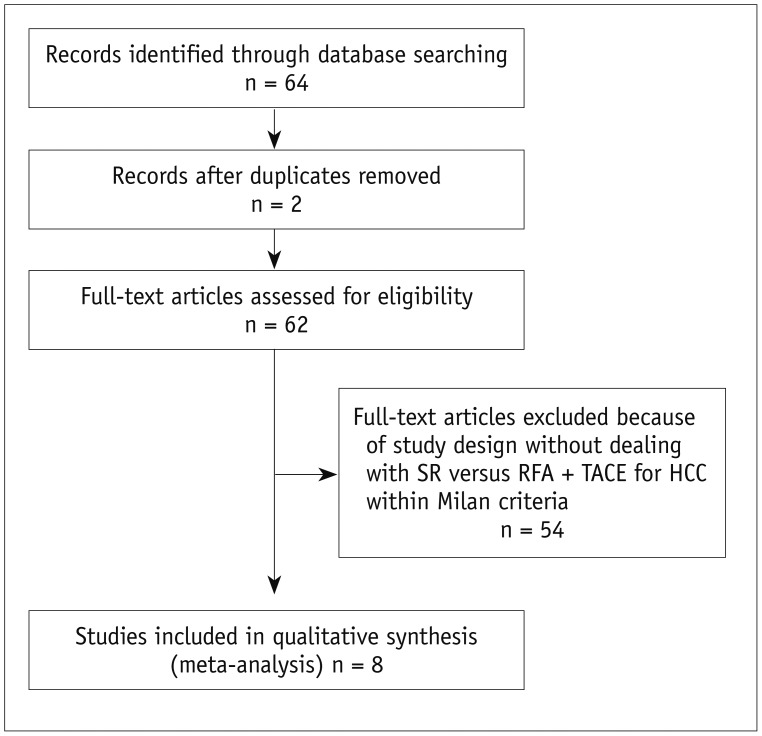 | Fig. 1Flow diagram of article selection process.HCC = hepatocellular carcinoma, RFA = radiofrequency ablation, SR = surgical resection, TACE = transarterial chemoembolization
|
Table 1
Characteristics of Included Studies
| Study | Year | Design | Country | Treatment | Number of Patients | Age (Years) (Range) | Sex (M/F) | Tumor Size (cm) (Range) | Child-Pugh Class (A/B/C) | Follow-Up (Month) (Range) | Hospitalization (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Li et al. (15) | 2015 | CS | China | SR | 148 | 54 (23–75) | 133/15 | 3.9 ± 1.8 | 140/8/0 | 43.4 ± 25.9 | 18.7 ± 4.9 |
| TACE + RFA | 137 | 51 (23–74) | 129/8 | 3.7 ± 1.8 | 124/13/0 | 43.4 ± 25.9 | 11.5 ± 6.9 | ||||
| Liu et al. (16) | 2016 | RCT | China | SR | 100 | 49 (30–76) | 94/6 | 3.0 (0.6–5.0) | 98/2/0 | 56 (5–85) | - |
| TACE + RFA | 100 | 52 (31–80) | 86/14 | 2.8 (0.6–5.0) | 96/4/0 | 56 (5–85) | - | ||||
| Takuma et al. (17) | 2013 | CS | Japan | SR | 176 | 67.0 (61.3–73.0) | 128/48 | 2.5 (2.0–3.3) | 167/9/0 | 45 (28–61) | - |
| TACE + RFA | 154 | 71.0 (65.0–75.5) | 107/47 | 2.0 (1.6–2.5) | 114/40/0 | 52 (34–84) | - | ||||
| Yamakado et al. (18) | 2008 | CS | Japan | SR | 62 | 64.5 ± 9.6 | 51/11 | 2.7 ± 2.1 | 62/0/0 | 38 ± 20 | - |
| TACE + RFA | 104 | 66.5 ± 8.7 | 79/25 | 2.5 ± 0.8 | 104/0/0 | 37 ± 18 | - | ||||
| Kim et al. (19) | 2013 | CS | Korea | SR | 47 | 58.8 ± 10.7 | 36/11 | 3.66 ± 0.76 | 45/2/0 | 31.7 ± 10.0 | 19.8 ± 8.4 |
| TACE + RFA | 37 | 61.7 ± 11.1 | 31/6 | 3.46 ± 0.75 | 31/0/0 | 29.9 ± 7.8 | 7.4 ± 2.2 | ||||
| Kagawa et al. (20) | 2010 | CS | Japan | SR | 55 | 66.1 ± 8.4 | 40/15 | 2.8 (1.0–5.0) | - | 49 (1–102) | - |
| TACE + RFA | 62 | 67.5 ± 8.4 | 39/23 | 2.4 (0.8–5.0) | - | 50 (9–95) | - | ||||
| Lee et al. (21) | 2017 | CS | Korea | SR | 49 | 60.8 ± 8.2 | 37/12 | 2.5 ± 0.3 | 49/0/0 | 41.0 (3.6–87.4) | 16.6 ± 6.7 |
| TACE + RFA | 49 | 61.7 ± 9.8 | 37/12 | 2.6 ± 0.3 | 49/0/0 | 34.3 (6.3–72.9) | 8.5 ± 4.1 | ||||
| Bholee et al. (22) | 2017 | CS | China | SR | 148 | 52.2 ± 11.2 | 136/12 | 3.0 ± 1.1 | 144/4/0 | 50.2 ± 32.3 | - |
