

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
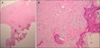
A 27-year-old man presented with a tender nodule on the distal aspect of the right third toe, slowly growing in size over a 2-month period. He had a history of trauma in the right third toe during exercise two months prior to his visit. Initially, the nodule was soft in consistency but with time enlarged in size and became hard. An examination revealed an erythematous, eroded, hard mobile nodule measuring 0.5×0.5 cm in size (Fig. 1). The initial clinical suspicion was that it was a viral wart; thus, a punch biopsy was done. Microscopic examination showed the lesion was multinodular with irregular margins in the dermis. The nodules consisted of a mixture of fibroblasts, mixoid matrix, and focal deposits of osteoid with irregularly distributed osteoblasts (Fig. 2A). The osseous trabeculae were haphazardly distributed without peripheral zoning. The osseous trabeculae were rimmed by proliferated fibroblasts and osteoblasts (Fig. 2B). The diagnosis was confirmed by histopathologic findings as fibro-osseous pseudotomor of the digits (FOPD). The tumor was completely excised, and no connection with the underlying bone was observed. No recurrence was noted during a follow-up period of 6 months.
FOPD is a rare benign ossifying lesion proposed as a unifying term by Dupree and Enzinger1. FOPD may occur anywhere in the body but is most common in the finger, especially in the region of the proximal phalange12. In Korea, only 3 cases of FOPD of the finger and 1 case of FOPD of the toe have been reported. Typically, this lesion affects young adults, mainly women, and presents as a soft tissue mass growing over a period of weeks or a few months2. Pain, tenderness, and functional limitation may be present. The pathogenesis of FOPD is thought to be related to repeated trauma to the area; however, a specific history of antecedent trauma was revealed in a small number of cases1.
The essential histologic features include localization in the subcutaneous tissue without muscular involvement, a disorderly multinodular growth pattern with indistinct borders, and a fibroblastic proliferation showing varying degrees of cellular atypia and haphazardly arranged osseous trabeculae without the zoning phenomenon13. Main pathologic differentials to this entity are myositis ossificans, extraskeletal osteosarcoma, and subungual exostosis. Mysositis ossificans usually occur after trauma, in the deeper aspect of proximal soft tissues and histopathologically show a typical zonation pattern3. Extraskeletal osteosarcoma should always be ruled out; however, it shows destructive stromal invasion, obvious cytologic atypia and immature osteoid directly formed by tumor cells4. Subungual exostosis can appear clinically and histopathologically very similar to FOPD, except for the presence of a connection to the underlying phalangeal bone, the presence of bone marrow tissue, and the feature of an overlying fibro-cartilaginous cap5.
FOPD has an excellent prognosis following complete excision with low risk of recurrence (0%~14%)5. No cases of malignant transformation or metastases are on record15. We report herein a rare and typical case of FOPD of the toe and suggest that FOPD should be considered in the differential diagnosis of any digital mass.

 XML Download
XML Download