

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is a common chronic inflammatory skin disease that is triggered by specific allergens, such as house dust mites (HDM). Allergen-specific immunotherapy has recently been reported to be an effective treatment for AD12. Allergen-specific immunotherapy is classified into two treatment modalities according to the method of allergen administration: subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT)3. Compared to SCIT, SLIT has not been well validated, and there are conflicting data regarding the use of SLIT for treating AD2. However, a few recent reports have shown that SLIT is a viable alternative to the classic injection route45. To date, no study has assessed the efficacy and safety of SLIT for AD patients in Korea. Therefore, we aimed to investigate the efficacy and safety of SLIT in Korean patients with AD.
MATERIALS AND METHODS
Patients
This was an open-label, non-controlled, non-randomized pilot trial in Pusan National University Hospital from July 2011 to September 2014. The study was approved by the institutional review board of Pusan National University Hospital (No. E-2015039), and all the patients were given informed consent. A total of 34 patients with a diagnosis of AD (by Hanifin and Rajka criteria) who presented with positive results to the specific immunoglobulin (Ig)E testing (ImmunoCAP®; Phadia, Uppsala, Sweden) to Dermatophagoides pteronyssinus (DP) and D. farinae (DF) (Class ≥3) were included in this study. Patients were excluded for having uncontrolled or severe asthma, having significant co-morbid disease such as cardiovascular disability, and using beta-blockers. Patients with AD were classified in two groups according to the number of sensitized allergens: mono-sensitized patients (sensitized to only DP and DF) and poly-sensitized patients (simultaneously sensitized to HDM and other allergens proven by a multiple allergen simultaneous test immunoblot assay (Polycheck Allergy®; Biocheck GmbH, Münster, Germany). AD patients who presented with mild to moderate severity (eczema area and severity index [EASI] score ≤20) after cyclosporine induction therapy (3~4 mg/kg for 2~4 weeks) were included.
Immunotherapy
Patients with AD received SLIT (DP and DF mix extracts, 200 standardized treatment units/dose, SLIT one®; ALK-abello, Hørsholm, Denmark) for at least 12 months. The daily dose was a volume of 0.2 ml per single-dose container. Drops were held under the tongue for 2 minutes and were then swallowed. Patients were prohibited to drink or eat any foods for 5 minutes after swallowing the drops.
Measurement of clinical efficacy and rescue medications
The clinical efficacy of SLIT was evaluated by changes in EASI score. Responders were defined as patients with ≥30% improvement of EASI scores after SLIT. Levels of total serum IgE and specific IgE to DP and DF were measured at baseline and after 12 months of SLIT. Clinical response and adverse effects were checked after 1, 3, 6, 9, and 12 months of treatment. Topical tacrolimus 0.1% ointment/pimecrolimus 1% cream and oral antihistamines were allowed during SLIT. Short-term therapy with oral cyclosporine (3~4 mg/kg) was permitted in the case of worsening pruritus, itching, edema, or oozing.
Statistical analysis
Only patients who received SLIT over 12 months were included in the analysis. Statistical analyses were performed using PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA), and a p-value of <0.05 was considered to indicate statistically significant differences. The Mann-Whitney test was used to test changes in EASI scores, total IgE serum levels, and specific anti-HDM IgE serum levels.
RESULTS
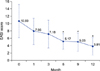
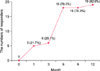
The demographics of all patients are summarized in Table 1. Twenty-three patients continued SLIT for 12 months or more, whereas 3 patients (8.8%) dropped out because of exacerbation of dermatitis, and 8 patients (23.5%) were lost to follow-up. Thirteen of the patients were male, and 10 were female (mean age, 20.6 years). The average duration of SLIT was 22.4 months (range, 12~32 months). Compared with baseline scores, there was a significant reduction of EASI scores after 6 months (p<0.05; Fig. 1). This presented a 51.6% reduction in EASI scores. A total of 18 (78.3%) patients were considered responders to SLIT after 6 months (Fig. 2).
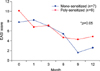
In contrast, there were no significant differences in age, gender, disease duration, severity, total IgE level, and positivity to DP/DF between responders and non-responders after 12 months (p>0.05) (data not shown). Total and specific IgE serum levels did not show significant reduction (p>0.05; Fig. 3, 4). The reduction in EASI scores between the mono-sensitized and poly-sensitized groups was not significantly different (p>0.05; Fig. 5). During the treatment, no patients experienced serious adverse events, with the exception of two patients who suffered from transient lip and tongue swelling. The above minor adverse effects disappeared spontaneously without treatment.
DISCUSSION
AD is a T-cell-mediated chronic inflammatory skin disease associated with cutaneous hyperreactivity to environmental antigens, such as HDM6. The mechanism of action underlying SLIT with DF extract is hyposensitization to the allergen. SLIT leads to decreased numbers of specific T cells, increased production of interleukin-10, and enhanced protection from DF-induced skin inflammation7.
The indication of SLIT in allergic rhinitis and asthma is well-established in adults and children, regardless of the allergen considered8. However, there have been few studies investigating the use of SLIT for AD. Recently, a few studies34910 have reported that SLIT resulted in clinically significant improvements in those with AD compared to those in healthy individuals (Table 2). Our study demonstrated a significant reduction of EASI scores, which supports the results of these previous reports. Cadario et al.4 reported that 51 patients (51/86, 59.3%) responded to SLIT after 12 months. In our study, the responder/non-responder ratio was higher than that in a previous report4. We think that the reason for this high ratio of responders in our study may be partially because we allowed patients to use topical treatment and rescue medication for AD exacerbations. However, despite these biases in our study, SLIT showed favorable results for treating patients with AD.
There is no gold standard serological or laboratory test for assessing the severity of AD. However, several studies of specific immunotherapy for AD reported changes in levels of IgE, IgG4, and cytokines in the blood11. While Cadario et al.4 presented that total and specific IgE values decreased significantly after SLIT, other researchers512 reported no significant difference in IgE values. Our study showed that the levels of total and allergen-specific IgE remained unchanged during treatment. Serum IgE levels are thought to correlate with the severity of AD, but additional studies are still needed to identify the influence of specific immunotherapy on IgE levels.
Criteria for the selection of SLIT indicate that mono-sensitized patients are ideal candidates13. However, our results demonstrated that the reduction in EASI scores between the mono-sensitized and poly-sensitized groups were not significantly different. Moreover, SLIT with mixed DP and DF extract showed a similar effect on poly-sensitized patients with AD in our study. As the sample size of the current study was relatively small, and there have been few clinical trials of SLIT in poly-sensitized AD patients, more clinical studies are necessary to determine the efficacy of SLIT in mono- and poly-sensitized patients with AD.
SLIT is known to have a better safety profile than SCIT, and no fatality has been reported in clinical trials1415. Local side effects, such as itching or mild edema in the mouth and/or throat, have been frequently reported. Only two patients developed transient lip and tongue swelling in this study, and these adverse effects resolved when the treatment was temporarily stopped. Moreover, we did not observe any serious systemic reactions or anaphylaxis. Three dropped out patients experienced an exacerbation of AD from the result. Rather than stopping cyclosporine, we assume that SLIT itself may have influenced on exacerbation as it was mostly identified after every re-administration of SLIT.
In conclusion, our study shows that SLIT with HDM extracts is effective and tolerable in Korean patients with AD, as shown by the significant overall reduction of EASI scores. Additional controlled long-term trials with larger patient populations are required to reinforce these current results in Korea.




 XML Download
XML Download