

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital melanocytic nevi (CMN) are benign nevomelanocytic proliferations present at birth or which arise within the first few weeks of life1. CMN are classified according to their diameter as small (<1.5 cm), medium (1.5~19.9 cm) or large (≥20 cm)2, where size is a predictor of malignant transformation3. The estimated prevalence of CMN is 0.5% to 31.7%3, and is a common presentation for dermatologists. Treatment of CMN varies depending on the patients' age, psychological effects, lesion size and location. Over the past decade, many CMN treatments have been described4. Excision has been the first-line treatment, especially for lesions with a high risk of malignant transformation5. While bulk removal of the nevus cells is possible, the associated risks include sepsis, scarring and restrictions in joint mobility6. The incidence rate of melanoma in small and medium CMN is <1%78910. Therefore, in these cases, the main aim of treatment is to reliably remove the pigmented skin with minimal scarring. With the evolution of laser and light technology, a number of lasers and intense pulsed light (IPL) have been applied to small and medium sized CMN4111213141516.
IPL therapy using non-coherent broad-spectrum light has been effectively used for hair removal and for treating superficial pigmented lesions and vascular lesions171819202122. Although effective, removal of the deep-seated nevus cells in CMN is expected to be difficult using IPL alone. Recent case reports have described successful treatment of small sized and medium sized CMN combining erbium: yttrium-aluminum-garnet (Er: YAG) lasers with long pulsed laser or IPL1215. The exposure of deep-seated nevomelanocytes to IPL or long pulse laser forms the basis of combination treatment, along with the additional removal of superficial nevus cells by Er: YAG laser ablation.
We herein present the clinical and histological outcomes of small-to-medium sized CMN treated by IPL alone and in combination with Er: YAG laser.
MATERIALS AND METHODS
The study was approved by the institutional review board of the Catholic Medical Center, Seoul, Korea (IRB no. XC15RISI0049KO). We retrospectively screened all patients who received IPL alone or in combination with Er: YAG laser under the diagnosis of small-to-medium sized CMN. Patients with incompatible clinical assessment or biopsy results were excluded. Data regarding patient age at referral, sex, location and size of the nevi, details of treatment, and complications were collected.
Laser treatment
Patients were counseled regarding the risks and benefits of IPL and informed consent for treatment was obtained from the patient or parents (in cases where the patient was under 20 years of age). CMN lesions were photographed pre-treatment. All procedures were performed under local anesthesia and by a single dermatologist. Patients underwent treatment with a non-coherent IPL source (Lumenis One™; Lumenis Inc., San Jose, CA, USA) at 2~3 week interval with a spot size of 15 mm×35 mm, 590 nm filter (590~1,200 nm), fluence of 12~13 J/cm2, double pulse trains of 4 ms with a pulse delay of 20 ms and 755 nm filter (755~1,200 nm), fluence energy 17~18 J/cm2, triple pulse trains of 4 ms with pulse delays of 80 ms. Two or three passes were applied to the CMN. Initially, all patients were treated only with IPL, but in cases where the pigment reduction was less than 15% following treatment, IPL was combined with Er: YAG laser (Joule™; Sciton Inc., Palo Alto, CA, USA). Ablation was performed at settings of 2.5~5 J/cm2 and 8 Hz, with a 2 mm spot size, followed by simultaneous IPL (755 nm filter [755~1,200 nm], fluence energy 17 J/cm2, triple pulse trains of 4 ms with pulse delays of 80 ms) once monthly. IPL fluence and treatment passes were adjusted if judged appropriate by the operator. Further treatments were not carried out if sites of previous treatment had not healed.
Follow-up and clinical evaluation
Patients received IPL treatment at 2~4 week interval until the patient and clinician were satisfied with the results or treatment was deemed complete (defined as “completion of treatment”). Patients were further reviewed one year or more after the last treatment session to check recurrence. At each treatment visit, the CMN were evaluated for the healing status, pigmentation, and complications. Clinical photographs were taken at all visits under identical camera settings (EOS 5D mark II; Canon, Tokyo, Japan) and light conditions. The treatment results were independently evaluated by comparing the pre and post-procedural (taken at the time of treatment completion) photographs by two physicians who were blinded to the study. The degree of improvement and lightening was evaluated using the 5-point scale established by Kilmer et al.23: 1=poor (no change, with lightening of ≤15%); 2=fair (slight improvement, with lightening of 16%~50%); 3=good (improvement, with lightening of 51%~75%); 4=excellent (lightening of 76%~95%); and 5=clear (near-complete disappearance of the lesion, with lightening of ≥95%). Recurrence was defined as the re-appearance of residual pigmentation after completion of treatment in the same area of skin.
