

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Postpartum hemorrhage (PPH) is defined as blood loss > 500 mL within 24 hours after vaginal delivery or > 1000 mL after cesarean delivery and is a potentially life-threatening condition (1). Primary PPH appears during the first 24 hours after delivery and secondary PPH occurs for more than 24 hours and up to 12 weeks after delivery (2).
Regardless of the mode of delivery, severe PPH is defined as life-threatening blood loss with one or more of the following events related to the blood loss: blood transfusion; transcatheter arterial embolization (TAE); arterial ligation; other conservative uterine surgery; hysterectomy; transfer to an intensive care unit, peripartum hemoglobin reduction of 4 g/dL or more (considered equivalent to the loss of 1000 mL or more of blood), or maternal death (3). PPH and severe PPH represent 6% and 1.86% of all deliveries, respectively (45); however, PPH is often underestimated due to the difficulties in estimating the blood loss and missed instances of bleeding in patients with intra- or retroperitoneal bleeding or vaginal hematoma. Severe PPH causes approximately 25% of the maternal deaths worldwide (5).
Conservative management of PPH includes resuscitation, blood transfusion, and administration of uterotonic drugs such as oxytocin and prostaglandin, uterine compression, and intrauterine balloon tamponade. When conservative management fails, TAE or surgical management is implemented without any delay. Surgical management includes vessel ligation (bilateral ligation of the uterine or internal iliac arteries), uterine compression suture, and hysterectomy (4).
It is widely accepted that TAE is an effective therapeutic strategy for PPH of various causes (6). TAE has the advantage of being a fast, repeatable procedure and can be performed without general anesthesia. Moreover, TAE preserves the uterus and makes future menstruation and fertility possible. In the present work, we review the current literature regarding vascular anatomy relevant to PPH, technical considerations and outcomes of TAE, and a detailed review of every single specific clinical setting.
Go to : 
Vascular Anatomy Relevant to PPH
Precise knowledge of the normal and varying anatomy of the female genital tract is essential for accurate interpretation of angiographic images and safe performance of PPH embolization. The internal iliac artery (IIA) divides into two divisions (Fig. 1, Table 1). The anterior division of the IIA is subject to numerous variations and gives rise to the umbilical, superior vesical, obturator, inferior vesical, vaginal, middle rectal, internal pudendal, inferior gluteal, and uterine arteries (UAs). The posterior division of the IIA gives rise to iliolumbar, lateral sacral, and superior gluteal arteries.
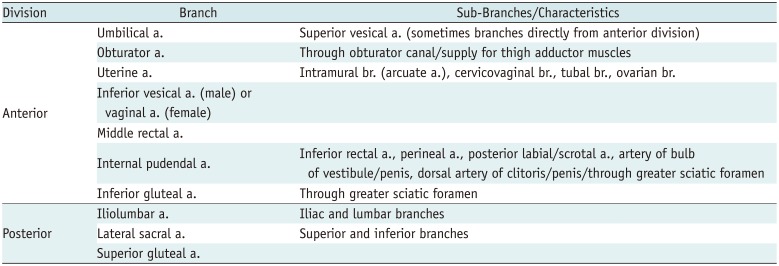
 | Fig. 1Vascular anatomy relevant to PPH.
A. Schema of IIA and its branches. 1, common iliac artery; 2, external iliac artery; 3, inferior epigastric artery; 4, IIA; 5, superior vesical artery; 6, obturator artery; 7, UA; 8, internal pudendal artery; 9, inferior gluteal artery; 10, superior gluteal artery; 11, lateral sacral artery; 12, iliolumbar artery; 13, piriformis muscle; and 14, sacrospinous ligament. B. Left IIA arteriogram in right anterior oblique projection (20°). 1, IIA; 2, external iliac artery; 3, lateral sacral artery; 4, UA; 5, inferior gluteal artery; 6, internal pudendal artery; 7, obturator artery; 8, vesical artery; 9, superior gluteal artery; and 10, iliolumbar artery. IIA = internal iliac artery, PPH = postpartum hemorrhage, UA = uterine artery
|
Table 1
Division, Branches, and Characteristics of Internal Iliac Artery
![]()
The UA shows the characteristic U-shaped course and consists of a descending or parietal segment, a transverse or arch segment, and an ascending or marginal segment which runs along the uterine side and has numerous intramural branches (arcuate arteries) (Fig. 2). The cervicovaginal branch arises from the transverse segment and supplies blood to cervix and vagina (7). Ovarian and round ligament arteries often participate in a complex anastomotic network that provides blood supply to the uterus (8). The ovarian artery arises from the abdominal aorta below the renal artery, and the round ligament artery originates from the inferior epigastric artery (8). Collaterals to the uterus from the ovarian artery, inferior mesenteric artery, round ligament artery, and internal pudendal artery are well-known and can be a bleeding source in PPH (79).
