

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The high prevalence of allergic diseases including allergic rhinoconjunctivitis and allergic asthma is associated with considerable direct individual morbidity as well as high societal costs including loss of productivity. Allergic rhinitis affects 37.6% of the population in Korea.1 In Sweden, the prevalence is estimated at 24% and the loss of productivity due to rhinitis was estimated at 2.7 billion EUR per year.2 It was the most costly disease in the United States with an estimated at $593 USD per employee per year in lost productivity (absenteeism+unproductive) without accounting for the cost of asthma excerbations.3
Cats and dogs are the most prevalent household pets. Allergic responses to other animals are thought to be similar. Among dog allergic adults who have dogs, acute asthma care costs are estimated to add $500 million to $1 billion in the USA.4 The ability to accurately identify susceptible individuals to dog and cat induced exacerbations is critical to decrease the burden of allergic asthma by allowing a better assessment of effective therapies.
The diagnosis and treatment of patients with allergies to dogs continues to be a challenge in contrast to cats. It has been assumed that continuous exposure to animal allergens lead to allergic sensitization, and progression to clinically relevant allergic symptoms. Allergy to dogs and cats has long been considered a major risk factor in the development of allergic rhinitis and asthma.5 However, mounting evidence over the past decade suggests that early exposure to dogs before a year of age may have a protective effect in preventing allergic sensitizations.56 Similarly conflicting studies have been reported for early cat exposures,7 and to date, there is no consensus regarding animal exposure and preventing later onset of asthma or other allergic diseases.8 Studies also differ on the impact of cats or dogs as being most protective.9
Domestic animals are one of the most common allergen that children are sensitized to worldwide. The prevalence of sensitization to cats and dogs in Asia varies. In Korea, dog sensitization is estimated at 15.7% for adults who participated in the Korea National Health and Nutrition Examination Survey (KNHANES) from 2010 to 2012.10 In other Asian countries, sensitization was: 12.2% to cats and 8.9% to dogs in Sri Lanka;11 and 30.8% to cat hair and 34.5% to dog hair in the Zhengzhou district of China.12 Interestingly, sensitization was found to be 11.8% to dog hair and 8.1% to cat hair in the developed region compared to 7.1% and 8.7%, respectively in the developing region of the Pearl delta in Guangdong, China13 supporting environmental studies linking western urbanized lifestyles to increased sensitization.14 In contrast, sensitization assessed by skin prick test (SPT) in European school children to dogs was 8.7% in 1992 while in 2006 it was 15.6% (P<0.001).15 The prevalence of positive dog and cat immunoglobulin E (IgE) individuals >6 years in the USA has been reported at about 12% in National Health and Nutrition Examination Survey (NHANES) 2005–2006 with co-sensitization in those individuals of 78%.16
The prevalence of animal sensitization has increased in the USA,16 Europe,15 Asian countries,1718 and worldwide.14 The absolute numbers may vary depending on which tests were used, but the upward trend is clear. Compounding this problem, pet ownership continues to increase. Nearly 22% of South Korean households in 2016 had at least one pet, up from 17.4% 5 years earlier, a trend that has been fueled by the rise in single-person households.19 Increasing numbers of sensitized individuals along with increasing dog ownership will lead to more affected people. The identification of dog allergic individuals is critically important since exposure to dog allergens in dog sensitized individuals increased bronchial hyper-responsiveness and a susceptibility to asthma attacks.20 Interestingly, dog and cat allergen exposure is ubiquitous even in public places.2122
The current mainstay method to reduce allergic symptoms is to limit exposure to allergens. However, studies over the last 2 decades suggest that early introduction of pets at home may reduce the likelihood of developing sensitization.6 Similarly, food allergy research more recently is advocating early introduction of peanuts as a protective intervention.23 Further study is still required to define the timing and level of exposure to provide protection. But, since it has been well established that continuous exposure in patients with established pet allergy leads to persistent symptoms, it is critical that they be identified. Given the universal presence of detectable pet allergens, the ability to avoid dog and cat allergens therefore, may not be an effective treatment strategy in allergic individuals whereby persistent exposure leads to increased morbidity and mortality.
The ability to truly study dog induced allergic symptoms requires the accurate and consistent identification of sensitized individuals which, to date, is still lacking. Advances in allergy diagnosis and treatment have progressed with cats, grasses, and dust mites, but there has been slow progress in treating dog allergies. Studies on the diagnosis and treatment of dog allergies remain inconsistent and difficult to generalize even though dog allergies are a pervasive problem. This review will focus on the current state of diagnosing cat and dog sensitization and future directions.
