

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
The lymphatic system, a subset of the venous circulation system, has various functions in the human body including defense against invading organisms and regulating the pressure of the interstitial fluid.
Injury to this system may induce lymphatic leakage into the tissue and therefore, a collection of lymphatic fluid, which is called lymphocele, can occur1. It is generally known as a complication usually seen after major surgery involving the genitourinary, gynecologic organs, or chest. However, lymphocele can also be encountered as a rare complication after skin biopsy procedures.
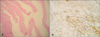
A 29-year-old woman was referred to our clinic presenting with a spontaneously arisen non-tender subcutaneous nodule on her left inner thigh (Fig. 1A). Lipoma was clinically suspected and the sequential excisional biopsy result confirmed the diagnosis. The lesion seemed to be totally removed after the biopsy. However, a palpable nodule developed on the biopsy site after few weeks of follow-up. At first, it was thought to be a scar and she underwent several sessions of intra-lesional steroid injection at 2-week intervals. Despite of the treatment, the lesion kept increasing in size and a subcutaneous cyst was suspected instead of the scar at this point (Fig. 1B). Total excision was planned to remove the cyst. However, upon incision on the lesion, collection of serous fluid came out. After removal of the surrounding remnant tissue, wound was closed but the cystic nodular lesion recurred within a week (Fig. 1C). Fluid aspiration was performed repeatedly and the lesion site was compressed using elastic bandage for a month. The lesion has improved and shows no recurrence until now (Fig. 1D). Histologic examination of the excised tissue suggested a type of pseudocyst and further evaluation revealed the dilated lymphatic channels with flat endothelium that stains for D2-402 (Fig. 2). We concluded that this cyst-like lesion to be a lymphocele caused by an injury on main lymphatics. In this case, initial excisional biopsy of the deep seated lipoma might have injured the lymphatic channel alongside the great saphenous vein of the inner thigh, resulting in lymphorrhea. There is no consensus on effective treatment for post-procedural lymphocele until now1. In majority of cases, lymphocele is spontaneously reabsorbed, but otherwise may develop to be a potentially serious complication1. Few cases proved the improvement after an application of polidocanol foam sclerotheraphy or compression therapy1. In our case, prolonged compression for a month was effective.
Reported cases of cyst formation secondary to trauma or surgery include epidermal cysts to rare metaplastic synovial cyst in literatures3. In addition, to our knowledge, sentinel lymph node biopsy-related lymphatic complications in melanoma-affected patients were the only published reports on dermatologic field45. We report this rare case to highlight the lymphocele that developed after an excisional biopsy in inner thigh, near the great saphenous vein. Therefore, caution is needed when one performs a surgical procedure on the predictable course of great lymphatics, such as inner thigh.

 XML Download
XML Download