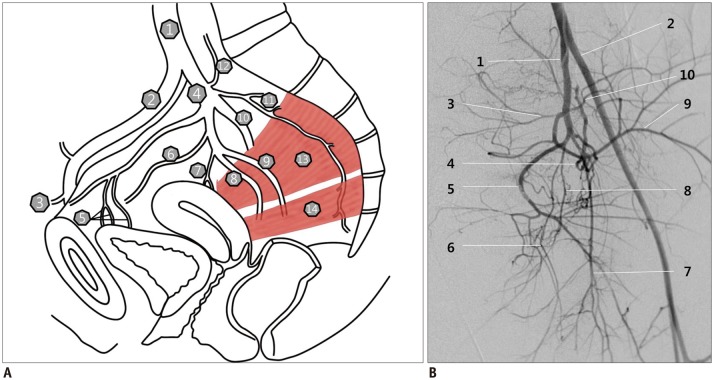
 | Fig. 235-year-old woman with primary PPH due to uterine atony.
A. Left internal iliac arteriogram in frontal projection shows typical tortuous shape of UA (arrows). B. Selective arteriogram of left UA shows enlarged UA (arrow) which supplies enlarged uterus with numerous intramural branches (arcuate arteries, arrowhead). Cobra catheter (white arrows) was used to catheterize contralateral left UA (inset). C. Right internal iliac arteriogram in frontal projection demonstrates tortuous, enlarged UA with characteristic descending (arrowhead), transverse, and ascending segments (arrow). Ipsilateral, right UA was selected with Cobra catheter using Waltman loop (white arrows in inset). Bilateral UAs were embolized using gelatin sponge particles (not shown). D. Completion arteriogram shows no visualized bilateral UAs.
|
The vaginal artery arises from the anterior division of the IIA just below the origin of the UA or from the UA and supplies blood to the anterior and lateral surface of the vagina (10). Branches from the inferior vesical artery supply blood to the middle portion of the vagina, and the internal pudendal artery supplies to its lower portion, the posterior surface being vascularized by the middle rectal artery. Therefore, branches from internal pudendal or rectal arteries can be a bleeding focus when vaginal laceration occurs due to the presence of a complex arterial network on the borders of the vagina, uterus, and adnexa (11).
A persistent sciatic artery is a rare vascular anomaly with a high potential risk to cause irreversible ischemic damage of the lower limb during TAE for PPH (12). The persistent sciatic artery starts at the IIA and runs through the greater sciatic foramen, from where its course becomes closer to the sciatic nerve (13). Distally, the artery lies deep in the major gluteal muscle and follows a course along the adductor magnus muscle. Finally, the sciatic artery reaches the popliteal artery running through the popliteal fossa, lateral to the insertion of the adductor magnus muscle (13). If a persistent sciatic artery exists during the procedure to control PPH, it is important to prevent the reflux of the embolic materials, which can cause ischemic damage of the lower limb. In one report, TAE for PPH was canceled in one case with bilateral persistent sciatic artery because UAs could not be superselected successfully and subsequently, hysterectomy was performed (12).
