

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant biliary hilar obstruction (MBHO) is very difficult to cure because only 10–20% of patients are suitable for curative resections (1). Adequate biliary drainage is essential to improve the quality of life and overall survival in patients with unresectable tumors (23). Accordingly, the placement of a self-expandable metallic stent, for hilar obstruction, has been established as an effective palliative treatment for MBHO (456).
Although many investigators agree that the placement of a metallic stent is useful, several controversies have emerged regarding the details of practical methodologies. First, there are concerns over whether placement of the stent should be bilateral or unilateral (5789). Bilateral stent placement are preferred by some investigators, not only because it can preserve the functional volume of the liver during chemotherapy, but also because it can prevent procedure-related cholangitis in a contaminated and undrained lobe (41011). However, other investigators have argued that unilateral stent placement can achieve effective palliation in properly selected patients with low risk of complications (12). Second, covered stents have been used to prevent tumor ingrowth; however, less is known regarding the outcomes following covered stent placement (131415).
The purposes of this study were to investigate the technical and clinical outcomes of percutaneous metallic stent placement in patients with MBHO. Additionally, this study was conducted to compare the outcomes between bilateral and unilateral stenting methods and between covered and uncovered stents.
Go to : 
MATERIALS AND METHODS
Patient Population
The Institutional Review Board approved this retrospective study and waived the requirement for informed patient consent. From January 2007 to December 2014, 415 patients (men, 261; women, 154; mean age, 65 years [range, 29–92 years]) with MBHO (Bismuth II or higher) were included in this study. None of the patients were surgical candidates because of advanced staging, unresectability, comorbidities, and when endoscopic management was unsuccessful. The exclusion criteria included a high risk of bleeding (international normalized ratio value > 1.5 and platelet count < 50000/mm3) or a poor general condition (Eastern Cooperative Oncology Group performance status grade 3–4). The patients' characteristics are presented in Table 1. Short-term outcomes, including the technical success rates, procedure-related complications and rate of successful internal drainage, were evaluated in 415 patients. Long-term outcomes including stent occlusion-free survival, overall survival and the causes of stent occlusion, were evaluated in 318 of 415 patients with successful internal drainage who were not lost to follow-up (Fig. 1). Information regarding the patient's current health status for all patients was obtained by telephone or from their medical records.
