

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Thyroid carcinoma is the most common endocrine malignancy and the incidence has increased continuously1. Thyroid fine-needle aspiration biopsy (FNAB) is a reliable, safe, and cost-effective screening test and recommended study for evaluation of thyroid nodules23. Post-FNAB local pain and minor hematomas are the most common complications, while serious complications, such as infection, recurrent laryngeal nerve palsy, hemangioma, and tumor implantation seem to be rare3.
A 34-year-old woman presented with an asymptomatic, solitary, bean sized bluish nodule on the right anterior neck for 6 months. Five years ago, thyroid ultrasound examination revealed a solitary nodule on the right thyroid lobe. Ultrasound-guided FNAB performed on the thyroid nodule and she underwent right lobectomy with regional neck dissection. Pathological findings showed that the tumor was a papillary adenocarcinoma of the thyroid. After surgery, she regularly visited the hospital for follow-up and last visit revealed nonspecific findings.
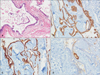
A subdermal nodule was noted about 3 cm above the operation scar line, at the site where aspiration needle had been inserted (Fig. 1). We removed the nodule with elliptical excision. Pathologic findings showed a well demarcated nodule consisting of many tumor cells with multiple follicular structures. Nuclear features demonstrated apparent ground glass, nuclear pseudoinclusions appearing as sharply outlined acidophilic formations, and nuclear grooves (Fig. 2A). In order to identify the tumor origin, immunohistochemical stain with cytokerain 19, thyroid transcription factor-1 (TTF-1) was positive and thyroglobulin was focal positive (Fig. 2B~D). The nodule was highly suggestive of papillary thyroid carcinoma caused by needle tract dissemination and she was transfered to another hospital for further evaluation.
Implantation metastasis through the needle track is a rare complication of FNAB and the incidence range is between 0.003%~0.009% of all FNABs4. Most reported cases are pancreatic, hepatocellular, prostatic cancer or mesotheliomal cell and melanoma. Several cases of implantation metastasis after FNAB of thyroid carcinoma have also been reported45. The interval between FNAB and implantation has been shown to be widely variable, ranges from 1 month to 7 years5. The cutaneous implantation doesn't not affect the prognosis of the disease, because it can be surgically removed without recurrence5. In order to minimize the risk of skin implantation, it is recommended to use a 23-gauge or smaller needle and to release suction before needle withdrawl45.
Although incidence of spontaneous metastasis of thyroid carcinoma is higher than implantation metastasis, we concluded that implantation is more likely for the several reasons in our case: (i) the recurrent tumor occurred at the insertion site of FNAB; (ii) implanted nodule was located above the surgical line; (iii) recurrent tumor was an absence of accompanying lymphoid or neurovascular tissue; and (iv) there was a central bluish papule on the implanted lesion, which suggestive of a previous needle injury45.
We describe a case of cutaneous implantation metastasis of the papillary thyroid carcinoma following FNAB. If physicians discover the skin lesion at the site of FNAB during follow up, they must keep in mind the possibility of cutaneous implantation metastasis after FNAB.

 XML Download
XML Download