Go to :
Transcatheter Arterial Embolization
Technical Consideration
The common femoral artery is accessed using the Seldinger technique either with palpation/fluoroscopy or by ultrasound guidance. Ultrasound guidance is particularly useful in women with small-diameter femoral arteries secondary to hemodynamic instability. A single puncture of the right common femoral artery allows catheterization of both the pelvic arteries using a Waltman loop with a 5 Fr Cobra (Cook, Bloomington, IN, USA) (Fig. 2). A Roberts Uterine Catheter (Cook) can be used to catheterize either contralateral or ipsilateral IIA. Usually, the contralateral anterior oblique view (approximately 30 degrees) after the anterior-posterior view is recommended in order to delineate the location of the anterior division of the IIA or UA (14). Commonly, the UA can be cannulated using a 5 Fr catheter as the UA is almost always hypertrophied given the enlarged uterus and recent postpartum state. A microcatheter is usually used for superselection of the transverse or ascending segments of the UAs (1516), although the position of the microcatheter depends on the underlying vascular condition and the patient's hemodynamic status. It is often necessary to skip deeper catheterization for speeding up the setting of hemodynamic instability, and nonselective embolization of the anterior division of IIA may be necessary. Arteriograms of bilateral IIAs are basically necessary to identify the UAs on both the sides as well as any other potential sites of bleeding. Aortography is needed to identify other potential bleeders, such as ovarian arteries, in patients with persistent or recurrent bleeding after embolization of bilateral UAs and IIAs.
The general rule regarding the embolization of bleeding arteries is 1) embolization of bilateral UAs regardless of the presence of active bleeding foci; 2) embolization of the anterior divisions of bilateral IIAs in case the UA could not be easily accessed, e.g., in patients with hysterectomy or hemodynamic instability, or when bilateral UA embolization fails to stop bleeding; 3) embolization of other potential bleeders (Table 2) based on additional angiography or aortography if bilateral UA and IIA embolization fails. These anastomotic arteries, especially the ovarian artery and the round ligament artery, have an important role in rebleeding (1718).
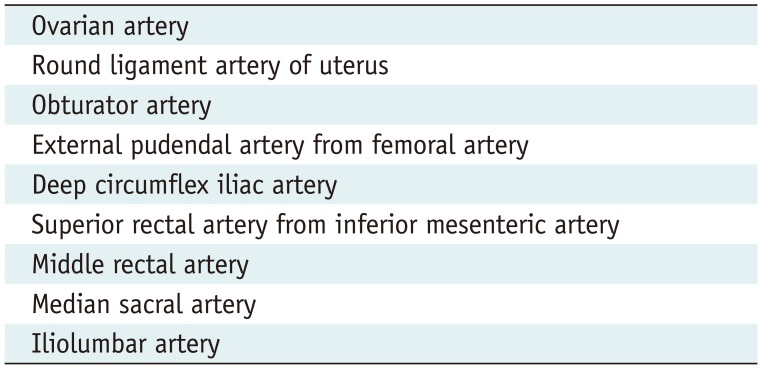
Table 2
Possible Anastomotic Arteries Causing PPH Other than UA
![]()
Active extravasation of the contrast medium, pseudoaneurysms with or without extravasation of contrast medium, and abruptly cutoff vessels are considered to represent active bleeding foci (19). Extravasation does not necessarily indicate more severe hemorrhage, and negative findings on angiography do not exclude bleeding (20). Completion angiography of bilateral common iliac arteries or aortography is recommended to cover all possible bleeding foci. The exact judgment of cessation of bleeding after TAE is possible with on-site speculum examination.
The complication rate attributable to TAE is really low. The complication rate of both primary PPH and secondary PPH is about 4.0% (11192021). The major complications reported include lower extremity deep vein thrombosis, hemoperitoneum related to dissection of IIA, endometritis, zonal ischemic necrosis of the inner half of the myometrial wall, and uterine necrosis. Minor complications include postembolization syndromes (transient fever, mild leukocytosis, and abdominal pain), altered menstruations (heavier menses, lighter menses, and dysmenorrheal), dissection of the UAs, transient buttock/foot ischemia, and puncture site hematoma (11202122).
Timing of Embolization
The major factor in the adverse outcomes associated with primary PPH is a delay in appropriate management (23). After the first-line treatment, such as removal of traumatic factors, i.e., uterine rupture or genital tract laceration, blood transfusions, uterotonic drug administration, and uterine compression, an interventional radiologist should be involved at the time when abnormal bleeding is observed, regardless of the severity of PPH, as embolization is a useful and important treatment option for any type of PPH.