Diagnostic challenges in defining clinical allergy to dogs
In clinically relevant allergy, individuals suffer reproducible hypersensitivity reactions with exposures to an allergen at a dose tolerated by non-allergic individuals. Diagnosis has routinely involved obtaining a good medical exposure history coupled with detection of sensitization. The presence of allergic sensitization has been identified using serum specific IgE or SPT with extracts. Historically, quantifying symptoms after exposure challenges such as: induction of asthma with measurement of spirometry changes/peak flows; allergic rhinitis with nasal peak flow; and conjunctival provocation with tear formation have not been used in clinical practice, only in allergen research. These valuable tests clinically assess reactivity to specific allergens at the organ where it affects and should correspond well to natural exposure. More recent provocation testing in individuals with negative skin testing and normal serum specific aeroallergen IgE testing have identified IgE antibodies in the nose and therefore these individuals suffer from locally induced allergic rhinitis.24 Because provocation tests are time and resource intensive, they are usually available only in large research settings, but may be needed in individuals who have persistent symptoms with exposure who are skin test and specific IgE negative.
Evaluating for dog sensitization is significantly more complex and challenging than for cats. The correlation between serum IgE to dog and skin testing is poor with only 52.2% agreement and a correlation coefficient r=0.04.25
In vitro assays have sensitivities averaging 70%–75% for most other aeroallergens compared with symptoms induced after either natural or controlled challenges while other suggest specificity ranging from 30%–95% overall.26 Most clinicians use a specific IgE cutoff level greater than 0.35 kU/L in defining sensitization. Data suggests lower levels of detection may improve diagnostic accuracy,27 but those results are rarely reported.
There remains great difficulty in using SPT for detecting dog allergic patients. Commercially available dog extracts used in skin testing is composed of multiple proteins and their potency in extracts can vary considerably, by up to 1,000-fold.27 Dog component allergens have been identified in serum, dander, pelt, hair, saliva, and urine. Extracts prepared from dog liver, serum, salivary glands, and keratinocytes contain fewer IgE binding allergens compared to dander. Initial studies that showed the importance of the dog component allergen Can f 1 suggests that dander is the preferred source for most commercial dog allergen extract preparations,28 but not all companies use that source and there is no idea on the amount of other component allergens present.
Considerable variation in SPT results depending on the extract used in testing.29 The concentrations of clinically relevant individual dog protein allergens may not be at a high enough level and the source material may not contain the appropriate amounts of allergens leading to false negatives. Though patients report considerable symptoms with exposure, commercial crude allergen extracts show slight positive or even negative results.30 Dog crude extracts are not standardized and the amounts of identified allergens in each extract are unclear.
Increasing the confounding factors, crude dog allergen extracts are contaminated with other allergens. Contamination with other allergens that individuals are allergic will cause false positives in both skin testing and in IgE testing when that extract is being used as the target. Allergens such as dust mites have been found in crude dog allergen extracts.31 More effort is required to define what is in each crude extract and improve their purity thereby making skin testing more reliable in identifying sensitized patients. Variations in dog specific component allergens and the contamination with other proteins severely limits the utility of crude dog extracts in SPT to identify sensitized individuals. Unlike allergies to cats, allergies to dogs are significantly less defined and the importance of pure high quality extracts is more critical.
Diagnostic challenges in allergies to cats compared to dogs
Detecting sensitization to cats has been easier than dogs. Purification and characterization of the cat component protein Fel d 1 occurred in 1973 by Ohman et al.32 This has led to measuring class specific antibodies, production of protein specific antibodies used to measure exposure, crude extract standardization, and generation of T cell specific peptides. In individuals who had a positive exposure challenge, 38 of 41 (92.7%) had positive SPTs.33 Compared to a historical recollection of symptoms to exposure, SPT results equal or >3 mm to cat had a sensitivity of 0.90 sensitivity, specificity of 0.90, with a diagnostic accuracy of 0.90.34 The authors also noted that a tenfold dilutions of cat extract reduced sensitivity without significantly improving specificity.34 Concordance between Phadebas RAST and SPT was 94%35 and Pharmacia CAP System and SPT was 91%.36
In cats, Fel d 1 is the most dominant protein cat allergen where up to 96% of all patients react.37 It does not have significant IgE cross-reactivity with other mammalian proteins and the functional role of Fel d 1 in cats remains unknown. While airborne, it is associated with larger particles (>9 µm) but about 23% is carried on small particles (<4.7 µm in diameter) that stay suspended for several days.38 Though Fel d 1 is the most important component cat allergen, others have been identified (Table 1). Crude extracts for cats, therefore, have been more easily standardized since it can be based on Fel d 1, and therefore advances in cat allergy treatment have been more forthcoming.
