

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Achieving natural harmony between implant-prosthetic components and the surrounding soft tissues is challenging for the restorative team. The implant abutment design, its material and color seem to be of decisive importance for ensuring an esthetic mucogingival architecture.12 In the past, there have been two main types of abutments available for restoring implants: conventional titanium stock abutments, traditionally supplied by dental implant manufacturers to match their respective implant system, and custom cast abutments. Recently, novel computer-aided designed (CAD), computer-aided manufactured (CAM) abutments of various materials have been introduced. CAD/CAM abutments can be custom designed to re-create the desired emergence profile and supporting crown orientation, facilitating the formation of anatomical mucosal topography and coronal contours for prosthetic replacement.34 Although very stable from a technical point of view, all abutments made of commercially pure titanium have been reported to cause a greyish discolouration of the surrounding soft tissues, compromising the esthetic outcome in the anterior region.56 This discolouration is most apparent in patients with a thin gingival biotype that is incapable of blocking reflective light from the metallic abutment surface.5 Due to their tooth-like colour and potential biologic advantages, ceramic abutments have been promoted to achieve better mucogingival esthetics. 789 Nevertheless, the esthetic benefit of all-ceramic abutments needs to be carefully balanced against the reduced fracture resistance compared to titanium abutments.10 All-ceramic abutments cannot be machined to the same degree of precision as metal abutments. Recent studies have shown that zirconia abutments have a marginal misfit to the implant that might cause screw loosening, micromotion, wear of the implant-abutment interface, and increased size of the marginal gap subject to bacterial colonization.11121314 In addition to commercially pure titanium abutments, clinical studies have reported promising results with surface modifications of titanium, such as coatings of CAD/CAM abutments with titanium nitride (TiN).1516
The TiN-coating is created by a plasma coating process in which titanium and nitrogen ions are combined with TiN, and then molecularly bonded with the titanium substrate of the abutment. Reports have characterized TiN as having a high chemical inertness, low friction coefficient, and good biocompatibility.1718 TiN has excellent infrared reflectivity properties, reflecting in a spectrum similar to elemental gold, achieving a warm esthetic tone under the mucosa because of its gold shaded hue.19 Less color difference of the peri-implant mucosa has been reported with gold-shaded and titanium nitride-coated CAD/CAM abutments.152021 In addition, TiN coatings seem to have a beneficial effect on antibacterial activity inhibiting the formation of microbial plaque, minimizing the adverse effects of peri-implantitis on implant longevity. It reduces bacteria, diminishes its metabolic activity, adhesion and proliferation but simultaneously maintains the biological affinity of titanium surfaces towards bone cell precursors and promotes human gingival fibroblast adhesion.18222324 In light of this, antibacterial activity is a desirable property while, especially for an abutment, enhanced abrasion resistance against scaling treatments is wanted to maintain the surface finish of the abutment. The surface properties of implant components at a gingival level have a decisive impact on the long term success of dental implants. Surface roughness beyond a threshold of 0.2 µm was found to be unsupportive in the prevention of plaque accumulation.2526 An ideal transmucosal implant surface should be smooth, in order to allow the formation of an epithelial seal that prevents plaque accumulation.252627 However, inappropriate instruments during regular maintenance therapy and plaque control may have an adverse effect on the surface integrity and biocompatibility of TiN-coated implant abutments.28 Therefore, the aim of this in vitro study was to investigate the extent of treatment traces, surface roughness (Sa, in µm) and developed interfacial area ratio (Sdr, %) of TiN CAD/CAM abutments after treatment with various implant prophylaxis instruments.
