

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
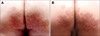
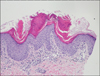
A 58-year-old man with no specific medical comorbidities presented with an 8-year history of pruritic oozing plaques on the buttocks and perianal area. Clinical inspection of the buttocks and perianal region showed symmetric, irregular but sharply demarcated, red- to brown-colored verrucous and hyperkeratotic plaques with marginal induration and scales (Fig. 1A). Because the clinical features were suspicious for tinea corporis, a direct fungal smear was performed; it was positive for fungal hyphae. Oral terbinafine and topical sertaconazole were used to control the superficial fungal infection for 4 weeks. However, the response to treatment was poor, so treatment was switched to oral itraconazole, fluconazole and topical flutrimazole cream. After 8 weeks of treatment, the plaque showed slight decrease in scaling and pruritus was improved, but the overall response for the treatment was unsatisfactory. Alternative diagnoses such as psoriasis or porokeratosis were suspected, so punch biopsy of the lesions was performed. H&E staining revealed slight acanthosis and multiple parakeratotic column with disappearance of the granular layer underneath (the cornoid lamella), characteristic histologic findings of porokeratosis ptychotropica (Fig. 2). On the basis of these clinical and histologic features, a diagnosis of porokeratosis ptychotropica was established, and topical calcipotriol was administered. The verrucous lesions slightly improved with an appearance resembling typical porokeratosis of Mibelli with a prominent porokeratotic border after 6 weeks of treatment (Fig. 1B).
Porokeratosis represents a heterogeneous group of disorders of keratinization characterized by atrophic lesions with a prominent ridge-like border and histological features of colloid lamella. Several variants of porokeratosis have been described. When the perianal and gluteal regions are involved, this localized form is referred to as porokeratosis ptychotropica, a rare variant of porokeratosis12. Multiple cornoid lamellae, as seen in this case, are a characteristic finding of this unique form. Various treatment options have been used in previous publications345. Topical steroids provided symptom relief, but various treatments including systemic, topical agent and physical modalities showed minimal or variable effects. Pitney et al.5 reported similar post-treatment changes to those seen in this case, including a Mibelli-like appearance, and hypothesized that porokeratosis ptychotropica is the end stage of a local proliferation of Mibelli-like lesions associated with koebnerization and/or lichenification.
In conclusion, this case involved a rare entity, porokeratosis ptychotropica. Although diagnosis in this case was delayed due to the coexistence of a superficial fungal infection, this condition is often misdiagnosed, especially in its early stages due to its rarity. To the best of our knowledge, this is only the second report of porokeratosis ptychotropica in the Republic of Korea. We would like to raise awareness of this disease entity so that it is included in the clinical differential diagnosis of perianal and gluteal skin diseases, especially when tinea corporis and psoriasis are suspected.
 XML Download
XML Download