

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Psoriasis is a common, chronic, and recurrent inflammatory disease of the skin affecting 1%~3% of the population worldwide1. This disorder can be associated with a characteristic variant of inflammatory arthritis termed as psoriatic arthritis (PsA). According to a recent systematic review, 7%~26% of patients with psoriasis develop PsA, which manifests as pain and stiffness, swelling, and joint disability in several patterns2.
Some features distinguish PsA from other forms of arthritis. Unlike rheumatoid arthritis, the pattern of joint involvement in PsA is usually asymmetric and frequently involves the distal interphalangeal (DIP) joints. There is also no marker of PsA that is usually seronegative for rheumatoid factor. Importantly, >90% of PsA cases are associated with psoriasis3. For these reasons, it is generally accepted that PsA is a distinct entity from other specified arthropathies. There is a link between psoriasis and PsA; however, the relation between skin and joint manifestations in PsA patients is inconsistent, and shared genetic markers or disease mechanisms have not been definitely elucidated4. A better understanding of the development of the symptoms of PsA, including early warning signs, would be of great value.
Patients with PsA experience significant morbidities such as progressive joint destruction and functional disability, in addition to increased health-care costs5678. As PsA is preceded by cutaneous psoriasis in 80% of cases, dermatologists have an important role in screening psoriasis patients for PsA and assessing them before further evaluation9. A recent study has shown that up to 29% of psoriasis patients seen by dermatologists have undiagnosed PsA10. Additionally, it is important for dermatologists to evaluate psoriatic nail involvement because nail psoriasis is associated with a prolonged duration of psoriasis itself and a greater severity of skin and joint involvement, and may also be an indicator for the severity of PsA.
Several classification criteria have been developed because the diagnosis of PsA is challenging. In 2006, the criteria of the classification of psoriatic arthritis (CASPAR) study group were derived from an in-depth clinical, laboratory, and radiographic study of 588 PsA cases and 536 controls with rheumatoid arthritis, ankylosing spondylitis, or undifferentiated arthritis11. However, there is a possibility of overdiagnosing PsA when using the CASPAR criteria in that psoriatic patients with joint symptoms and nail involvement can be considered as having PsA.
The purpose of this study was to investigate the prevalence of PsA by using the CASPAR criteria, as well as its correlation with psoriasis severity and nail psoriasis severity. The diagnosis was based on physical examination alone. Our aim was to estimate the proportion of psoriatic patients with suspected PsA diagnosed by using the CASPAR criteria without laboratory tests and radiology imaging. Measuring joint involvement is one of the most essential evaluation before determining the presence and clinical patterns of PsA. Therefore, the study patients with peripheral joint symptoms were assessed by the Joint Count 66/68 (JC66/68), which allows a global analysis of inflammatory involvement in PsA by capturing a maximum number of peripheral joints and minimizing chances to miss affected one12. Additionally, we evaluated all the fingernails and toenails of the included psoriatic patients by calculating the nail psoriasis severity index (NAPSI) score.
MATERIALS AND METHODS
Study design
This epidemiological research was organized as a single-center, noninterventional, cross-sectional observational cohort study. The study population comprised patients with psoriasis who visited the dermatology clinic at Seoul National University Bundang Hospital between January and September 2015. The protocol of the study was approved by the institutional review boards (IRB) and conducted according to the principles of the Declaration of Helsinki (IRB no. B-1412/278-005).
Conduct of the study
Outpatients with a confirmed diagnosis of psoriasis were enrolled consecutively. After the patients gave written informed consent, basic demographic data were recorded, including age, age of psoriasis onset, sex, comorbidities (heart diseases and stroke, diabetes, hyperlipidemia, hypertension, and fatty liver), type of psoriasis (plaque psoriasis or localized pustular psoriasis), and sites of psoriatic skin lesions (scalp, face, intertriginous area, genitalia, or nail). The current disease severity was quantified by using the psoriasis area and severity index (PASI). Severity was then assigned as mild (<10), moderate (10~20), or severe (>20). The extent of the disease was evaluated according to the affected body surface area (BSA) of psoriasis. Severity was then assigned as mild (<3%), moderate (3%~10%), or severe (>20%). In addition, NAPSI was used for the precise evaluation of the severity of finger and toe nail lesions because one of the most distinguishing clinical features of PsA is known to be nail involvement13. Patients with a score of ≥1 were considered as having nail psoriasis. The PASI, BSA, and NAPSI were calculated by the same highly experienced dermatologist (S.W. Youn) to exclude the possibility of interrater variability.