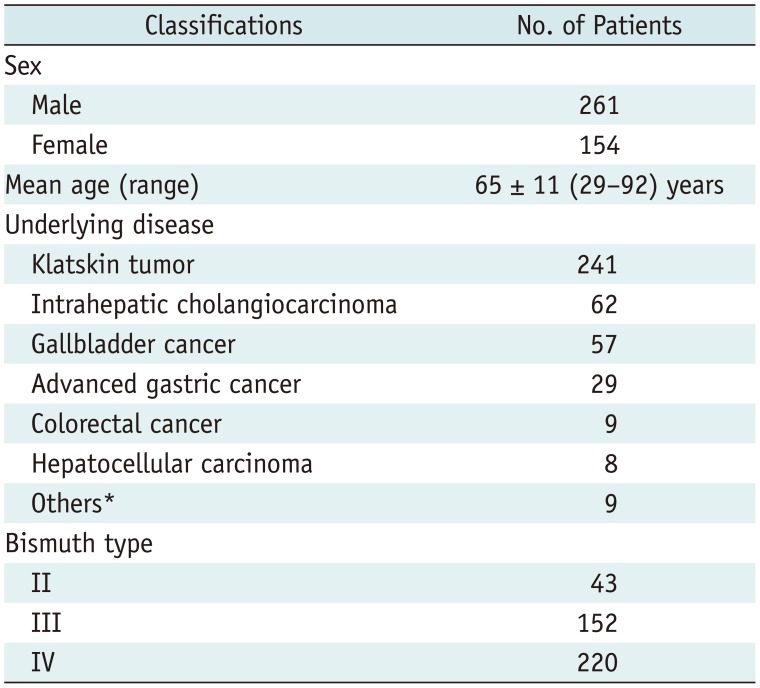
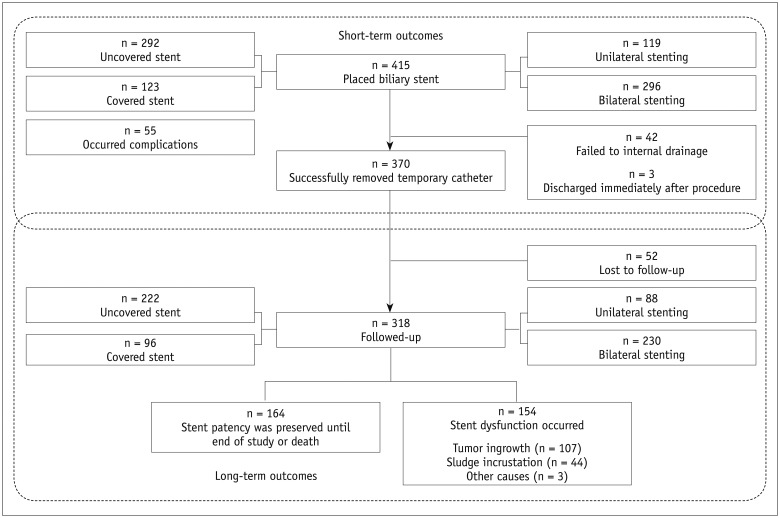
Table 1
Patient Characteristics of 415 Patients Treated with Stent Placement
![]()
Technique
The decision to perform unilateral or bilateral stenting was based on clinical findings which included cholangitis and cholangiography. If a patient exhibited symptoms of cholangitis at admission, we attempted unilateral drainage of the lobe that had the patent portal vein. If cholangitis was relieved after the initial unilateral percutaneous transhepatic biliary drainage (PTBD), we performed a unilateral uncovered or covered stent placement. If cholangitis persisted after the unilateral PTBD, we attempted to drain both lobes by catheter advancement or with an additional contralateral PTBD. If the contrast material did not enter the contralateral ducts before stent placement, unilateral stenting was performed. If the contralateral ducts were opacified, bilateral stenting was attempted due to the increased risk of cholangitis.
In patients with patent bilateral portal flows, a larger lobar hepatic duct volume was initially drained. Several days after the first PTBD, bilateral drainage was performed. We initially attempted to utilize the T configuration. This consisted of bilateral uncovered or covered stent placement through single percutaneous sites in all patients, because it did not require a contralateral puncture. However, when the negotiation of a guidewire into the contralateral duct failed, the Y configuration, which consisted of bilateral uncovered or covered stent placement through the bilateral percutaneous sites, or the crisscross configuration, which consisted of bilateral uncovered stent placement through bilateral sites, was used. Both uncovered stents (Zilver, Cook Medical, Bloomington, IN, USA; Sentinol™, Boston Scientific, Galway, Ireland; or Niti S stent, TaeWoog Medical, Kimpo, Korea) and covered stents (ComVi™, TaeWoog Medical; Hercules, S&G Biotech, Seongnam, Korea; or GD stent, TaeWoog Medical) were utilized. The covered stents were partially polytetrafluoroethylene (PTFE)-covered Nitinol stents with 2- or 3-cm bare extensions at the proximal end to prevent tumor overgrowth, stent migration, and intrahepatic duct occlusion. All stents were available in diameters of 6, 8, and 10 mm and in lengths of 6, 8, and 10 cm. The stent deployment technique, configuration, and types of each stent were chosen by the physician operators according to their personal preferences.
After stent placement, one or two temporary drainage catheters were inserted, just proximal to the stent(s). These temporary catheters were removed after 2–3 days of clamping, when the contrast agent flowed through the stent(s) into the duodenum was confirmed by cholangiography.