| TACE + RFA | 74 | 54.9 ± 10.8 | 68/6 | 2.9 ± 1.1 | 70/4/0 | 56.9 ± 33.5 | - |
![]()
Table 2
OS of Patients in Included Studies
| Study | Number of Patients | 1-Year OS (%) | 2-Year OS (%) | 3-Year OS (%) | 4-Year OS (%) | 5-Year OS (%) | Major Complications |
|---|---|---|---|---|---|---|---|
| Li et al. (15) | NA | NA | |||||
| SR | 148 | 88 (130/148) | 66 (98/148) | 47 (69/148) | 2.0 (3/148) | ||
| TACE + RFA | 137 | 95 (130/137) | 74 (101/137) | 67 (92/137) | 1.5 (2/137) | ||
| Liu et al. (16) | NA | NA | |||||
| SR | 100 | 97.0 (97/100) | 83.7 (84/100) | 61.9 (62/100) | 23.0 (23/100) | ||
| TACE + RFA | 100 | 96.0 (96/100) | 67.2 (67/100) | 45.7 (46/100) | 11.0 (11/100) | ||
| Takuma et al. (17) | NA | NA | |||||
| SR | 176 | 97 (171/176) | 87 (153/176) | 74 (91/176) | 0.6 (1/176) | ||
| TACE + RFA | 154 | 99 (152/154) | 83 (128/154) | 58 (89/154) | 1.1 (2/154) | ||
| Yamakado et al. (18) | NA | NA | |||||
| SR | 62 | 97 (60/62) | 93 (58/62) | 81 (50/62) | 3.2 (2/62) | ||
| TACE + RFA | 104 | 98 (102/104) | 94 (98/104) | 75 (78/104) | 2.2 (3/104) | ||
| Kim et al. (19) | NA | ||||||
| SR | 47 | 95.7 (45/47) | 89.4 (42/47) | 84.3 (40/47) | 80.3 (38/47) | 14.9 (7/47) | |
| TACE + RFA | 37 | 97.3 (36/37) | 86.5 (32/37) | 78.4 (29/37) | 78.4 (29/37) | 2.7 (1/37) | |
| Kagawa et al. (20) | NA | NA | NA | ||||
| SR | 55 | 92.5 (51/55) | 82.7 (45/55) | 76.9 (42/55) | |||
| TACE + RFA | 62 | 100 (62/62) | 94.8 (59/62) | 64.6 (40/62) | |||
| Lee et al. (21) | NA | NA | |||||
| SR | 49 | 93.9 (46/49) | 86.7 (42/49) | 74.6 (37/49) | 2.0 (1/49) | ||
| TACE + RFA | 49 | 95.9 (47/49) | 87.4 (43/49) | 87.4 (43/49) | 6.1 (3/49) | ||
| Bholee et al. (22) | NA | NA | |||||
| SR | 148 | 91.2 (135/148) | 64.4 (95/148) | 47.7 (71/148) | 4.1 (6/148) | ||
| TACE + RFA | 74 | 94.6 (70/74) | 75.1 (56/74) | 55.3 (41/74) | 1.4 (1/74) |
![]()
Table 3
RFS of Patients in Included Studies
| Study | Number of Patients | 1-Year RFS (%) | 2-Year RFS (%) | 3-Year RFS (%) | 4-Year RFS (%) | 5-Year RFS (%) |
|---|---|---|---|---|---|---|