Go to : 
MATERIALS AND METHODS
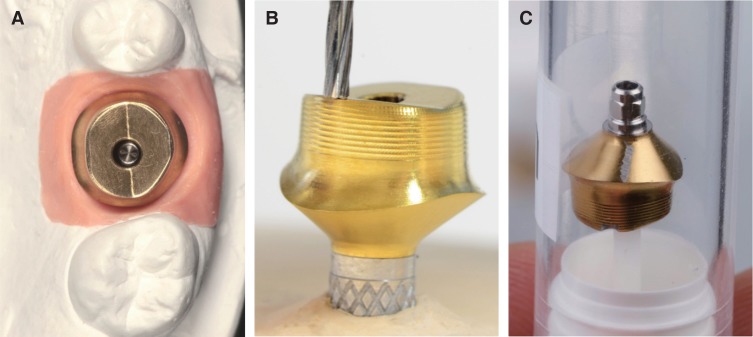
A total of 12 titanium nitride coated (TiN) CAD/CAM implant abutments were virtually designed and centrally manufactured (ATLANTIS GoldHue, Dentsply Sirona Implants, Mölndal, Sweden). The master cast of a clinical case in which the left maxillary first molar had been replaced by an implant restoration served as model of origin. The emergence profile of the peri-implant mucosa had been pre-conditioned by means of a temporary implant-supported single crown. The abutment and outer geometry were designed to allow placement of the crown margin slightly below the mucosa, following its scalloped anatomy. All specimens underwent a standardized ultrasonic cleaning procedure according to Gehrke et al.29 (Fig. 1). The samples were cleansed three times in an ultrasonic bath at 60℃ for 10 minutes each. A resin nano ceramic (RNC) crown (Lava Ultimate, 3M ESPE, Neuss, Germany) was CAD/CAM produced (Cerec 3D, Sirona Dental Systems GmbH, Bensheim, Germany) and fixed on each abutment with a low-viscous silicone (Fit Checker Advanced, GC Corporation, Tokyo, Japan) prior to testing. It was refrained from cementing the crown in order to avoid surface alterations of the abutment shoulder due to undetected cement remnants.
For the present in vitro study the abutment-crown assemblies (12) were randomly divided into four groups of three samples each (3 test groups/ 1 control group).
In the test groups, three assemblies each were instrumented for 20 strokes with 150 g contact pressure at the labial aspect and 200 g at the oral aspect at the submucosal TiN-abutment shoulder (two 5 × 5 mm test fields on each abutment) with the following instruments: group 1: acrylic scaler (Hu Friedy Mfg. Co., LLC, Frankfurt); group 2: titanium curette (Hu Friedy Mfg. Co., LLC, Frankfurt); and group 3: steel tip on ultrasonic scaler at 30 kHz (Cavitron Plus, Hager & Werken, Dentsply, Duisburg, Germany). Three other abutment samples were not treated and used as a control group. The in vitro scaling of the abutments have been carried out in a custom-made device in order to allow for controlled, standardized conditions (Fig. 2).28 The abutment-crown assemblies were connected to the compatible implant analogs (XiVE D 4.5 mm, Dentsply Sirona Implants, Mannheim, Germany) and mounted into the test set-up. A rail mechanism allowed for horizontally defined sliding, simulating the movements of instruments during scaling with a defined pressure (150 g / 200 g).
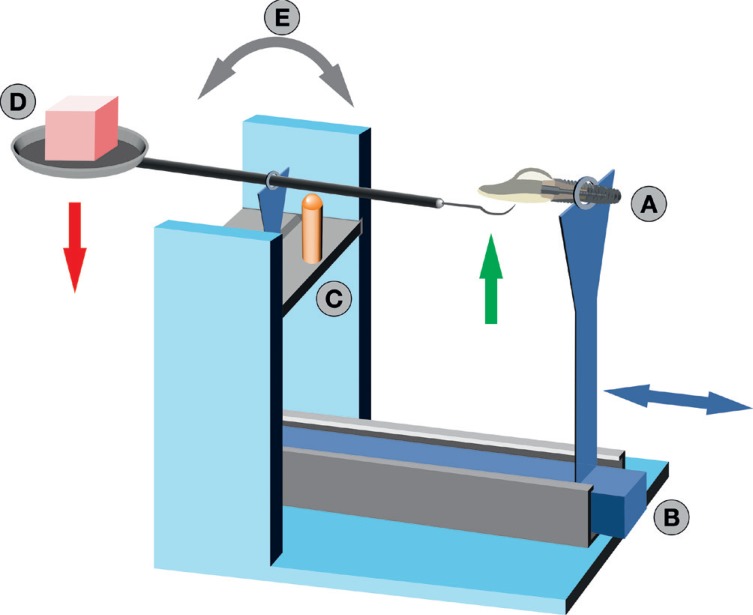 | Fig. 2Schematic test set-up: The TiN abutment-crown assembly was connected to an implant analog (A) and fixed in a horizontal rail mechanism (B). The handle of the scaling instrument was transversely mounted to a metal plate of the test construction, relative to the longitudinal axis of the handle (C). A weight (D) of 150 g / 200 g ensured a defined pressure of the working tip of the scaler at the abutment shoulder during horizontal sliding. Continuous contact of the working tip was provided by a tilting mechanism (E). Once the test specimen was hand-pushed by the rail mechanism, a scaling movement was simulated.