Study Endpoints and Definitions
The study endpoints included technical success, complications, successful internal drainage, overall survival and stent occlusion-free survival. Technical success was defined as stent placement in an appropriate position across the stricture and in good contrast medium passage through the stent. The complications were classified as major and minor according to the Society of Interventional Radiology Standards of Practice Committee guidelines (16). Successful internal drainage was defined as the removal of temporary drainage catheters and decrease in serum bilirubin levels to below 75% of the pretreatment value by the end of the first month. The interval between the initial stent placement and the patient's death or last follow-up was acquired to analyze the overall patient survival. The interval between the initial stent placement and the recurrence of the stent occlusion or the patient's death or last follow-up in the case of no recurrence of stent occlusion was also obtained to analyzed stent occlusion-free survival. Stent occlusion was defined as biliary obstruction, confirmed either endoscopically or radiologically, serum bilirubin levels greater than 3 mg/dL, or any other condition requiring intervention to improve biliary drainage. Sludge incrustation was defined as occlusion of the stent with sludge which could be removed by a balloon sweeping. Tumor ingrowth was defined as tumor growth into the stent lumen that could not be cleared by a balloon sweeping. Tumor overgrowth was a new stricture occurring at both ends of a stent.
Statistical Analysis
The independent samples t test was used to compare pairs of independent and continuous variables between the groups. Pearson's chi-square or Fisher's exact test was used to compare categorical variables between the groups. Stent occlusion-free survival and overall survival were estimated using the Kaplan Meier method. They were compared between unilateral and bilateral stenting methods and between uncovered and covered stents using multivariable Cox regression analysis that included covariates of age, sex, Bismuth classification, stent occlusion, and complications. The analyses were conducted using statistical software (SPSS, version 17.0; SPSS Inc., Chicago, IL, USA) and p < 0.05 was considered significant.
Go to :
RESULTS
Short-Term Outcomes
Technical success was achieved in all 415 patients and 784 of the self-expandable metallic stents were successfully deployed in the biliary hila. Patients underwent unilateral (n = 119) or bilateral (n = 296) metallic stent placements using covered (n = 123) or uncovered stents (n = 292). In 119 patients, unilateral metallic stent placements (covered stents, n = 60; uncovered stents, n = 59) were performed to relieve malignant hilar obstructions. In 296 patients, bilateral metallic stent placements (covered stents, n = 63; uncovered stents, n = 233) were performed in a T configuration (n = 174), Y configuration (n = 86), or a crisscross configuration (n = 36).
Minor, procedure-related complications occurred in 30 patients (7%), including 15 with self-limiting hemobilia which resolved within 3 days without any transfusion and 13 with cholangitis that resolved within 3 days following antibiotic therapy. One patient developed bile peritonitis but improved without sequelae. Another patient had a fistula between the hepatic vein and the bile duct but spontaneously resolved without intervention. Major complications occurred in 25 patients (6%). These included; hemobilia due to arterial injury that was successfully treated by transarterial embolization in 4 patients, cholecystitis that was managed by cholecystostomy and the administration of antibiotics in 11 patients, and bilomas that required percutaneous drainage in 10 patients. In terms of the complication rates, the unilateral and bilateral stent groups were not significantly different (p = 0.065) but the uncovered and covered stent groups were significantly different (p < 0.001). Moreover, all complications recovered with appropriate management and were not associated with any serious sequelae or mortality.
Three patients were discharged immediately after stent placement; thus, the removal of the temporary drainage catheters was not verified. Successful internal drainage was achieved in 370 (89.1%) of 415 patients, including 106 (89.1%) of the 119 patients in the unilateral stent group and 266 (89.9%) of the 296 patients in the bilateral stent group, as well as 261 (89.3%) of the 292 patients in the uncovered stent group and 111 (90.2%) of the 123 patients in the covered stent group. Catheters could not be removed in the remaining 42 patients due to increased serum bilirubin levels caused by rapid disease progression (n = 27), fever after catheter clamping (n = 6), immediate stent dysfunction (n = 4), recurrent hemobilia (n = 4), or septic shock (n = 1). The mean serum bilirubin level, that was 9.4 ± 7.7 mg/dL before drainage, decreased significantly to 2.9 ± 5.3 mg/dL 1 month after stent placement (p < 0.001).
Outcomes were compared between the unilateral and bilateral stenting groups as well as between the covered and uncovered stent groups (Table 2). The stent type and configuration used did not significantly affect technical success, complications, or successful internal drainage.