The investigator presented the psoriatic patients with a list of questions related to possible joint involvement. Five of the questions were from the Psoriasis Epidemiology Screening Tool (PEST) for the screening of PsA14. Regardless of the number of positive responses to these five questions, any patient with joint symptoms was further evaluated by the investigators.
Joint involvement, the most essential part of making a diagnosis of PsA, was assessed by using the JC66/68 assessment, a reliable method in evaluating articular manifestations. The clinical diagnosis of PsA was based on the CASPAR criteria; however, axial/spinal joint involvement (spondylitis and/or sacroiliitis) was not evaluated. The CASPAR criteria require a diagnosis of inflammatory articular disease documented by either a primary care physician or a rheumatologist. The subjects who fulfilled the CASPAR criteria with a score of ≥3 were considered as patients having PsA. The CASPAR criteria requires a diagnosis of inflammatory articular disease (joint, spine, entheseal) documented by either a primary care physician or a rheumatologist, and achievement of a score of ≥3 of the following 5 CASPAR criteria: 1) current psoriasis (score of 2), personal history of psoriasis, or family history of psoriasis; 2) nail dystrophy such as onycholysis, pitting, or hyperkeratosis; 3) a negative rheumatoid factor (RF); 4) current dactylitis or a personal history of dactylitis as recorded by a physician; and 5) radiographic evidence of psoriatic bone changes of the hand or foot, such as juxta-articular new bone formation on plain film11. Laboratory tests and imaging tests were not used for further evaluation of the psoriatic patients with joint symptoms.
Statistical analysis
Descriptive statistics were used to summarize the characteristics of the study population. The associations between PsA and other suggested factors were assessed with a binary logistic regression to remove confounding effects. For continuous variables, the significance of the difference between the means of the groups was investigated by using Student's t-test. Categorical variables were analyzed with Pearson's chi-square test. Statistical significance was set at p<0.05 on the basis of a two-sided calculation. All calculations were made with IBM SPSS Statistics ver. 20.0 for Windows (IBM Co., Armonk, NY, USA).
RESULTS
Patient demographics
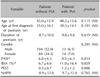
The study population comprised a cohort of 200 psoriasis patients. In this cohort, we identified 34 (17.0%) psoriatic patients with joint symptoms, and confirmed PsA by using the CASPAR criteria in 27 (13.5%) patients, which is 79% of psoriatic patients with joint symptoms. None of these patients had a previous diagnosis of PsA. Seven patients did not satisfy the CASPAR criteria because nail psoriasis or active cutaneous psoriasis was not found. Therefore, 27 patients (13.5%) were considered as having psoriasis with PsA. Table 1 shows the clinical features of the 200 included psoriatic patients compared with the 27 PsA patients. The mean age of PsA patients was 48.2 years, and 47.6% were men. The mean age at first diagnosis of psoriasis was 39.3 years, and the mean duration of psoriasis was 9.8 years in the PsA group.
Table 2 presents the results from the comparative analyses based on the presence or absence of PsA. There were no significant differences in age and the age at the onset of psoriasis between the two groups. The mean psoriasis duration was higher in patients with PsA than in those with psoriasis alone; however, the difference was not statistically significant. The sex distribution was similar between the two groups.
PsA and psoriatic features
The prevalence of nail psoriasis in the study population was 85.5%, and all of the patients with PsA had nail psoriasis. Plaque psoriasis was found in 77.8% of the PsA patients, whereas localized pustular psoriasis including palmoplantar pustulosis was noted in 22.2% of PsA patients. Psoriatic involvement of the intertriginous area and genitalia was more common among PsA patients. All study patients had used topical agents, and >25% of the patients had been prescribed with oral systemic drugs in the past regardless of PsA status. Interestingly, the patients with PsA in our study population never had a history of biologics use. When a binary logistic regression was performed, hyperlipidemia and localized pustular psoriasis were found to be significant predictors of PsA with odd ratios of 4.08 and 9.16, respectively. The effect of other nominal parameters listed in Table 1 was not significantly predictive (p-values are not shown).