As surgical ligation of the UAs or IIAs often fails to stop the bleeding due to potential collateral circulation (2425) and emergency hysterectomy is associated with high mortality with loss of fertility (26), TAE should be considered as the first-line hemostatic measure for patients when TAE is promptly available or if the patient can withstand transportation to a hospital where TAE is available. Hemodynamic instability should not be considered as a contraindication for TAE (19). Repeat embolization should also be considered before performing hysterectomy because of its advantage in achieving hemostasis without sacrificing the reproductive ability of the patient (19). The performance of TAE at an earlier stage provides the advantage of reducing blood loss and easy subsequent surgery with a clear field of vision (27).
If there is massive bleeding from a placental abnormality, it is ideal to consider TAE immediately in the operating room. An emergency procedure of prophylactic balloon catheter occlusion at the level of the common iliac arteries can maintain hemodynamic stability during hysterectomy or TAE (2829).
Because a significant portion of PPH-related maternal morbidity may be prevented through early diagnosis and rapid intervention, it is recommended to develop multidisciplinary algorithms and rapid-response teams in order to optimize the outcomes of PPH (30). The use of protocols and hemorrhage drills extends beyond the obstetric teams alone and are dependent on the successful collaboration of providers from numerous disciplines, including interventional radiology, and may reduce the morbidity and mortality associated with PPH (31).
Embolic Materials
The choice of embolic materials depends on the combination of angiographic findings, achievable catheter position, and the operator preference.
Gelatin sponge particles are the most commonly used primary embolic material for PPH embolization. Gelatin sponge particles are mixed with diluted contrast medium to produce a slurry, which is subsequently injected into the arteries until stasis or occlusion of blood flow is evident during angiography (22). They enable temporary occlusion for 3–6 weeks and recanalization of the target arteries which is advantageous for future fertility (6). However, TAE with gelatin sponges as the sole embolic material in patients with coagulopathy has been reported to limit the effectiveness in achieving successful hemostasis (32). In addition, in patients with active bleeding, such as in patients with a pseudoaneurysm, use of a gelatin sponge may be inadequate for effective treatment (1533).
The use of N-butyl cyanoacrylate (NBCA) should be considered in patients with 1) active bleeding, i.e., contrast extravasation or a pseudoaneurysm, 2) hemodynamically unstable conditions, or 3) failed embolization with gelatin sponge particles (usually at the repeated session of embolization) (Figs. 3, 4). The mechanism of NBCA embolization involves rapid polymerization by making contact with blood and complete blocking of arterial injury/filling the pseudoaneurysm, and thus providing effective embolization regardless of coagulopathy. Therefore, emergency TAE using NBCA can be a beneficial first-choice treatment for PPH with disseminated intravascular coagulation (DIC), extravasation or pseudoaneurysm (1534). In patients with DIC, employment of NBCA in the distal UA, but not in the far distal to the myometrium would be a better option to reduce the possibility of rebleeding secondary to the opening of unusual collateral supply to the uterus.