Table 2
Short-Term Outcomes Regarding Technical Success, Complications, and Successful Internal Drainage in 415 Patients
![]()
Long-Term Outcomes
Patient Survival
Of the 370 patients, 52 were lost to follow-up. The remaining 318 patients were followed until death or the end of the study. The cutoff date for data analysis was December 31, 2015. During the mean follow-up period of 278 days (range, 20–1641 days), 315 patients died and three survived. Four patients died within 30 days of stent placement due to the rapid progression of underlying malignancies that were unrelated to complications caused by the procedure. The patients' characteristics are summarized for the unilateral and bilateral stenting groups (Table 3), as well as for the covered and uncovered stent groups (Table 4).
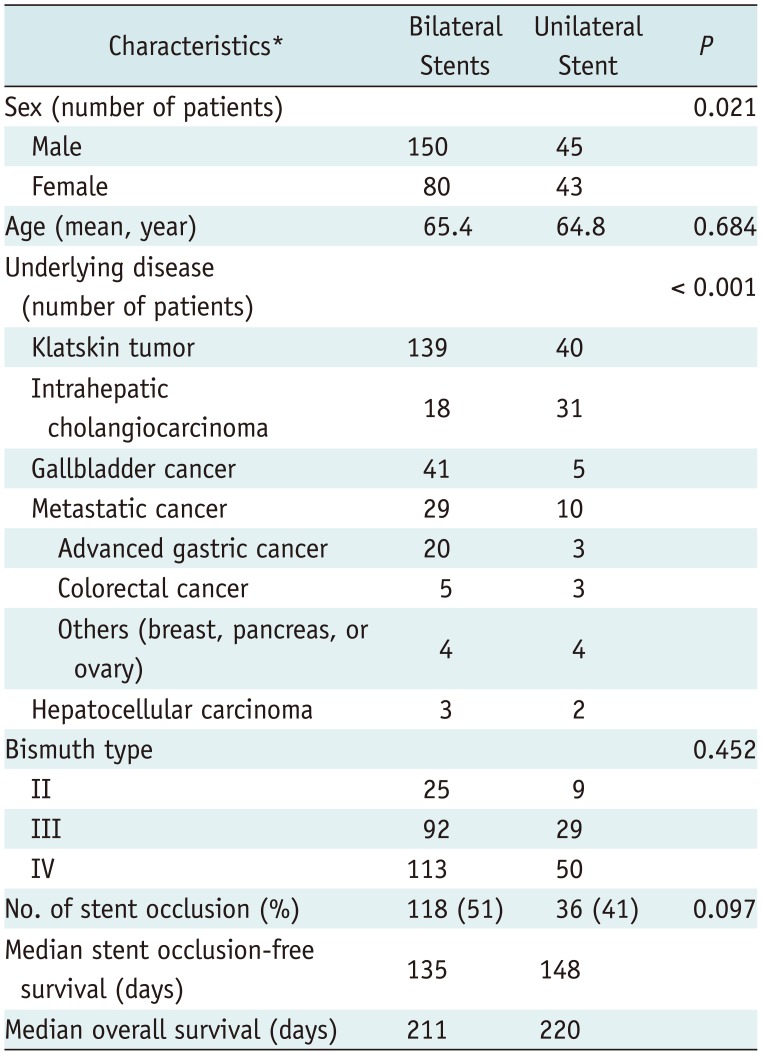
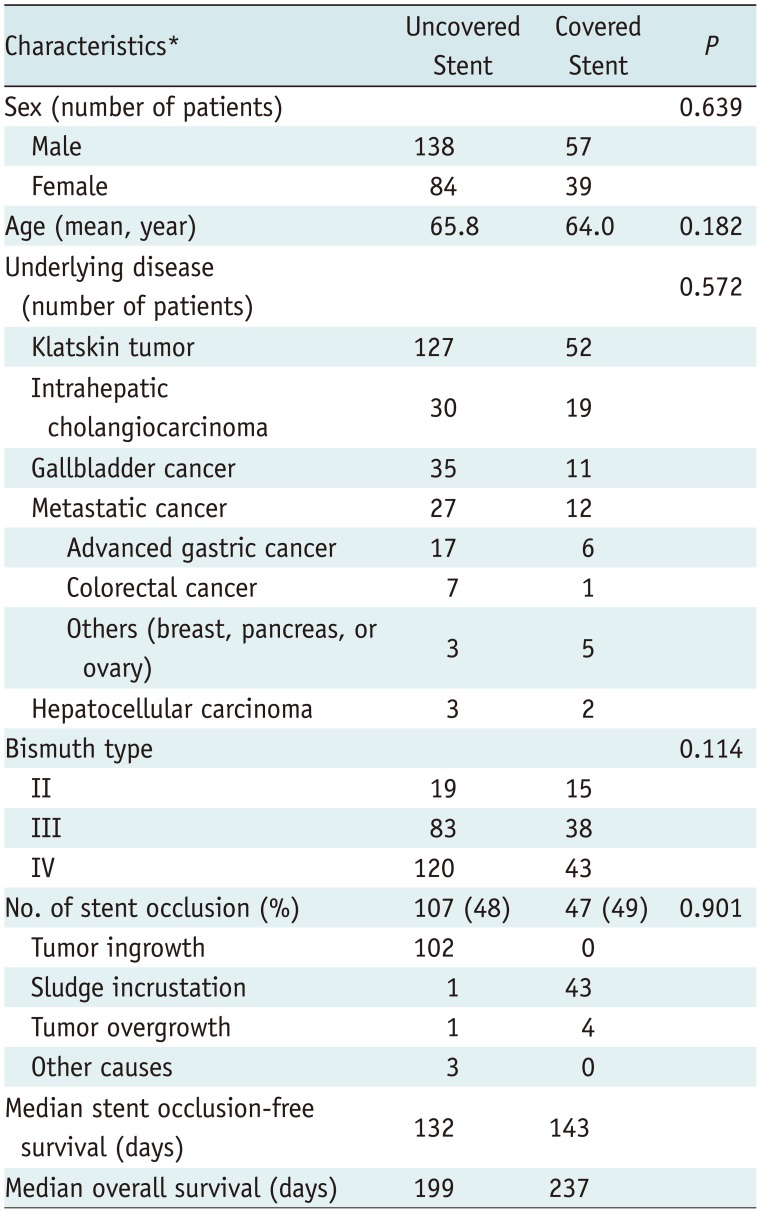
Table 3
