

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The diagnosis of Kawasaki disease depends on clinical symptoms, which makes it difficult to diagnose early in patients with only cervical lymphadenopathy. The purpose of this study is to understand the clinical characteristics of cervical-lymph-node-first presentation of Kawasaki disease and compare them with those of typical Kawasaki disease.
Methods
We surveyed 283 patients who were admitted to Hallym Sacred Heart Hospital and were diagnosed with Kawasaki disease from January 2012 to December 2014. The patients were divided into two groups: cervical-lymph-node-first presentation of Kawasaki disease (LKD, N=24) and typical Kawasaki disease (KD, N=259). The medical records were retrospectively reviewed.
Results
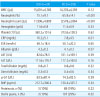
The mean age of the LKD group was higher than that of the KD group (P=0.04). At admission, the LKD patients had on average 1.62 out of 5 symptoms, whereas the KD patients had 3.47. The time from fever to diagnosis and administration of IV immunoglobulin was longer in the LKD group than in the KD group (P<0.001). The mean C-reactive protein of the LKD group was higher than that of the KD group (P=0.01). There were no statistical differences in the presence of coronary artery complications between the two groups at two weeks or at two months after diagnosis (P=0.52, P=0.08).
Figures and Tables
Table 1
Comparison of Characteristics between Cervical-lymph-node-first Presentation of Kawasaki Disease Group and Typically Manifested Kawasaki Disease Group

Abbreviation: IVIG, intravenous immunoglobulin.
*Symptoms observed at admission.
†Including BCG scar site redness.
‡Days from fever onset to the day of admission.
∫Days from fever onset to the day diagnosed as Kawasaki disease and received IVIG treatment.
∥Days from the day of admission to the day diagnosed as Kawasaki disease and received IVIG treatment.
¶Cases received antibiotics at admission.
**Cases received 2nd IVIG because of sustained fever or relapsed fever after 36 hours of 1st IVIG treatment.
References
1. Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974; 54:271–276.

2. Bell DM, Morens DM, Holman RC, Hurwitz ES, Hunter MK. Kawasaki syndrome in the United States: 1976 to 1980. Am J Dis Child. 1983; 137:211–214.
3. Burns JC, Mason WH, Glode MP, Shulman ST, Melish ME, Meissner C, et al. Clinical and epidemiologic characteristics of patients referred for evaluation of possible Kawasaki disease. J Pediatr. 1991; 118:680–686.
4. Mason WH, Takahashi M. Kawasaki syndrome. Clin Infect Dis. 1999; 28:169–185.
5. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004; 110:2747–2771.
6. Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, Duffy CE, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. 1986; 315:341–347.
7. Ayusawa M, Sonobe T, Uemura S, Ogawa S, Nakamura Y, Kiyosawa N, et al. Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition). Pediatr Int. 2005; 47:232–234.
8. Youn YS, Yoon HW, Kim SY, Sul JY, Song CJ, Kim JM, et al. Clinical evaluation of tissue biopsy for children with neck mass; a single center study. Korean J Pediatr. 2005; 48:839–845.
9. Anderson MS, Todd JK, Glodé MP. Delayed diagnosis of Kawasaki syndrome: an analysis of the problem. Pediatrics. 2005; 115:e428–e433.
10. Rowley AH, Gonzalez-Crussi F, Shulman ST. Kawasaki syndrome. Rev Infect Dis. 1988; 10:1–15.
11. Kao HT, Huang YC, Lin TY. Kawasaki disease presenting as cervical lymphadenitis or deep neck infection. Otolaryngol Head Neck Surg. 2001; 124:468–470.
12. Stamos JK, Corydon K, Donaldson J, Shulman ST. Lymphadenitis as the dominant manifestation of Kawasaki disease. Pediatrics. 1994; 93:525–528.
13. Kim JY, Kim JH, Moon SJ, Cho BS, Cha SH. Clinical characteristics of lymphadenopathy as the initial manifestation of Kawasaki disease. Korean J Pediatr Infect Dis. 2000; 7:152–158.
14. Tashiro N, Matsubara T, Uchida M, Katayama K, Ichiyama T, Furukawa S. Ultrasonographic evaluation of cervical lymph nodes in Kawasaki disease. Pediatrics. 2002; 109:e77.
15. Yanagi S, Nomura Y, Masuda K, Koriyama C, Sameshima K, Eguchi T, et al. Early diagnosis of Kawasaki disease in patients with cervical lymphadenopathy. Pediatr Int. 2008; 50:179–183.
16. Kubota M, Usami I, Yamakawa M, Tomita Y, Haruta T. Kawasaki disease with lymphadenopathy and fever as sole initial manifestations. J Paediatr Child Health. 2008; 44:359–362.
17. Kook DH, Ko YM, Lee KY, Kim DU, Lee KY, Lee JS. Characteristics of Kawasaki disease patients who are unresponsive to high-dose intravenous immunoglobulin therapy. Korean J Pediatr Infect Dis. 2008; 15:180–187.
18. Harada K. Intravenous γ-globulin treatment in Kawasaki disease. Acta Paediatr Jpn. 1991; 33:805–810.
19. Zhang T, Yanagawa H, Oki I, Nakamura Y, Yashiro M, Ojima T, et al. Factors related to cardiac sequelae of Kawasaki disease. Eur J Pediatr. 1999; 158:694–697.
20. Nomura Y, Masuda K, Yoshinaga M, Sameshima K, Miyata K. Patients diagnosed with Kawasaki disease before the fifth day of illness have a higher risk of coronary artery aneurysm. Pediatr Int. 2002; 44:353–357.
21. Muta H, Ishii M, Sakaue T, Egami K, Furui J, Sugahara Y, et al. Older age is a risk factor for the development of cardiovascular sequelae in Kawasaki disease. Pediatrics. 2004; 114:751–754.
22. Joffe A, Kabani A, Jadavji T. Atypical and complicated Kawasaki disease in infants. Do we need criteria? West J Med. 1995; 162:322–327.
23. Fan P, Chiu C, Yen M, Huang Y, Li C, Lin T. School-aged children with Kawasaki disease: high incidence of cervical lymphadenopathy and coronary artery involvement. J Paediatr Child Health. 2003; 39:55–57.
24. Lee KY, Hong JH, Han JW, Lee JS, Lee BC, Burgner D. Features of Kawasaki disease at the extremes of age. J Paediatr Child Health. 2006; 42:423–427.
25. April MM, Burns JC, Newburger JW, Healy GB. Kawasaki disease and cervical adenopathy. Arch Otolaryngol Head Neck Surg. 1989; 115:512–514.
26. Nomura Y, Arata M, Koriyama C, Masuda K, Morita Y, Hazeki D, et al. A severe form of Kawasaki disease presenting with only fever and cervical lymphadenopathy at admission. J Pediatr. 2010; 156:786–791.
 XML Download
XML Download