PsA and psoriasis severity
The PASI score was significantly higher in PsA patients than in those with psoriasis alone (p=0.014, Table 2). As seen in Fig. 1, the frequency distributions of patients in PASI values were different in the two groups. The frequency distribution in psoriatic patients without PsA was more skewed to the right (between 0 and 5 of the PASI score), whereas the PsA patients were distributed mostly between 5 and 15 in terms of PASI scores. In addition, BSA, which is also indicative of psoriasis severity, was higher in the PsA group, and the difference was statistically significant. Patients with localized pustular psoriasis were omitted from the calculation because the PASI and BSA were not applicable. The mean of the total number of positive responses to five questions, which form the basis of the PEST screening questionnaire, was significantly higher in patients with PsA (p=0.006).
PsA and nail psoriasis severity
For the evaluation of nail psoriasis, we calculated the NAPSI score to measure the severity of nail involvement. The mean NAPSI scores were 7.9±11.2 (mean±standard deviation [SD]) and 18.0±19.1 (mean±SD) in patients with chronic plaque psoriasis and localized pustular psoriasis, respectively. The difference was statistically significant (p=0.027). The mean NAPSI score was higher in patients with PsA; however, the difference was not statistically significant (Table 2). Fig. 2 plots the frequency distribution of patients in NAPSI values according to presence or absence of PsA for the two different types of psoriasis. As shown in the Fig. 2A, most of the patients with chronic plaque psoriasis had a NAPSI score of <20, and the frequency distribution of NAPSI in PsA patients was similar to that in psoriatic patients without PsA. Fig. 2B shows that the NAPSI scores of localized pustular psoriasis patients are evenly distributed throughout the graph compared with chronic plaque psoriasis patients.
Articular manifestations of PsA
Among patients with PsA assessed by an investigator, oligoarthritis was the most common clinical subset, followed by monoarthritis, and polyarthritis (Table 3). This trend was also seen in psoriatic patients who had complained of joint symptoms. The most commonly affected joints were the finger and toe joints, especially the proximal interphalangeal joints (14.8%) and metacarpophalangeal joints (14.8%) in the hand, and the proximal interphalangeal joints (29.6%) and metatarsophalangeal joints (25.9%) of the foot. Interestingly, the frequency of hand DIP joint involvement was relatively low (11.1%).
DISCUSSION
The prevalence and clinical characteristics of PsA in patients with psoriasis vary greatly worldwide. In one study, the prevalence of arthritis among psoriatic patients was estimated to be up to 42% with the Moll and Wright critieria15. Generally, the prevalence among whites is estimated at 15%~30% in Western countries, which is a rather high prevalence compared with that in Asians. In this prospective cross-sectional study, we found that 13.5% of psoriatic patients fulfilled the CASPAR criteria for PsA. Our results are in line with several other studies in Asian populations16171819. In addition, we found that hyperlipidemia and localized pustular psoriasis were significant predictors of PsA. Previously, it was reported that hyperlipidemia was associated with an elevated risk of psoriasis and psoriasis with PsA20. Our results also agree with those of a previous study, and the close association between localized pustular psoriasis and PsA may be due to the high prevalence of nail psoriasis in patients with localized pustular psoriasis20.
There are some possible reasons for the low prevalence of PsA in our study. First, the patients without PsA might have satisfied other requirements of the CASPAR criteria, such as a negative rheumatoid factor or positive radiographic imaging of psoriatic bone changes. Therefore, more psoriatic patients in the study population might fulfill the CASPAR criteria as patients with suspected PsA did not have blood tests or imaging tests for further evaluation. Secondly, the number of psoriatic patients with arthritis could be higher because patients with spondylitis or axial joint involvement were not evaluated because of the difficulty for dermatologists to assess those joints. Accordingly, the limitations of the use of the JC66/68 in diagnosing PsA should be considered as the axial/spinal joint evaluation is not part of the JC66/68 method for the joint evaluation of PsA.