Characteristics and Outcomes of Bilateral Versus Unilateral Stenting Groups
![]()
Table 4
Characteristics and Outcomes of Covered Versus Uncovered Stent Groups
![]()
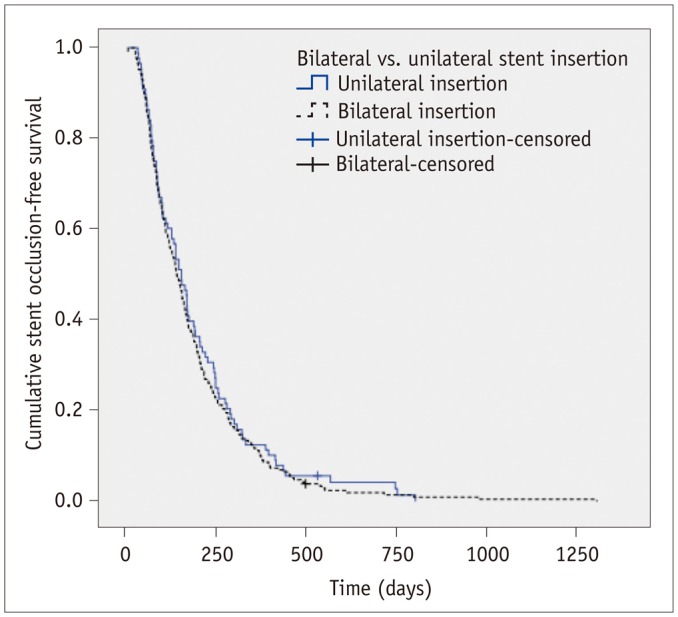
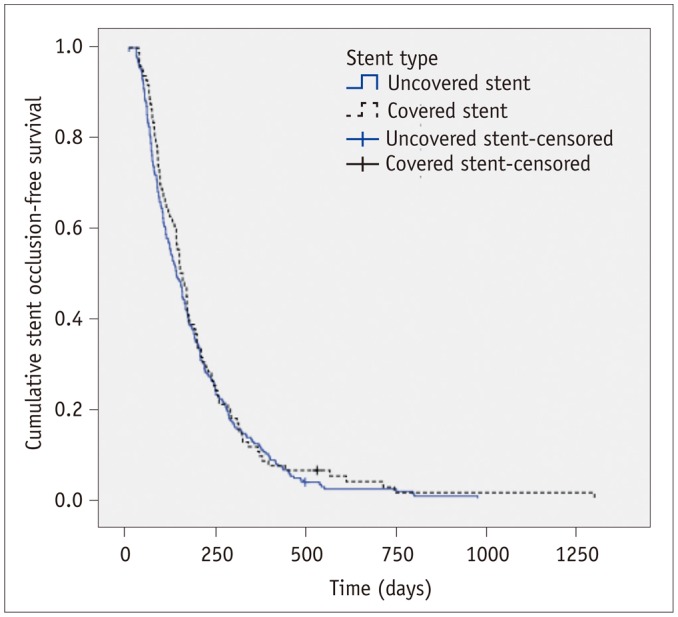
The median patient overall survival was 212 days (95% confidence interval [CI], 186−237 days) for all 318 patients. There were no significant statistical differences in overall patient survival between the unilateral and bilateral stent groups (adjusted hazard ratio; 0.964 [95% CI = 0.741−1.256] with a baseline of unilateral stenting, p = 0.788) (Fig. 2). Overall patient survival was not significantly different for a covered stent as compared with uncovered stents (adjusted hazard ratio; 0.795 [95% CI = 0.611−1.034] with the baseline of uncovered stent, p = 0.087) (Fig. 3). The median stent occlusion-free survival was 141 days (95% CI, 126−156 days) for all 318 patients. In terms