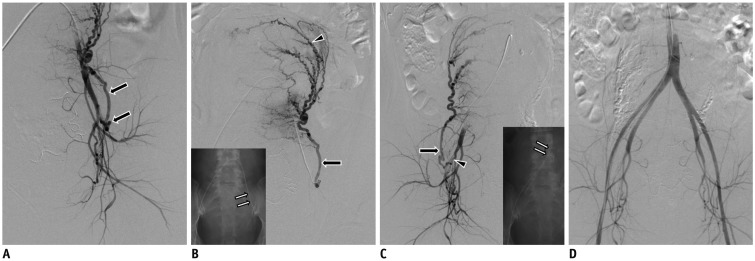
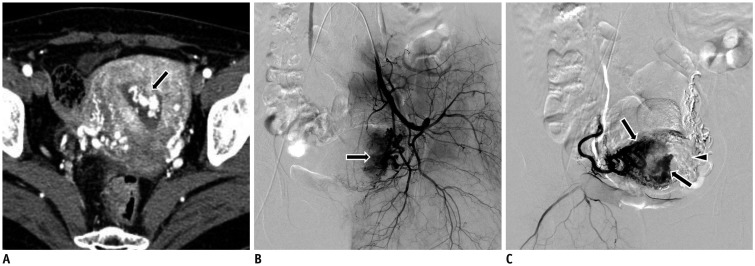
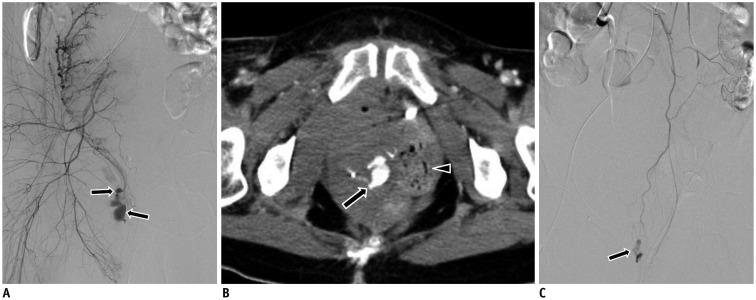 | Fig. 334-year-old woman with primary PPH three hours after vaginal delivery.There was vaginal laceration, which could not be controlled with vaginal packing and suture.
A. Initial, right internal iliac arteriogram shows contrast extravasations (arrows) in vaginal branches from anterior division of IIA. Several bleeders, including vaginal branches, were embolized with NBCA and microcoil, after which bilateral UAs were embolized with gelatin sponge particles (not shown). However, persistent contrast extravasation was noted. Therefore, right IIA was embolized with gelatin sponge particles (not shown). B. Vaginal bleeding recurred four hours later. Axial contrast-enhanced CT scan shows active bleeding (arrow) in right paravaginal hematoma. Note vaginal packing (arrowhead). C. In second session, aortogram demonstrates contrast extravasation at lower pelvis level. Subsequent, selective inferior mesenteric arteriogram shows contrast extravasations (arrow) in distal branch which was embolized with NBCA (not shown). NBCA = N-butyl cyanoacrylate
|
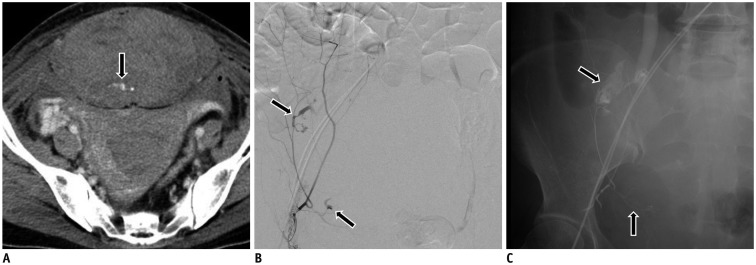 | Fig. 440-year-old woman with decreased hemoglobin level following cesarean section.However, obvious vaginal hemorrhage was not found.
A. Axial enhanced CT scan shows large hematoma with active bleeding focus (arrow) within rectus abdominis muscle. Small amount of hematoma is found in endometrial cavity without active bleeding. B. Selective left inferior epigastric arteriogram demonstrates no active bleeding. However, subsequent, selective right inferior epigastric arteriogram demonstrates contrast extravasation (arrows). C. Completion, fluoroscopic image shows NBCA cast (arrows) of right inferior epigastric artery. Additional angiogram of right superior epigastric artery demonstrates no active bleeding focus.
|
General Outcomes of TAE
Both primary and secondary PPH can be life-threatening, although primary PPH is more associated with urgency and maternal mortality. Patients with secondary PPH appear to be hemodynamically stable and receive fewer transfusions than patients with primary PPH (1936). Differences in etiologies, angiographic findings, and technical and clinical success are summarized in Table 3. Although pseudoaneurysm of the UA is known to be a rare cause of delayed PPH (33373839), it is highly associated with secondary PPH in up to 23% of the initial angiograms (36).