Histological evaluation
Punch biopsies (3 mm) were obtained mostly at initial visit to confirm the diagnosis of CMN and to examine the histological melanin content and depth of the nevus cells. Additional biopsies were obtained during or after treatment completion to assess the effect of IPL on CMN and to evaluate the degree of elimination of the nevomelanocytes. Specimens were fixed in 10% formaldehyde solution, embedded in paraffin, sectioned, and stained with hematoxylin-eosin and s-100.
Statistical analysis
Data were analyzed using software (SPSS ver. 22.0 for Windows; IBM Co., Armonk, NY, USA). An independent 2-sample t-test was used to evaluate difference in treatment number and treatment outcomes between the treatment-completed small and medium sized nevi. A p-value of less than 0.05 was considered statistically significant.
RESULTS
Twenty six patients with 26 small-to-medium sized CMN who preferred non-surgical treatment were included. The mean age of the subjects at the time of their first IPL treatment was 11.9±8.4 years. Nine (34.6%) of the CMN were located on the upper extremities, 8 (30.8%) on the face, 5 (19.2%) on the lower extremities, 3 (11.5%) on the trunk and one (3.8%) on the neck (Table 1).
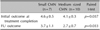
Seventeen patients (65.4%) completed treatment and were followed-up. Nine (34.6%) were not able to complete treatment due to school, work, change in residence, and treatment related stress. Among the treatment completed patients, 10 (58.8%) received IPL alone with a mean of 10.5±5.8 sessions. Seven patients (41.2%) underwent treatment with IPL (mean: 7.7±3.2 sessions) and Er: YAG/IPL combination therapy (mean: 4.7±3.1 sessions) (Fig. 1, Table 2).
Of the 17 treatment complete nevi, 7 (41.2%) were small and 10 (58.8%) were medium in size. Four patients (57.1%) with small CMN received IPL alone with a mean of 9.5±4.2 sessions. Three (42.9%) small CMN were treated with IPL (mean: 6.7±1.5 sessions) and Er: YAG/IPL combination therapy (mean: 2±1 sessions). Six patients (60.0%) with medium sized CMN received IPL alone with a mean of 11.2±6.9 sessions. The remaining four (40%) medium sized CMN were treated with IPL (mean: 8.5±4.1 sessions) and Er: YAG/IPL combination therapy (mean: 6.8±2.4 sessions) (Fig. 1, Table 2).
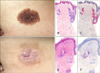
The treatment outcome measured at treatment completion was clear in 5 patients and excellent in 12 (Fig. 2). In the small CMN group, 4 were scored clear and 3 excellent (mean: 4.6±0.5), whereas in the medium-sized CMN group, one was scored clear and 9 excellent (mean: 4.1±0.3). Follow-up evaluation, which was generally made at least one year after treatment completion, showed recurrence in 14 cases (82.4%) (Fig. 3). The overall follow-up scores were 2 clear, 3 excellent, 7 good and 5 fair. The small CMN scored as follows: 2 clear, 2 excellent, 2 good and one fair (mean: 3.7±1.1). The medium-sized CMN scored as follows: 1 excellent, 5 good and 4 fair (mean: 2.7±0.7) (Fig. 1, Table 3).
Histologically, the skin biopsy specimens showed features of a compound nevus with nevomelanocytic cell infiltration in the deep dermis and around the hair follicles. Epidermal detachment and profound collagen degeneration in the superficial and mid-dermis were the findings of a biopsy specimen taken immediately after IPL (Fig. 4).
In terms of complication, 2 patients (7.7%) experienced bullae from IPL therapy (Fig. 5) and one patient (3.8%) experienced focal scarring later on. Treatment related crusting, erythema and post-inflammatory hyperpigmentation and changes in skin texture were experienced by all, but faded with time and was not so significant by the time of their follow-up visit post treatment completion.
One patient who received 23 sessions of IPL and 5 sessions of Er: YAG/IPL combination therapy achieved improvement of CMN but was not able to complete treatment due to change in residence. In the follow-up photos sent from her mother, significant re-pigmentation was noticed. We recommended staged excision which was successfully performed by a derm-surgeon (Fig. 6).