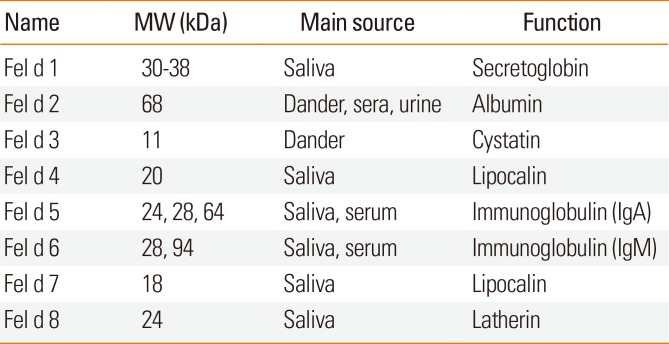
Table 1
Characteristics of cat component allergens
![]()
Unlike cat allergies where most individuals react against one main protein, the diagnosis of dog allergies is more complex. Slowly, individual dog proteins have been isolated and characterized. Currently, there are 7 named dog component allergens identified as Can f 1–7 by the International Union of Immunological Societies that has standardized allergen nomenclature (Table 2). Though many are classified as a “major” allergen, only >50% of allergic patients need to react,39 and of these, no dog allergen has been identified to have the extent of reactivity compared with cat allergic individuals and Fel d 1. Further complicating studies in dog allergies, allergen concentrations vary between breeds and within.304041 Older dogs produce more dander than younger ones because their skin is drier and some breeds are more prone to eczema and oily seborrhea. Seasonal variation also affects the level of dog IgE antibodies.42
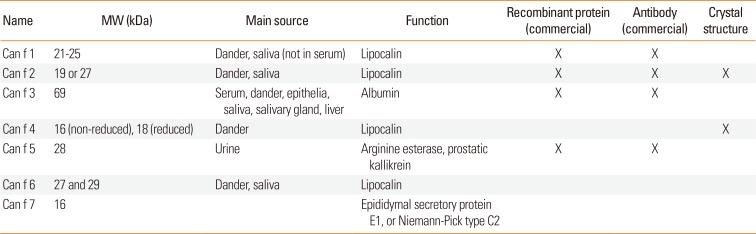
Table 2
Characteristics of dog component allergens
![]()
Molecular based allergen testing
Molecular based diagnosis of allergies is an important advancement in improving sensitivity and specificity43 and will be needed to further define dog sensitization. Assessment of sensitization to allergen components can be done individually (which provides quantitative results on each allergen component), or using an allergen microarray chip (which provides semi-quantitative measurements of IgE antibody binding to numerous components simultaneously). To date, commercially available specific IgE components for dogs (Can f 1, Can f 2, Can f 3, and Can f 5) and for cats (Fel d 1, Fel d 2, and Fel d 4) exists. Studies utilizing component resolved diagnosis in academic studies note that of those who were sensitized, only 64% of adults are Can f 1 IgE positive, with only 32% of those individuals mono-sensitized to Can f 1.44 This suggests that if crude allergen extracts are not sufficiently enrich for each of the other component dog allergen(s), clinicians may be falsely assuming these patients are not dog sensitized.
Diagnosis of allergies based on exposure to specific proteins is known to be critical. Gradually, allergy diagnose is moving away from the crude source of allergens and towards identifying specific causative proteins. For example, the understanding of component allergens in peanuts where Ara h 1, 2, and 3 sensitization is associated with a systemic allergic response in 87% of children with IgE reactivity45 has led to better care. Unfortunately, it will remain unknown what clinical reactions occur with exposure to each dog component allergen without further research. But, individual dog allergen components are slowly being characterized. A greater understanding of the specific proteins that cause specific symptoms based on similar structural features and amino acid sequences may be more important than the exact source of the allergen. In vivo and in vitro testing using the microarray ImmunoCap ISAC technique suggests that allergic sensitization to common pets increases the risk of developing further sensitizations to other furry animals leading to allergies with exposures to them.46 It is clear that sensitization to one allergen predisposes individuals to later sensitization to other aeroallergens, but the mechanism remains unknown. Identification of cross-sensitization with other plants and animals will be important in understanding the development of allergies, how more accumulate, and in clinical management. Advances in linking symptoms caused by specific allergens will improve medical care as tests for a patient's allergen component sensitization profile become more available.
