

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
An arborizing vessel (AV) is composed of a stem vessel and irregular treelike branching vessels1. Among a variety of vascular structures on dermoscopy, this appearance of AV is very characteristic, and is regarded as an important dermoscopic feature of basal cell carcinoma (BCC). Thus, AV is included in the dermoscopic diagnostic criteria of pigmented BCC proposed by Menzies et al.2 As a result, most dermatologists who perform dermoscopic exam instinctively consider BCC if they find AV on dermoscopy. Although there have been some reports that AV is found in various skin disorders other than BCC, we experienced AV in more skin conditions than in previous reports. We performed this study to clarify what skin conditions other than BCC can show AV, and what dermoscopic differences of AV differentiate BCC from non-BCC.
MATERIALS AND METHODS
Patients
Among patients who visited the dermatologic clinics in Pusan National University Hospital and Pusan National University Yangsan Hospital from May 2012 to March 2015, patients whose lesions showed AV on dermoscopy were prospectively enrolled in this study. After the final diagnosis was made with skin biopsy, we classified the lesions into BCC and non-BCC. Non-BCCs were classified into tumors and non-tumors. Tumors were further divided into 3 subgroups of benign cystic, benign non-cystic, premalignant, and malignant tumors. This study was approved by Institutional Review Board of Pusan National University Hospital Clinical Trials Center (IRB no. E-2015106).
Methods
1) Photographs
Clinical photographs were taken with a Canon EOS 50D digital single lens reflex camera (Canon, Tokyo, Japan). For dermoscopic images, Dermlite II Pro HR equipment (3Gen; LLC, Dana Point, CA, USA) was used, and dermoscopic photographs were taken with a DSC-W290 (Sony, Tokyo, Japan).
2) Systematic literature search
To identify previous reports demonstrating AV in dermatoses other than BCC, we used PubMed with the following combinations of keywords: “arborizing vessel,” “arborizing vessel AND dermoscopy,” and “vascular AND dermoscopy.” We limited the search to articles published in English before March 31, 2015.
3) Characteristics of AV on the dermoscopy
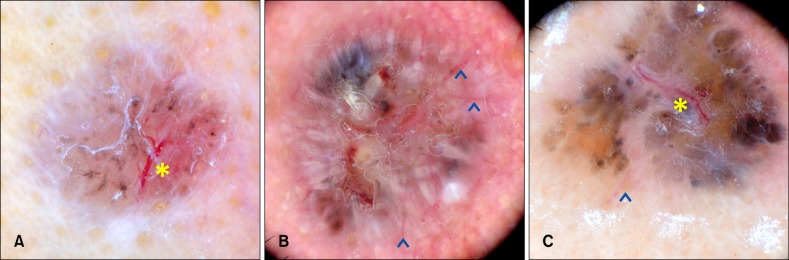
We examined whether AV was focused or unfocused (Fig. 1). We also compared the widest diameter of stem vessel, the widest diameter ratio of stem vessel to the first branch, and the number of ramifications in both groups. Focused AV was defined as bright red AV, which was sharply focused and passed over the central parts of the lesion. Unfocused AV was blurred in color and distributed at the periphery of the lesion3. The widest diameter of stem and branching vessels was measured by using graduation marks of the dermoscope.
4) Statistical analysis
The proportions of focused or unfocused AVs in BCC and non-BCC groups were compared with the chi-square test. The independent t-test was used to evaluate differences between BCC and non-BCC groups (total and individual) in regard to the diameter of the stem vessel, the widest diameter ratio of stem vessel to the first branch and number of ramifications. Statistical significance was defined as a p-value of <0.05 and statistical analysis was performed with IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA).
RESULTS
Demographics
A total of 124 dermoscopic images showing AV were included in this study. Among these, 67 (54.0%) were BCC and 57 (46.0%) were non-BCC. The ratio of male to female subjects was 1 to 1 (BCC, 1:1.09 and non-BCC, 1: 0.90) and the average age was 60.15 years (BCC, 69.12 and non-BCC, 49.60).