of stent occlusion-free survival. There were no significant differences between the unilateral and bilateral stent groups (adjusted hazard ratio; 1.062 [95% CI = 0.817−1.381] within the baseline of unilateral stenting, p = 0.653) (Fig. 4) or the uncovered and covered stent groups (adjusted hazard ratio; 0.952 [95% CI = 0.733−1.236] with the baseline of uncovered stent, p = 0.709) (Fig. 5) was detected.
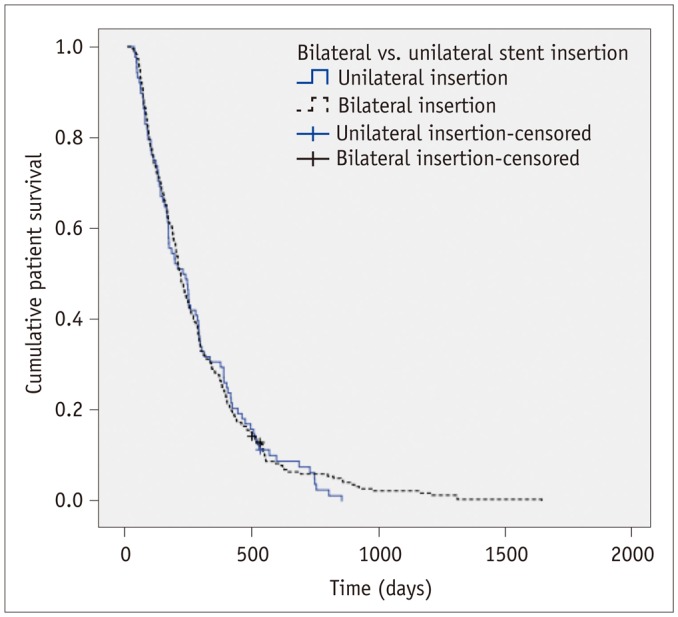 | Fig. 2Comparison of overall patient survival between unilateral and bilateral stent placement groups (adjusted hazard ratio; 0.964 [95% CI = 0.741−1.256] with baseline of unilateral stenting, p = 0.788).CI = confidence interval
|
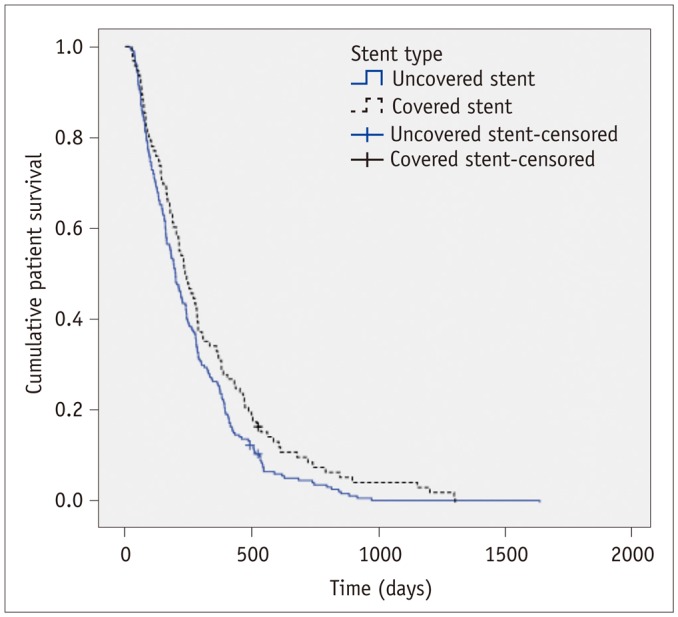 | Fig. 3Comparison of overall patient survival between covered and uncovered stent groups (adjusted hazard ratio; 0.795 [95% CI = 0.611−1.034] with baseline of uncovered stent, p = 0.087).