|
The test and control abutments were examined for average surface roughness (Sa) and developed interfacial surface area ratio due to texture (Sdr) by means of profilometric focus-variation microscopy (Infinite Focus Standard G4, Alicona Imaging GmbH, Graz, Austria). Treatment traces were analyzed by scanning electron microscopy (SEM) (Phenom ProX, PhenomWorld B.V., Eindhoven, Netherlands). The magnifications of the test and control fields were ×1000 and ×5000 times. The quality of the treatment traces on the abutment shoulder was classified by 3 independent investigators who, prior to study initiation, were calibrated for intra- and inter-examiner reproducibility using duplicate measurements of a minimum of 30 treated surfaces. These investigators classified the treatment traces using 3 grades: none, moderate, and pronounced. The untreated TiN-abutment surfaces served as controls.
For continuous variables, mean and standard deviation of the individual values were calculated. Frequency distributions were used to characterize categorical variables. Estimation of inter-rater agreement for the toolmark ratings of different raters were executed by calculating Cohens Kappa coefficient. Mann-Whitney U-Test and Kruskal-Wallis H-Test were used to compare two (e.g. contact pressure 150 g vs. 200 g) or more than two (e.g. test and control groups) independent groups for continuous variables (e.g. Sa). In case of categorial comparisons (e.g. test and control groups vs. coating displacement), Pearsons's chi-squared test was applied. Statistical analysis was carried out using the program packages STATISTICA (version 9.1, STATSOFT, Tulsa, OK, USA) and BiAS (version 11.02, Epsilon-Verlag, Frankfurt, Germany). Significance was set at P < .05.
Go to :
RESULTS
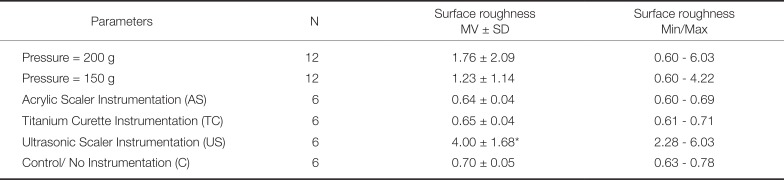
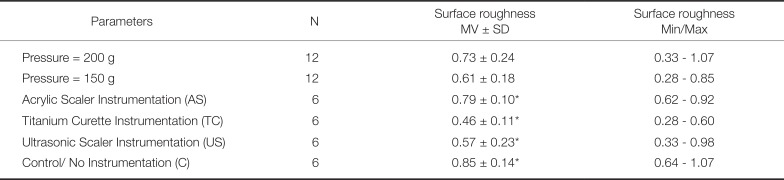
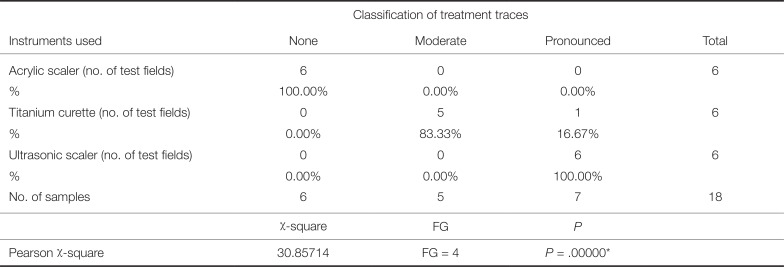
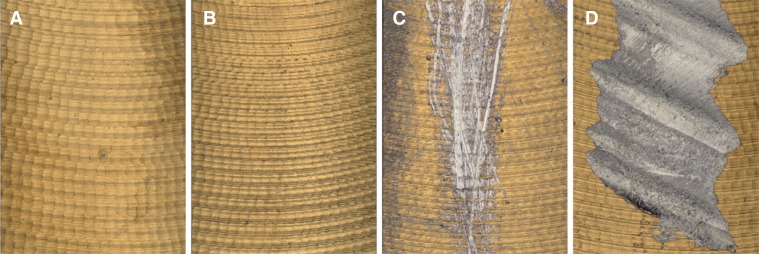