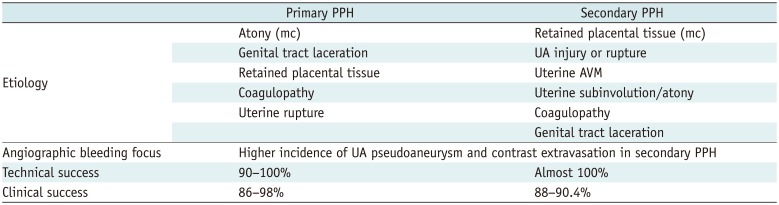
Table 3
Differences of Primary and Secondary PPH
![]()
When PPH cannot be effectively controlled using conservative management, TAE or a surgical procedure should be considered. During primary PPH, TAE is preferably performed when PPH occurs after vaginal delivery (4). Ligation is the recommended first-line option for PPH during cesarean section; while TAE should be strongly considered when PPH occurs after completion of the cesarean section (7). During secondary PPH, TAE is recommended as the first-line option regardless of the method of delivery.
Clinical success involves many clinical factors, such as the transfer time, cooperation of the obstetrician and interventional doctor, and detailed management for DIC and placental abnormality. Currently, although the clinical success rate ranges from 86.5% to 95.0%, it is hypothesized that with the improvement of many factors related to clinical success, enhancement in the effect of TAE for PPH can be achieved (1922). Factors more frequently found in failed embolization include DIC, hemodynamic instability, a hemoglobin level below 8 g/dL, and extravasation detected on angiography (40).
Effects on Menstruations and Fertility
The most important advantage of TAE is that it preserves a woman's uterus and childbearing potential compared with hysterectomy, and menstruation and fertility do not seem to be affected by TAE (4142); resumption of a regular menstrual cycle was demonstrated in 97.3% of 251 patients (19), and no significant difference with regard to fertility was reported between patients who underwent TAE for severe PPH and those who did not (43).
Radiation Exposure
Since the ovaries are usually in the direct path of the radiation beam and cannot be shielded throughout TAE for PPH, the radiation dose to the ovaries is high. One report demonstrated a mean estimated absorbed radiation dose of up to 58.6 cGy (range: 20–73 cGy) for an ovary in TAE (44). There has been, however, no report of TAE induced skin reactions, or children being born with malformations. Exposure to radiation during TAE also depends greatly on the procedure protocol (45). To decrease the radiation dose, repeat digital subtraction angiography, magnification fluoroscopy, the field of view, pulse rate frequency, fluoroscopy time, and the distance between the patient and image intensifier should all be minimized (4647).
Go to :
Specific Clinical Settings
Uterine Atony
Uterine atony is found in 70–80% of PPH and is the best indication for preferring TAE as the first-line measure (48). Angiography shows dilated uterine and arcuate arteries which extend cephalad to the aortic bifurcation (Fig. 2). Bleeding was usually reported to be diffuse with rarely visible extravasation of contrast material (7). Gelatin sponge particles are the preferred and sufficient embolic materials when coagulopathy is not associated.
Genital Tract Laceration
Lacerations of the genital tract are responsible for approximately 8–20% of PPH, alone or in association with atony, and for a still higher rate in primary and severe PPH (419). Conventional suture and packing methods are generally first performed for hemostasis in genital tract laceration, however, TAE can stop the bleeding and provide a clear visual field when repairing the trauma (49).
Angiography, including that of the pelvic floor vasculature, can be helpful to quickly assess vascular injury when a laceration is anticipated based on the delivery history and at instances when the location is unclear (14). A contrast-enhanced CT scan is also helpful for determining the amount and location of a hematoma and for detecting bleeding arteries, and thus subsequently facilitating catheterization and reducing the procedure time (Fig. 3).
The most frequently injured arteries are the uterine, vaginal, and internal pudendal arteries (3749), which manifest as a pseudoaneurysm and/or contrast extravasation. Rupture of a pseudoaneurysm may occur late as a secondary PPH (36), during which NBCA is the preferred embolic material as it makes a solid filling cast and occludes the artery.
Placental Abnormality
Placental abnormalities representing placental implant anomalies, such as placenta previa and placenta accreata/increta/percreta, are on a continuous rise secondary to the increasing incidence of cesarean sections. Remaining placental tissue prevents adequate contraction and predisposes the patient to excessive bleeding due to secondary, spontaneous placental detachment and recruitment of the blood supply from adjacent collaterals (750). Different approaches have been reported, including prophylactic sheath/catheter placement with or without TAE after delivery, balloon occlusion with or without TAE after delivery or TAE after delivery (50515253).