|
Causes of Obstruction
Stent dysfunction was observed in 107 (48.2%) of 222 patients after a mean of 177 days in the uncovered stent group and in 47 (49.0%) of 96 patients after a mean of 195 days in the covered stent group. Uncovered stent dysfunction was caused by tumor ingrowth (n = 102), sludge incrustation (n = 1), tumor overgrowth (n = 1), severe kinking of the common bile duct just distal to the stent (n = 1), hemobilia (n = 1), and food impaction (n = 1). Dysfunction of the covered stents were caused by sludge incrustation (n = 43) and tumor overgrowth (n = 4). No tumor ingrowth occurred in the covered stent group, whereas it occurred in 103 patients in the uncovered stent group. The incidences of tumor ingrowth and sludge incrustation between the covered and uncovered stent groups were significantly different (p < 0.0001). Among the 154 patients with stent dysfunction, 108 were managed utilizing an external drainage catheter due to their rapidly progressing disease, 31 were managed by placement of an additional stent via percutaneous (n = 25) or endoscopic (n = 6) routes, and 10 patients received an endoscopic nasobiliary catheter. The remaining five patients were managed conservatively due to their advanced disease stage.
Go to :
DISCUSSION
In the present study, we found that the technical success rate (100%), complication rate (13%), and successful internal drainage (89.1%) were in accordance with the results of other studies involving the placement of percutaneous or endoscopic metallic stents in patients with advanced hilar malignancies (21112). In prior studies, the technical success rates ranged from 98% to 100%, the overall complication rates ranged from 0% to 33%, and the successful internal drainage rates ranged from 75% to 100% (21112). We observed a median overall survival time of 212 days, which was similar to previously reported 193–319 days (21112). Likewise, the observed median stent occlusion-free survival time of 141 days was similar to the 130–192 days reported previously (21112). After the introduction of a fine needle (more than 21 gauge) and guidance by ultrasonography or fluoroscopy, the success rate of PTBD was nearly 100%, even in patients who had advanced biliary obstruction (type IV). Adequate biliary drainage can improve cholangitis and associated swelling. The subsequent guidewire passage through the obstruction can be achieved by repetitive trials. Thus, a high technical success rate of stent placement can be reasonably achieved.