Non-BCC with AV
1) Present study
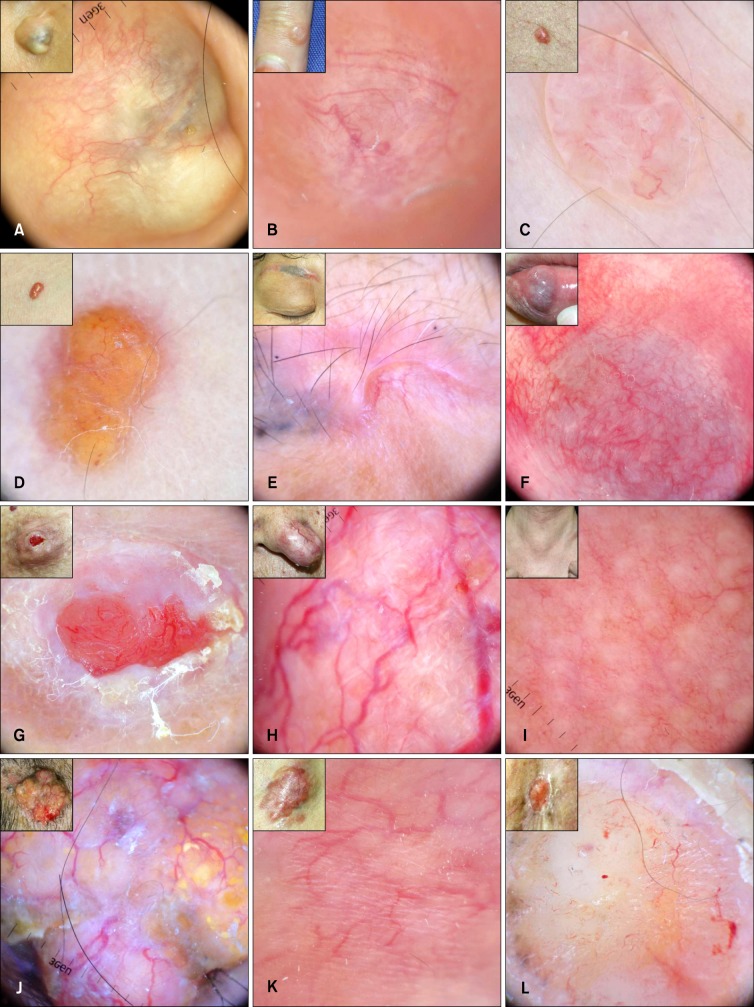
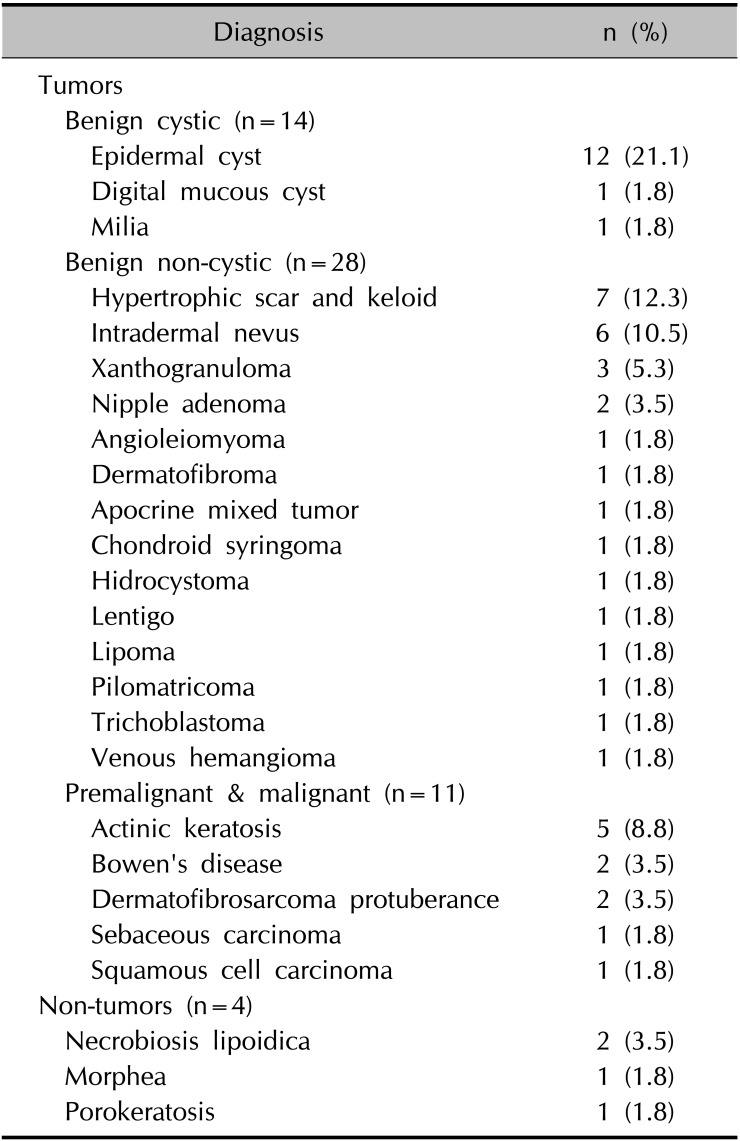
Various skin diseases showed AV (Fig. 2). There were 53 tumors and 4 non-tumors. Among tumors, the benign non-cystic subgroup was most common, followed by benign cystic and premalignant and malignant subgroups (Table 1). The most common dermatosis was epidermal cyst (n=12, 21.1%), followed by hypertrophic scar and keloid (n=7, 12.3%), intradermal nevus (n=6, 10.5%), and actinic keratosis (n=5, 8.8%). Non-tumors included necrobiosis lipoidica, morphea, and porokeratosis.