| Li et al. (15) | NA | NA | ||||
| SR | 148 | 75 (111/148) | 58 (86/148) | 44 (65/148) | ||
| TACE + RFA | 137 | 92 (126/137) | 69 (95/137) | 61 (84/137) | ||
| Liu et al. (16) | NA | NA | ||||
| SR | 100 | 94.0 (94/100) | 68.2 (68/100) | 48.4 (48/100) | ||
| TACE + RFA | 100 | 83.0 (83/100) | 44.9 (45/100) | 35.5 (36/100) | ||
| Takuma et al. (17) | NA | NA | ||||
| SR | 176 | 84 (148/176) | 56 (98/176) | 40 (91/176) | ||
| TACE + RFA | 154 | 85 (131/154) | 37 (57/154) | 15 (23/154) | ||
| Yamakado et al. (18) | NA | NA | ||||
| SR | 62 | 89 (55/62) | 69 (43/62) | 26 (16/62) | ||
| TACE + RFA | 104 | 92 (96/104) | 64 (67/104) | 27 (28/104) | ||
| Kim et al. (19) | NA | |||||
| SR | 47 | 81.8 (38/47) | 68.5 (32/47) | 68.5 (32/47) | 65 (31/47) | |
| TACE + RFA | 37 | 89.2 (33/37) | 75.2 (28/37) | 69.4 (25/37) | 69.4 (25/37) | |
| Kagawa et al. (20) | NA | NA | ||||
| SR | 55 | 64.5 (35/55) | 40.1 (22/55) | 18.0 (10/55) | ||
| TACE + RFA | 62 | 75.6 (47/62) | 41.1 (25/62) | 36.4 (23/62) | ||
| Lee et al. (21) | NA | NA | ||||
| SR | 49 | 83.7 (41/49) | 63.4 (31/49) | 45.4 (22/49) | ||
| TACE + RFA | 49 | 91.7 (45/49) | 63.1 (31/49) | 55.2 (27/49) | ||
| Bholee et al. (22) | NA | NA | ||||
| SR | 148 | 87.8 (130/148) | 48.3 (71/148) | 33.5 (50/148) | ||
| TACE + RFA | 74 | 68.9 (51/74) | 49.2 (36/74) | 40.9 (30/74) |
![]()
Study Quality
The quality of the case-control studies was evaluated according to the Newcastle-Ottawa scales. The quality of the RCTs was evaluated according to the revised Jadad's scale. All seven case-control studies had five to seven points, the RCT had four points.
Overall Survival Rate
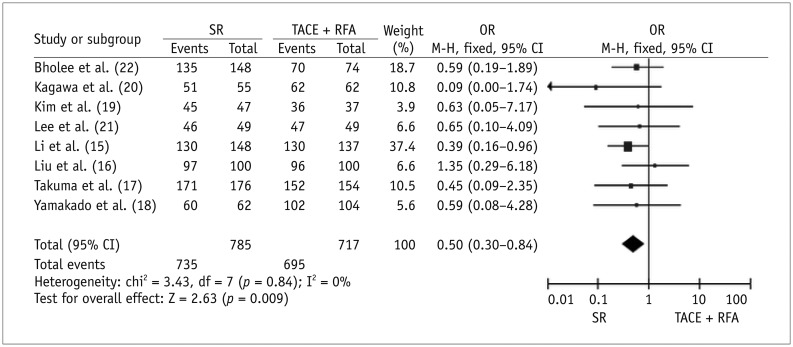
Eight studies reported data on the 1.0-year OS and there was no significant heterogeneity among these six studies (χ21-year = 3.43, I1-year2 = 0.0%, P1-year = 0.84); thus, the fixed-effects model was used to pool the results. Meta-analysis displayed that the combination of TACE plus RFA was associated with a higher 1.0-year OS compared with that of SR (OR 1.0-year = 0.50, 95% CI: 0.30–0.84, p = 0.009) (Fig. 2).