Prophylactic balloon catheter occlusion during delivery can maintain the hemodynamic stability during hysterectomy or TAE; however, it seems not so promising because of the potential vascular complications and questionable effectiveness in reducing blood loss due to extensive collateral circulation to the uterus (5052). Prophylactic embolization of IIA or UA before delivery is controversial as this results in a number of unnecessary catheter placements, potential vascular complications, and radiation exposure, while TAE immediately or on-demand after delivery seems to reduce the risk of PPH, be effective in bleeding control, and increases the chance of uterine preservation (5053).
Angiography shows dilated vascular channels scattered throughout the remaining placenta, thus suggesting trophoblastic vascularization primarily from the UA (50) (Fig. 5). Collateral blood supply other than that of the UA, such as that of the ovarian artery (Fig. 5), vesical artery or internal pudendal artery, can contribute in supplying blood to the placenta. TAE has shown a success rate of approximately 80% (50), with only 20% of women requiring further surgery and hysterectomy (5054). Gelatin sponge particles have been reported to have been used in a majority of the previously published reports (50555657).
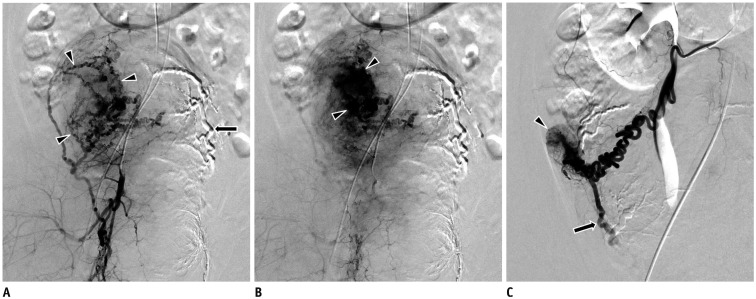 | Fig. 539-year-old woman with placenta accreta, presenting with PPH after cesarean section.
A, B. Early and delayed, right internal iliac arteriograms show multiple, tortuous UA branches (arrowheads in A) and extensive trophoblastic vascularization of placental intervillous spaces (arrowheads in B). Note embolized left UA with gelatin sponge particles (arrow). There was continued vaginal bleeding after bilateral UAs embolization with gelatin sponge particles. C. Selective, right ovarian artery angiogram shows reflux into UA (arrow). Faint ovarian blush (arrowhead) is also visible. Right ovarian artery was embolized with gelatin sponge particles.
|
Uterine Arteriovenous Malformation
Unlike idiopathic (or primary) uterine arteriovenous malformation (AVM) which has developmental anomalies, acquired (or secondary) AVM is a condition associated with delivery or surgical procedures (58). Therefore, uterine AVM is one of the etiologies of secondary PPH and manifests as unexpected, excessive, and intermittent bleeding after delivery (59).
Bilateral UAs are usually found to be feeding arteries. Angiography shows hypertrophied UAs into the AVM and early drainage from the AVM to pelvic veins (Fig. 6). Preprocedural imaging is helpful for evaluating possible extra-uterine feeders (58). Embolization of bilateral UAs by gelatin sponge particles is the first-line therapy (5860).
 | Fig. 633-year-old woman with arteriovenous malformation, presenting with secondary PPH after cesarean section.
A. Arterial phase of axial enhanced CT scan shows hypervascular lesion (arrow) in uterine cavity. B. Left internal iliac arteriogram shows hypervascular lesion (arrow) with enlarged tortuous UA. C. Selective angiogram of right UA shows hypervascular lesions (arrows) and parenchymal defect (arrowhead) due to embolization of left UA. Bilateral UAs were embolized with gelatin sponge particles.
|
PPH after Cesarean Section
Women with PPH following cesarean section constitute 26–44% of the women treated with TAE (1961). After cesarean section, injuries to pelvic arteries, uterine atony or placental abnormality are etiologies of primary PPH, while spontaneous pseudoaneurysm rupture frequently causes secondary PPH. TAE should be considered while the woman is out of the operating room (6), and cesarean delivery is no longer a predictor of poorer outcomes after TAE, compared with vaginal delivery (11192062).