2) Systematic literature review
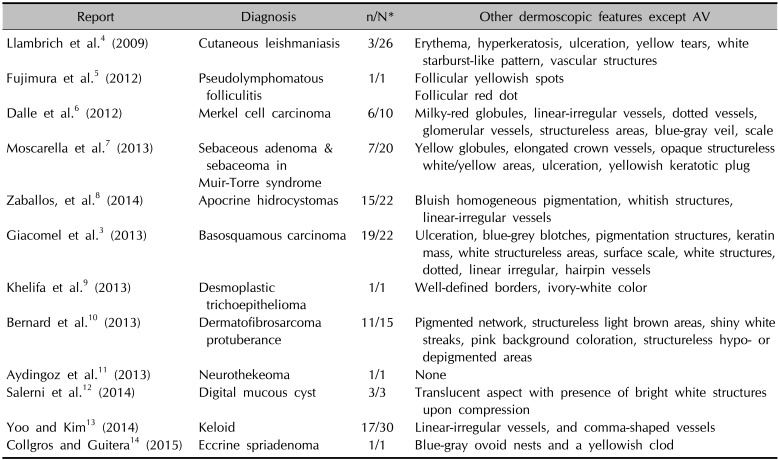
There were some reports of non-BCC with AV (Table 2)34567891011121314. According to the keywords, 9 of 81 articles found with “arborizing vessel,” 8 of 21 articles with “arborizing vessel AND dermoscopy,” and 10 of 250 articles with “vascular AND dermoscopy” were included. Some articles were duplicated, and 12 of 352 were finally selected. Among these, 5 articles were case reports and 7 were original articles.
Characteristics of AV on dermoscopy
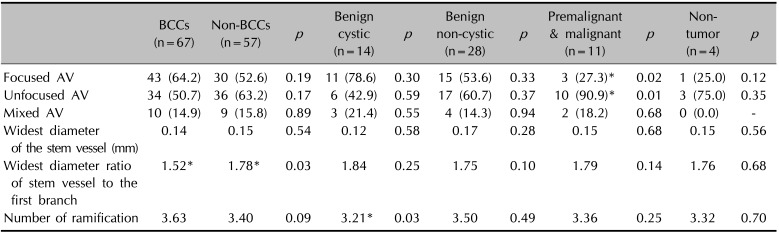
1) Comparison between BCC and non-BCC
Compared to non-BCC, focused AV was more prevalent in the BCC group, but unfocused and mixed AV was less prevalent in the BCC group (Table 3). The widest diameter of stem vessel and the widest diameter ratio of stem vessel to the first branch were less in BCC than in non-BCC. The number of ramifications was greater in BCC than in non-BCC. Of these, only the widest diameter ratio of stem vessel to the first branch was statistically significant at 1.52 in BCC and 1.78 in non-BCC (p=0.03).
2) Comparison between BCC and each subgroup of non-BCC
Statistical significance was only found for whether or not AV were focused in BCC and premalignant and malignant non-BCC, and for ramification numbers in BCC and benign cystic non-BCC (Table 3).