DISCUSSION
IPL emits non-coherent, broad-spectrum light, usually in the 500~1,200 nm range. Apart from wave-length, a wide range of treatment parameters including pulse duration, pulse sequences and pulse delay time are flexible with IPL, allowing it to eliminate hair, treat vascular lesions and remove pigment181920212224. Treatment of pigmented melanocytic lesions by means of IPL has been the object of recent interest and its success has been described12131718212224. The target chromophore of IPL in the treatment of melanocytic lesions is the melanosome. Selective thermal damage has been observed in a wide range of wavelengths, from 351 nm to 1,064 nm25. Short wavelengths (500~600 nm) reach right beneath the epidermis and target superficial melanocytic lesions while sparing the dermis. Longer wavelengths penetrate deeper into the dermis and are suitable for dermal melanocytic lesions1718. Since most CMN are compound nevi, we presumed that the broad wavelength of IPL would be beneficial in CMN treatment. We have applied a 590 nm filter (590~1,200 nm) and a 755 nm filter (755~1,200 nm) to our CMN patients, targeting both the superficial and deep melanosomes. However, to our disappointment, a skin biopsy taken immediately after IPL treatment revealed the effective depth of IPL to be the mid-dermis, sparing the deep nevus cells.
Pulse width is also an important factor to consider. The IPL pulse duration is on the order of ms whereas the thermal relaxation time of melanosomes is 70~250 ns. The long pulse duration of IPL allows less spatially selective, but more gentle, heating of the target chromophores (melanosomes), making it more effective than Q-switched mode lasers for the treatment of melanocytic nevi as they target individual cells and clusters of nevus cells. However, with the high density of melanosomes in CMN, heat accumulation can be excessive at times, resulting in bullae formation.
Among our patients, 2 (7.7%) experienced bullae formation; both patients had dark colored (heavily pigmented) CMN. We advise reducing the fluence energy in treating such patients. As for the results, a Er: YAG/IPL combination was used less often for small CMN, but the number of IPL sessions required for completion of treatment was similar between the small and medium sized CMN. The findings were slightly different from what we had expected, and suggest that the depth rather than the size of the CMN is the primary determinant of treatment number. The small CMN were found to have a better outcome (measured at the time of treatment completion) and follow-up outcome (generally made at least one year after treatment completion) with a comparatively lower recurrence rate (71.4%) to medium sized CMN (90%). Recurrence was observed in the majority of treatment completed patients (82.4%) suggesting the presence of a remnant nevi. In fact, a skin biopsy from one of our treatment completed CMN patient showed remnant nevus cells in the deep dermis confirming the hypothesis (Fig. 7).
Three patients (ages 4, 8, and 9 years) were not able to complete treatment due to treatment related stress. For anesthesia, we have routinely applied EMLA cream with lidocaine 2.5% and prilocaine 2.5% under occlusion for 40~50 minutes. In some cases, lidocaine injection was added. Many Asian parents disapprove of the use of general anesthesia and its avoidance was initially thought as an advantage of IPL treatment over surgery. However, our results suggest that local anesthesia may not be sufficient for IPL on CMN, especially in young children.
Unlike most lasers, IPL has a large spot size (15 mm×35 mm in case of Lumenis One™) and is convenient in treating bigger lesions22. From our experience, it took less than 5 minutes to treat small to medium sized CMN with IPL. Initially, the combination of broad wavelength, the ms pulse duration, and the large spot size of IPL was felt very much suitable for CMN treatment. IPL alone or in combination with Er: YAG laser effectively decreased the clinical pigmentation and destroyed the superficial nevus cells without significant scarring. Unfortunately, due to the persistence of the deep nevus cells, there was high recurrence. Compared to CMN, acquired melanocytic nevi are more superficially located, and may be successfully removed with IPL alone or in combination with Er: YAG1824.
There are a number of limitations to our study. The small sample size and restriction to Asians limit the generalizability of our results. In addition, our study was also not able to present the effect of IPL alone on CMN in a number of cases due to the limited efficacy of IPL on its own. Also, there has been no objective standardized assessment tool of clinical images for pigment reduction and also lacks a control group.
Despite the limitations, we feel that our study is meaningful in that it is the first large-scale study to evaluate the efficacy and safety of IPL application on CMN. The findings of this study suggest that IPL alone and in combination with Er: YAG laser are not definitive treatments and should not be considered as the first-line treatment.








 XML Download
XML Download