Angiography shows a higher incidence of pseudoaneurysm or contrast extravasation from the uterine, vaginal or internal pudendal artery caused by injury or laceration related to cesarean section, compared with vaginal delivery (113744). Cesarean section is the major cause of pseudoaneurysm of the UA (63).
When patients complain of abdominal pain and have reduced hemoglobin level but not obvious vaginal hemorrhage, post-cesarean hemoperitoneum, and abdominal wall hematoma should be considered (64). The inferior epigastric artery is usually responsible for the condition and overlooked as an atypical hemorrhage source (65) (Fig. 4).
Rebleeding after TAE
The rebleeding rate after TAE has been reported to range from 5.2% to 13.5%, despite its technical success (194066). The main reason for rebleeding after TAE is recanalization of embolized arteries, followed by the opening of the collateral communications (Fig. 3) (79). In addition to confirmation of UA recanalization, search for the presence of spontaneous arterial anastomoses, such as the round ligament artery (Fig. 7), ovarian artery, middle rectal artery or inferior mesenteric artery, is necessary on the angiography in search of rebleeding (17).
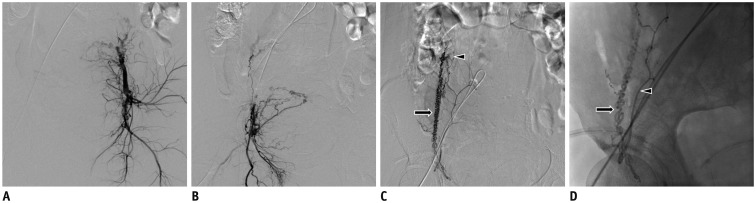 | Fig. 738-year-old woman with vaginal bleeding after cesarean section.
A, B. Bilateral internal iliac arteriogram in frontal projection shows hypertrophied bilateral UAs. However, vaginal bleeding was persistent after adequate embolization of both UAs using gelatin sponge particles. C. Pelvic aortography demonstrates right round ligament artery (not shown). Selective angiography of right round ligament artery (arrow) shows uterine stains (arrowhead). D. Image obtained during embolization shows right round ligament artery (arrow) and right inferior epigastric artery (arrowhead) filled with mixture of contrast medium and gelatin sponge particles. Embolization was performed at level of inferior epigastric artery because of failure of superselection of round ligament artery. Vaginal bleeding ceased after right round ligament artery embolization.
|
Application of CT
Multidetector CT plays an important role when intra-abdominal bleeding is suspected and can be considered in cases of rebleeding after TAE, as well as during evaluation of postsurgical complications (67). CT can provide information on detection, localization, and characterization of PPH in some difficult cases; although it is not recommended to routinely obtain CT scan in patients with PPH (68). Scanning range is from the infrarenal aorta to the femoral bifurcation after determining the location using a scout digital radiograph.
Early arterial, late arterial, and venous phase scanning are performed at a fixed delay of 8, 20, and 90 seconds, respectively. Volumetric data from the infrarenal aorta to the femoral bifurcation are acquired in the craniocaudal direction. Semitransparent volume-rendering images and maximum intensity projection images from each volume are generated in frontal and oblique views at 30-degree intervals, rotating 180° (69). CT is less invasive, less time-consuming and more sensitive than angiography in the detection of active bleeding (7071). Knowledge of the various radiologic appearances of PPH and the correlation with clinical information can ensure correct diagnosis and appropriate and prompt treatment planning in the patients with PPH (72).
Go to :
CONCLUSION
It is recommended that TAE should be considered as the first-line therapy to control PPH due to its characteristics of fast pace, excellent effect, wide indication, minimal invasiveness, and uterine preservation. Gelatin sponge particles are the primary embolic material used in PPH embolization; however, NBCA or metallic coils are also frequently used for active bleeding or as bailout materials for failed TAE with gelatin sponge particles. Close communication among the obstetrician and the interventional radiologist is also essential to avoid the delay in performing TAE.
Go to :
 XML Download
XML Download