Descriptive characteristic variables for the avarage surface roughness (Sa, in µm) and developed interfacial area ratio (Sdr, %) according to instrumentation is shown in Table 1 and Table 2. A pairwise comparison of treatment categories is presented in Table 3 and Table 4 for recorded Sa values and interfacial area ratio values. Profilometric images of the TiN surfaces with various treatments showed differences depending upon the given treatment (Fig. 3). Manipulation with ultrasonic scalers resulted in a significant increase of average surface roughness (Sa, P < .05). Treatment group comparison proved likewise an increase of developed interfacial area ratio contributed by the texture of TiN surfaces manipulated with ultrasonic instruments (Table 2). Variable contact pressure did not yield any statistically significant difference on Sa values for all instruments (Table 3). The quantitative evaluation of treatment traces by SEM analysis revealed major disparities (Fig. 4). After instrumentation with ultrasonic scalers, all examiners classified the resulting treatment traces on the abutment's TiN-layer as pronounced. Ultrasonic treatment resulted in partial detachment of the TiN-coating in combination with a planning effect of the surface. Titanium curettes predominantly caused moderate treatment traces, while no traces or detectable substance removal have been determined after manipulation with acrylic curettes. However, the samples displayed organic material on the abutment surface due to wear of friction of the acrylic instrument (Fig. 4). The difference between the treatment groups were statistically significant (P < .001) (Table 5). An influence of variable contact pressure with 200 g vs. 150 g was negligible (P = .843)(Table 6).


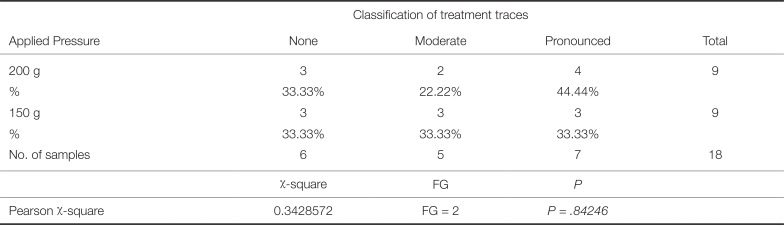
 | Fig. 3Profilometric microscopy images of the titanium nitride (TiN) surfaces displayed differences depending upon the given treatment. Samples treated with 150 g contact pressure: Untreated TiN surface, control (A), TiN surface instrumented with acrylic tip (B), titanium tip (C), and ultrasonic scaler (D). The acrylic scaler did not appear to affect the TiN surface after treatment. The severity of surface traces increased from utilizing titanium curettes to ultrasonic scalers. Ultrasonic scaling led to a significant increase of mean surface roughness (Sa) and partial detachment of the TiN coating.