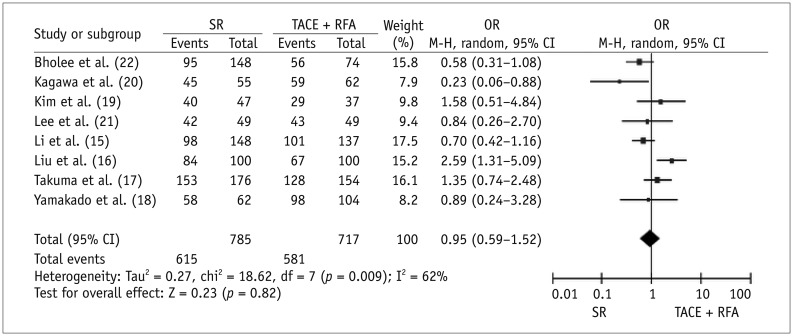
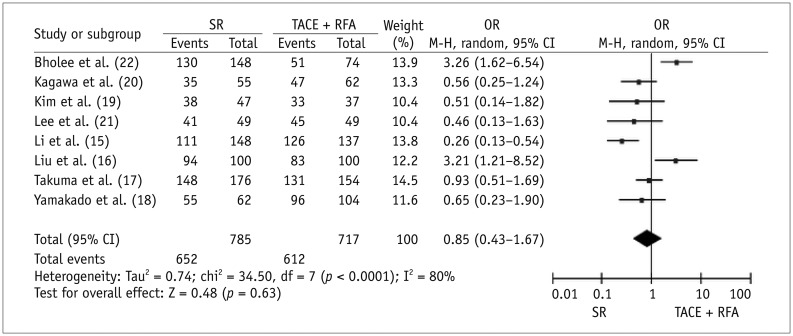
There were eight and seven studies that reported data for 3.0- and 5.0-year OS, respectively, and based on the results of tests for heterogeneity among the trials (χ23-year = 18.62, I3-year2 = 62.0%, P3-year = 0.009; χ25-year = 22.48, I5-year2 = 73.0%, P5-year = 0.001), the random-effects model was used to pool the results. Meta-analysis showed there was no significant difference between the TACE plus RFA and SR on 3.0- and 5.0-year OS (OR3-year = 0.95, 95% CI: 0.59–1.52, p = 0.82; OR5-year = 0.91, 95% CI: 0.58–1.43, p = 0.68) (Figs. 3, 4).