In the present study, the prevalence of PsA was comparable to that reported 16 years ago, although the patients were further assessed with laboratory evaluation, joint radiography, and bone scintigraphy in the previous study conducted with Korean psoriatic patients21. This suggests that the prevalence of PsA had increased in recent decades, which, as suggested by other researchers, could be caused by environmental factors and improved diagnostic tools18.
For better PsA screening, several questionnaires have been developed. Most of these are relatively complicated and very time consuming for routine clinical use. Recently, a new and simple screening questionnaire consisting of five questions has been proposed to identify cases of PsA in a population of persons with known psoriasis. The five questions that form the basis of the PEST screening questionnaire demonstrated good sensitivity and specificity14. In general, a score of ≥3 indicates a high probability of having PsA14. In our study, the mean of the total number of positive responses to five questions was 1.2 in patients with PsA. This indicates that a cutoff value of 3 might be set too high for reliable screening of PsA, especially in Koreans.
In comparison analyses based on the presence or absence of PsA, the scores of PEST and PASI, and the BSA were significantly higher in patients with PsA than in those without. A recent meta-analysis suggested a trend for an association between high PASI and PsA risk in accordance with our results22. Overall, we can conclude that there is a close relation between the severity of psoriasis and PsA. Psoriatic nail lesions, which can also be indicative of severe psoriasis, occur in about 10%~80% of patients with PsA. In our study, all of the patients with PsA had nail psoriasis as patients had to have nail psoriasis to satisfy the CASPAR criteria without further laboratory or imaging investigations.
This is the first study, to our knowledge, to assess the relation between PsA and psoriatic nail involvement by using the NAPSI score. The mean NAPSI score was higher in patients with PsA; however, the difference was not statistically significant. As a result, the nail psoriasis severity was not significantly different. Interestingly, the prevalence of nail psoriasis in the study population was 85.5%, which is high compared with that reported in previous studies2324. Psoriatic nail involvement, which is one of the most important symptoms-based criteria, should be evaluated thoroughly by dermatologists. If dermatologists carefully evaluate the nails of psoriatic patients like the trend of calculating the NAPSI score, nail involvement of psoriasis may be found more frequently than expected. Therefore, it is questionable whether one or two nail pittings should be considered as nail psoriasis because minor pitting could be found in subjects without any dermatologic disease. If these minor nail changes are considered as nail psoriasis, it is possible for PsA to be overdiagnosed by fulfilling the CASPAR criteria. From a dermatologist's point of view, patients with suspected PsA may need to be evaluated in different ways for the correct diagnosis of PsA, although the CASPAR classification criteria is useful in practice for affirming PsA diagnosis. Accordingly, we suggest that the CASPAR criteria should be more specified by using nail psoriasis severity or the clinical features of nail psoriasis. Many authors demonstrated that oligoarthritis was the most common pattern of PsA, whereas some authors reported that polyarthritis was the most common. The different results between the studies were possibly due to the differences of arthritis severity among the study populations. By assessing the patients with careful joint examination by using the JC66/68, oligoarthritis was the most common pattern of PsA in our study (55.6%). The JC66/68 allows a global analysis of inflammatory involvement in PsA by capturing a maximum number of peripheral joints12. Therefore, we believe that our assessment method minimizes the chances of missing affected persons in terms of peripheral joint evaluation.
The limitations of this study include the lack of a validated assessment by blood tests or imaging tests for the PsA diagnosis in psoriatic patients with joint symptoms. Therefore, our finding may still be an underestimation overall. Nonetheless, this pragmatic study produces results that can be applied in routine dermatology settings where laboratory or imaging tests are not readily available. The results of the previous study by Mease et al. support our findings showing that clinical evaluation alone is often a sufficient basis for PsA diagnosis25.
Conclusively, the prevalence of PsA in patients with psoriasis in Korea from physical examination for PsA was 13.5%. Dermatologists can diagnose PsA from current physical findings by using the nonlaboratory items of the CASPAR criteria. The strong point of the criteria is that the diagnosis of PsA can be established in the presence of proper cutaneous and articular symptoms so dermatologists can enroll appropriate patients with suspected PsA into early clinical intervention. However, careful examination of the fingernails and toenails is of utmost importance because nail psoriasis status can strongly affect making the diagnosis of PsA in patients with suspected PsA on the basis of the CASPAR criteria.




 XML Download
XML Download