|
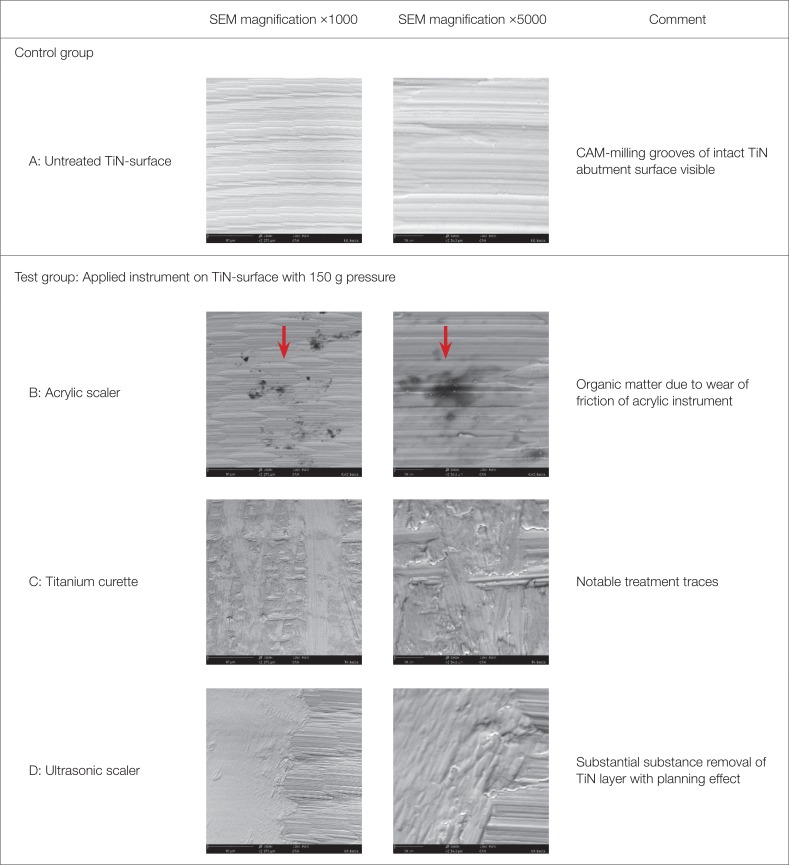 | Fig. 4SEM images of untreated titanium nitride surfaces (A: control) and instrumented titanium nitride surfaces (test). B: acrylic scaler, C: titanium curette, D: ultrasonic scaler.
|
Table 1
Descriptive characteristic variables for average surface roughness Sa (in µm) according to the used instrument and applied contact pressure (200 g / 150 g; two 2 × 2 mm test fields on each abutment)
![]()
Table 2
Descriptive characteristic variables for the developed interfacial area ratio (Sdr, %) according to the used instrument and applied contact pressure (200 g / 150 g; two 2 × 2-mm test fields on each abutment)
![]()
Table 3
Difference of average surface roughness (Sa, µm) after instrumentation with 200 g vs. 150 g contact pressure
| Mann-Whitney U-Test | ||||||
|---|---|---|---|---|---|---|
| Pressure 200 g | Pressure 150 g | U | Valid N 200 g | Valid N 150 g | Exact P | |
| Profile Sa (µm) | 155.0000 | 145.0000 | 67.00000 | 12 | 12 | 0.798745 |
![]()
Table 4
Difference of developed interfacial area ratio (Sdr, %) after instrumentation with 200 g vs. 150 g contact pressure (all instruments)
| Mann-Whitney U-Test | ||||||
|---|---|---|---|---|---|---|
| Pressure 200 g | Pressure 150 g | U | Valid N 200 g | Valid N 150 g | Exact P | |
| Profile Sdr (%) | 171.0000 | 129.0000 | 51.0000 | 12 | 12 | 0.241524 |
![]()
Table 5
After instrumentation with ultrasonic scalers, all examiners classified the resulting treatment traces on the abutmen's TiN-layer as pronounced. Titanium curettes caused predominantly moderate treatment traces, while acrylic scalers did not appear to significantly affect the TiN-surface of the abutment
![]()
Table 6
An influence of the applied contact pressure on the classification of treatment traces and detectable substance removal could not be demonstrated (Pearson-Square: P = .843)
![]()
Go to :
DISCUSSION
Since implant abutments are a part of the superstructure that is in direct contact with peri-implant tissues, their material and surface topography influence the soft-tissue reaction directly.30 A titanium nitride (TiN) coating of CAD/CAM implant abutments may clinically offer esthetic and biological advantages. Studies have shown a beneficial effect of TiN on antibacterial activity inhibiting the formation of microbial plaque and a prevention of compromising color differences of the peri-implant mucosa in patients with thin gingival biotypes.152021 Although considered to be essential for the prevention of inflammatory peri-implant diseases, a periodic removal of debris from the implant abutment shoulder could damage the TiN layer and change or roughen the surface profile. Surface alterations occurring over time might jeopardize the biocompatibility of the material and consequently lead to increased plaque accumulation that could adversely affect the peri-implant region.31 Within the limitations of this in vitro investigation, the results demonstrate that titanium curettes and ultrasonic scalers with steel tips leave gradually pronounced treatment traces on TiN-coated CAD/CAM abutments, independent of the contact pressure applied (200 g vs. 150 g). While titanium curettes caused predominantly moderate treatment traces, ultrasonic scaling led to a partially detachment of the TiN-coating. In addition, manipulation with ultrasonic scalers resulted in a significant increase of average surface roughness (Sa) and developed interfacial surface area ratio (Sdr). No treatment traces, no alterations of roughness depth, and