Recurrence-Free Survival Rate
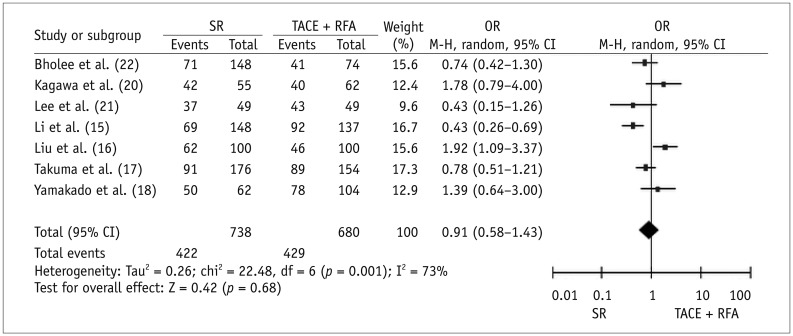
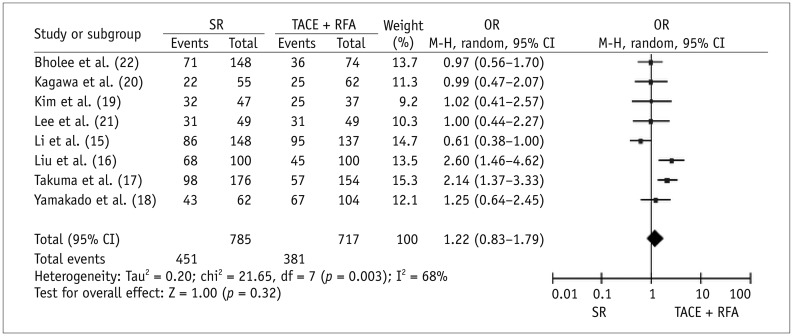
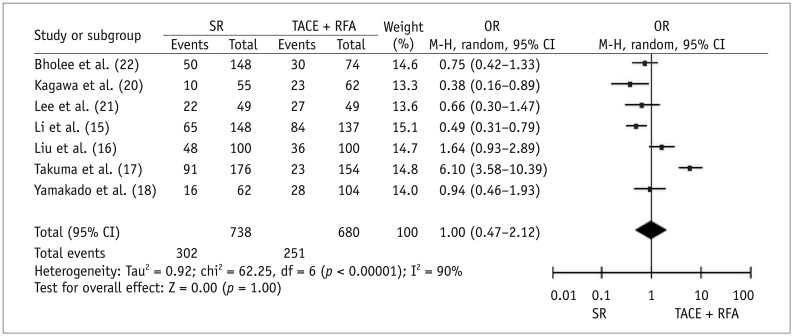
There were eight, eight, and seven studies that reported data on 1.0-, 3.0-, and 5.0-year RFS, respectively. Based on the results of tests for heterogeneity between trials (χ21-year = 34.50, I1-year2 = 80.0%, P1-year < 0.0001; χ23-year = 21.65, I3-year2 = 68.0%, P3-year = 0.003; χ25-year = 62.25, I5-year2 = 90.0%, P5-year < 0.00001), the random-effects model was used to pool the results. The meta-analysis showed that there was no significant difference between the TACE plus RFA and SR on 1.0-, 3.0-, and 5.0-year RFS (OR1-year = 0.85, 95% CI: 0.43–1.67, p = 0.63; OR3-year = 1.22, 95% CI: 0.83–1.79, p = 0.32; OR5-year = 1.00, 95% CI: 0.47–2.12, p = 1.00) (Figs. 5, 6, 7).
Major Complications
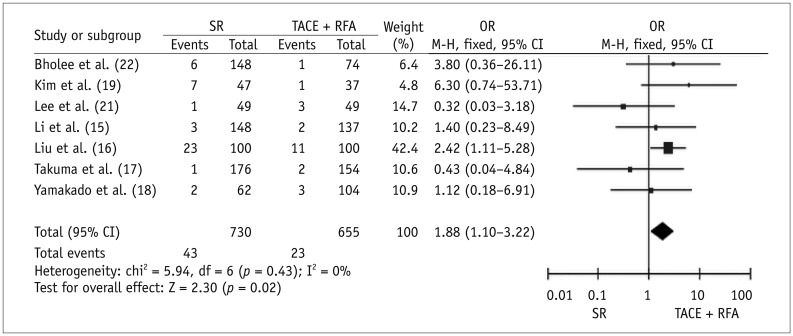
There were seven studies that reported the comparative data for major complications. Based on the results of the test for heterogeneity between trials (χ2 = 5.94, I2 = 0.0%, p = 0.43), the fixed-effects model was used to pool the results in the analysis of major complications. Meta-analysis data and forest plots indicated that SR was associated with significantly higher complications than TACE plus RFA therapy (OR = 1.88, 95% CI: 1.10–3.22, p = 0.02) (Fig. 8).
Average Length of Hospital Stay
Three studies reported on the average length of hospital stay as follows for the SR group vs. the combined therapy group: 19.8 ± 8.4 days vs. 7.4 ± 2.2 days (p < 0.0001); 18.7 ± 4.9 days vs. 11.5 ± 6.9 days (p < 0.0001); and 16.6 ± 6.7 days vs. 8.5 ± 4.1 days (p < 0.0001), respectively.