In the present study, we found no significant differences in the technical success rates (100% in the unilateral stent group and 100% in the bilateral stent group; p > 0.999), the complication rates (8% in the unilateral stent group and 15% in the bilateral stent group; p = 0.065), or in the rate of successful internal drainage (89.1% in the unilateral stent group and 89.9% in the bilateral stent group; p = 0.811). However, the stent occlusion-free survival and overall survival times were not different between the two groups (stent occlusion-free survival, adjusted hazard ratio; 1.062 [95% CI = 0.817−1.381] with the baseline of unilateral stenting, p = 0.653; overall survival, adjusted hazard ratio; 0.964 [95% CI = 0.741−1.256] with the baseline of unilateral stenting, p = 0.788). In patients with MBHO, the advantages of unilateral versus bilateral stent placement remains unclear (5101112). The insertion of a single biliary stent in one functional liver lobe, to allow unilateral drainage, could provide adequate palliation for most patients with MBHO (78917). Moreover, the advocates of unilateral drainage insist that severely atrophic lobes, resulting from longstanding cholangitis, or non-functioning lobes due to portal vein obstruction do not require drainage if there are no symptoms of cholangitis (18). A lobe with a portal vein obstruction was thought to cease producing of bile juice due to an interruption in enterohepatic circulation (7919). Previous investigators reported that biliary decompression of a lobe, with a portal vein occlusion neither reversed atrophy nor improved its function (920). Other authors have recommended that unilateral drainage in a lobe with a patent portal vein can be performed in patients with contralateral portal vein occlusion caused by advanced hilar malignancies (5717). Nonetheless, in some patients, bilateral stenting may be the best option for the drainage of both liver lobes when both sides are contaminated or if chemotherapy is scheduled. However, bilateral stenting requires more steps than unilateral stenting. In the present study, we found the stent configuration did not significantly affect technical success, complications, successful internal drainage, stent occlusion-free survival, or overall survival. For bilateral drainage, T-configured stenting might be preferable unless technical difficulties necessitate crisscross- or Y-configured stenting (2122). Moreover, crisscross- or Y-configured stenting requires additional contralateral PTBD and may introduce a greater chance of PTBD-associated complications (12).
In the present study, we found no significant differences in the technical success rates (100% in the uncovered stent group and 100% in the covered stent group; p > 0.999), and rates of successful internal drainage (89.3% in the uncovered stent group and 90.2% in the covered stent group; p = 0.793). Although the complication rate was significantly higher in the covered stent group (5.8% in the uncovered stent group and 30.9% in the covered stent group; p < 0.001), all patients recovered with appropriate management without follow up problems. Recently, the use of PTFE-covered stents were found to be an effective treatment method because the PTFE material serves as a barrier and prevents tumor ingrowth (13). A few previous studies reported the use of PTFE-covered stents for the palliative treatment of MBHO was technically safe and potentially clinically effective (14152324). Although there is a risk of occlusion in the branching ducts, including the side branches of the bile ducts or the cystic duct, prior studies reported that patients with branching duct blockage, caused by a covered stent, did not exhibit a significant increase in serum bilirubin levels or cholangitis.
In the current study, we also found no significant differences between the uncovered and covered stent groups in terms of complications such as cholangitis or cholecystitis. In a comparative study, PTFE-covered stents were significantly superior to uncovered stents in terms of stent occlusion-free survival (24). However, in the present study, the durations of stent occlusion-free survival were not different between the two groups (adjusted hazard ratio; 0.952 [95% CI = 0.733−1.236] with the baseline of uncovered stent, p = 0.709). Moreover, multivariable Cox regression analysis revealed no significant differences in the overall patient survival between uncovered and covered stent groups (adjusted hazard ratio; 0.795 [95% CI = 0.611−1.034] with the baseline of uncovered stent, p = 0.087).
In the Cox regression analysis, stent occlusion was the only factor that significantly influenced overall survival (adjusted hazard ratio; 0.484 [95% CI = 0.384−0.610] with the baseline of non-occlusion, p < 0.001). Our results are consistent with those of previous studies. Li et al. (25) reported that reintervention after occlusion improved the survival of patients. Hyun et al. (15) claimed that underlying liver function was important and that stent patency significantly correlated with survival. Generally, stent occlusions are not an advantageous events for overall survival. It can be postulated that patients with long term survival transcend stent occlusion-free survival, and survival may be more dependent on the underlying liver function. Thus, obtaining optimal biliary drainage is more important than Bismuth type, stent type, or configuration to prevent a septic crisis and to improve the patient's overall quality of life.
The present study had several limitations. The retrospective design and the restriction of the study population to a single center limited the clinical significance; however, this study is the largest of its type to date. Also, due to the retrospective design, we had no fixed algorithm for the treatment of MBHO. However, because differences among the metallic stents might have influenced the outcomes, additional prospective comparisons are needed.
In conclusion, percutaneous metallic stent placement can be technically safe and effective for internal drainage in patients with MBHO. In addition, the stent type and configuration used may not significantly affect the technical or clinical outcomes.
Go to :
 XML Download
XML Download