no detectable substance removal could be observed after manipulation with acrylic curettes. A concern, however, is the organic material located on the abutment surface due to frictional wear of the acrylic tip of the instrument. The biological consequences of implant or abutment contamination with plastic residues are critically discussed. It has been suggested that the biocompatibility of the surface may be impaired by the debris.32 Yang et al.33 demonstrated a surface coverage of plastic remnants of up to 15% on titanium discs after instrumentation with various plastic instruments and subsequent attempt of cleaning with water spray or a chlorhexidine- soaked cotton pellets. There is a relative abundance of literature on the effect of mechanical instruments on titanium implants.313435 In contrast, the impact of scaling on the integrity of TiN coated abutments were not extensively studied so far. No in vivo studies on this topic have yet been published. Mengel et al.28 examined the treatment of uncoated and TiN coated abutments in vitro with different instruments and summarized that a TiN coating may offer a way to prevent titanium abutments from sustaining damage during scaling. Moreover, the aforementioned trial concluded that, unlike the current study, TiN coated abutments can be treated with all instruments and equipment at low contact pressure without surface damage. Only high contact pressure on steel or titanium curettes and ultrasonic scalers with steel tips left pronounced treatment traces and caused a detachment of the surface coating.
While roughening of transmucosal prosthetic components should be avoided, it has not been adequately clarified to what extent various types of instrumentation alter the surface of the abutment shoulder and influence bacterial colonization. Similar to our results, Schmidt et al.35 demonstrated an increase of average surface roughness using metal curettes at implant collars. However, no significant differences in surface roughness and biofilm formation based on one-time instrumentation have been observed with ultrasonic devices with steel or plastic coated tips. A single roughness parameter has only limited validity with regard to the surface texture. The Sa value as arithmetic mean possibly represents the most important parameter for assessment. To obtain a more detailed overview of the surface characteristics, however, inclusion of the area excess (Sdr) appears to be useful. Sdr further differentiates surfaces of similar amplitudes and average roughness. To simulate the clinical situation as close as possible, standardized conditions by means of a customized device have been applied for mechanical treatment with defined pressure of 20 strokes. A comparison of the results to previous investigations proved to be difficult since pressure applied for treatment, application time of instruments, and number of strokes varied greatly among these studies.31
Go to :
CONCLUSION
Within the limitations of this in vitro study, the following conclusions can be drawn: inappropriate instrument selection during regular recall and plaque control measures may have an adverse effect on the integrity of the TiN coating of CAD/CAM abutments. The resulting roughness could increase plaque and bacteria retention. To prevent resolution defects and/or increased surface roughness at the transmucosal zone of TiN coated CAD/CAM abutments, only acrylic scaling instruments can be recommended for regular maintenance care.
Go to :
 XML Download
XML Download