Go to :
DISCUSSION
Surgical resection remains the best treatment choice for patients with early stage HCC. As new imaging techniques and technology advance, imaging-guided therapies for liver cancer have undergone rapid developments because of their efficacy and minimal invasiveness. RFA is considered a viable alternative to SR in patients with early HCC. However, whether SR or RFA is the better alternative treatment for small HCC is still controversial (25262728). Incomplete ablation is one of the main obstacles that greatly hinder the effectiveness of RFA for HCC. The reasons are first, for the tumor with a large size or irregular shape, it is often difficult to determine the ideal ablated margin. Second, the mechanical limits of RFA and the target temperature for ablation cannot be easily reached because of the “heat sink” effect of blood vessels, especially large vessels within or around the tumor. There could exist microscopic vascular invasion and satellites around the HCC. Local tumor progression caused by incomplete ablation is a negative prognostic factor (29303132) for achieving a larger ablated zone and complete necrosis of HCC. However the combination of interventional therapies was designed for clinical practice. One such strategy is TACE plus RFA. TACE is regional therapy that treats HCC by obstructing tumor vessels and providing regional chemotherapy. TACE might reduce the heat-sink effect of large vessels adjacent to HCC, resulting in a considerable increase in the ablation zone. TACE might also be effective in treating undetected micrometastases adjacent to the main tumor. In addition, edematous change in the tumor and its surrounding area induced by ischemia and inflammation after TACE, is expected to enlarge the tumor necrosis area during the RFA procedure (333435). Thus, combining TACE with RFA is expected to reduce local progression. However, some studies consider that TACE is not necessary when RFA can completely ablate the tumor. It might increase the occurrence of adverse events (3637). Whether sequential treatment of TACE plus RFA can achieve therapeutic effects better or similar to SR is still uncertain (1516171819202122). A meta-analysis is a suitable method by which to resolve this conflict.
Guo et al.'s meta-analysis (38) showed that TACE plus RFA is safe and as effective as SR for patients with early stage HCC. However, that meta-analysis comprised only four studies. Hence, we created this meta-analysis to include more new studies to further compare the effectiveness of the two therapies and reach a more valid conclusion. Our meta-analysis data revealed that TACE plus RFA had significantly better effectiveness on 1.0-year OS. The major complications after the combined therapy were significantly lower than those after SR. There was no significant difference between the combined therapy and the SR on the 3.0- and 5.0-year OS and the 1.0-, 3.0-, and 5.0-year RFS. In addition, TACE plus RFA therapy might shorten the length of the hospital stay. Thus, we believe that TACE plus RFA has been shown to be minimally invasive and safe in treating patients with HCC within the Milan criteria, that it is a viable choice of treatment. With further research on the topic and the progress in technology scholars have reached new conclusions. In particular, Liu and colleagues' RCT (16), which is regarded as the most efficient and high-level evidence for clinical research, contributes quite a bit to the final result. For these reasons, we draw a conclusion different from that reached in Guo et al.'s study (38).
This study had several limitations. The included studies were mostly case-control studies with only one RCT, which could lead to selection bias. In addition, because of the lack of sufficient data, we were unable to perform subgroup analyses to compare the effect of TACE plus RFA and SR on patients with different disease statuses (such as < 3.0 cm HCC or 3.0–5.0 cm HCC). The inclusion criteria bias of the included studies might also affect the obvious consistency of the effects, cause between-study heterogeneity and finally influence the entire quality of our study. However, the overall quality of the studies included in this meta-analysis was detected and judged to be high. Therefore, we can determine the studies included in the meta-analysis are strong evidences to support our results. In the future, more RCTs should be enrolled to provide additional evidence.
In conclusions, combined TACE plus RFA may be an alternative to SR for the treatment of patients with HCC within the Milan criteria. Non-randomized design, in most of the original studies, was a limitation.
Go to :
 XML Download
XML Download