DISCUSSION
Dermoscopy is a noninvasive and very useful diagnostic tool not only for pigmented skin tumors but also nonpigmented dermatoses, including nonpigmented skin tumors, and inflammatory and infectious skin diseases. In dermoscopic analysis of nonpigmented dermatoses, vascular structures can be the main focus. Various types of vascular structures, such as comma-like, dotted, linear-irregular, hairpin, glomerular, and AVs can be observed on dermoscopy, and most of these were described as characteristic for specific entities115. For example, linear-irregular vessels were detected in melanoma, glomerular and dotted vessels arranged in small clusters were described as a specific feature of Bowen's disease, and hairpin, dotted, and/or linear-irregular vessels were commonly observed in squamous cell carcinoma1516. Among these, AV was reported as a dermoscopic hallmark of nodular, sclerodermiform, or cystic BCC, with high diagnostic accuracy217.
The morphology of AV on dermoscopy is very distinctive, and is easily recognizable by dermatologists. However, this could be a pitfall, because AV can be observed in many other skin conditions, including tumors or inflammations. In the present study, AV was observed in a variety of diseases, and many have not been previously reported to show AV. Among the various diseases in this study, only digital mucous cysts, hidrocystomas, keloids, and dermatofibrosarcoma protuberans were reported previously81012. Therefore, dermatologists should not simply confirm BCC when AV is observed on dermoscopy, and should consider possibilities other than BCC.
Accordingly, we tried to identify morphologic differences in AV between BCC and non-BCC; to our knowledge, these have not previously been reported. Recently, criteria for morphologic discrimination between focused and unfocused AV have been adopted. By definition, focused AVs show classical arborizing telangiectasias, which resemble branches of a tree. These are composed of large-diameter stem vessels, with branches tapering irregularly into finer capillaries. They are bright red in color and sharply focused on dermoscopy. This is a hallmark of nodular BCC, and passes over the central part of the lesion17. On the other hand, unfocused AVs are branched vessels with blurring located at the periphery of the lesion. Unfocused AV were described as striking vascular features of basosquamous cell carcinoma, observed either alone or in combination with dotted or focused AV3. Unfocused AV was also reported as a major vascular structure in dermatofibrosarcoma protuberans, observed alone or mixed with focused AV10. In the present study, focused AV were more frequently observed in BCC, but the frequency showed no statistical significance compared to non-BCC. In particular, in benign cystic non-BCC, focused AV was more prevalent than in BCC. Therefore, focused AV as a diagnostic feature of BCC needs to be reconsidered. However, we think that classification of AV by whether or not they are focused can help discriminate BCC from premalignant and malignant non-BCC. Before this study, we surmised that the stem vessel in BCC might be thicker than that of non-BCC. On the contrary, the diameter of stem vessels in non-BCC was greater than in BCC. In particular, the diameter of stem vessels is greatest in benign cystic lesions. The widest diameter ratio of stem vessel to the first branch was less in BCC than in non-BCC. This means that the diameter of the branch vessel remains larger. This is supposedly related to cancer angiogenesis, but further investigation is needed to determine the relationship between the morphology of AV and clinical characteristics, such as aggressive progression. The number of ramifications was greater in BCC than that of non-BCC, and this difference was statistically significant compared to benign cystic non-BCC. This could also be related to cancer angiogenesis in BCC. The morphologic differences of AV found in this study could be helpful in discriminating BCC from non-BCC.
In the present study, we investigated what skin diseases other than BCC can display AV on dermoscopy. Besides BCC, AV was observed in various dermatoses, including benign cystic, non-cystic, premalignant, and malignant tumors, and even non-tumors, including necrobiosis lipoidica, morphea, and porokeratosis. Even though AV is a very distinct and remarkable dermoscopic vascular structure, and is reportedly very specific in the diagnosis of BCC using dermoscopy, dermatologists should be careful in interpreting the significance of AV. Furthermore, we tried to identify dermoscopic differences of AV between BCC and non-BCC. Focused AV were observed more frequently in BCC, and unfocused AV were dominant in premalignant and malignant non-BCC. In non-BCC, the number of ramifications was less than in BCC, and the diameter of vessels decreased more acutely from the stem vessel to the first branch. In ambiguous cases with AV, these dermoscopic differences could help differentiate lesions.
 XML Download
XML Download