Dog allergen components
Dog lipocalins
Four of the known dog component allergens are in the lipocalin family of proteins: Can f 1, Can f 2, Can f 4, and Can f 6. Lipocalins share a great diversity at the sequence level, but they all have a highly conserved single 8-stranded continuously hydrogen-bonded antiparallel beta-barrel which encloses a ligand-binding pocket. These proteins can bind a range of small hydrophobic molecules and cell surface receptors. Sensitization patterns to each of the dog allergen components are still being defined. Purified proteins have not been used routinely in clinical practice to define the level necessary for a clinical response. Data suggests that individual binding to each component varies: Can f 1 binds 49%, Can f 2 binds 22%, Can f 4 binds up to 35%,47 and Can f 6 binds IgE in 38% of dog sensitized subjects.48 The exact function of each protein allergen component in dogs remain unclear, but analysis of Can f 6 show cross-reactivity with cat (Fel d 4) and horse (Equ c 1).48
Dog albumin
Can f 3 is a serum albumin. It binds IgE in only 16% of dog sensitized patients and cross-reacts with allergens from other furry animals.47 Mammalian albumins cross-react with one another. Cross sensitization to other furry animals via initial allergy to Can f 3 may play a role in the progression to polysensitization and clinical allergies to other animals.
Dog kallikrein
Can f 5 is a member of the kallikrein family of proteins. Kallikreins are a subgroup of serine proteases that act as enzymes which cleave peptide bonds. Although there is no known cross-reactivity to other furry animals, yet cross-reactivity to human prostate-specific antigen has been reported.49 Can f 5 binds IgE in up to 70% of dog sensitized subjects, of those up to 38% did not have antibodies to Can f 1, Can f 2, or Can f 3.49
Dog MD-2 related lipid recognition (ML) family
Can f 7 is a member of the ML family which has been implicated in lipid recognition of pathogen related products. These proteins have an immunoglobulin-like beta-sandwich fold similar to that of Ig domains. Can f 7 is also known as Niemann-Pick disease type C2 protein (NPC2) which has also been previously reported as epididymal protein CE1. NPC2 is an intracellular cholesterol transporter. It is a structural homolog of the human epididymis protein HE1. In Niemann-Pick type C disease, disruption of cholesterol esterification leads to the accumulation of free cholesterol and bis-monoacyl-glycerophosphate that further leads to accumulation of low-density lipoprotein-derived cholesterol in lysosomes which presents as infantile hepatosplenomegaly, while neurologic symptoms appear at 2 to 4 years old.50 The exact role of Can f 7 in dogs remains unclear. Recombinant Can f 7 has been found to bind IgE in 14%–17% (recombinant from yeast and bacteria respectively) of dog sensitized individuals.50
Cat allergen components
Cat secretoglobulin
Fel d 1 is part of a secretoglobulin family that is found only in mammals and is the dominant cat allergen. It is primarily secreted by cat sebaceous glands and therefore is present on the skin surface and fur of a cat. Both short and long hair cats produce it. It is secreted to a lesser extent by salivary gland, lacrimal glands, skin and anal glands. This tetrameric protein is joined together by 2 heterodimers that contain 2 small disulfide linked glycoproteins with chain 1 and 2 containing 70 and 92 amino acids.51 Naturally occurring Fel d 1 is about 38 kDa in size while the recombinant protein is about 30 kDa likely due to 10%–20%-N-linked glycosylation. IgE binding is reportedly conformational and does not involve the carbohydrate residues. The recombinant protein maintains a structure similar to the natural protein and the T cell epitope repertoire has been characterized.52 Data show that Fel d 1 binds the cysteine-rich domain of mannose receptors expressed on antigen presenting dendritic cells suggesting a pivotal mechanism of allergic sensitization to airborne allergens in vivo.53 In 509 cat allergic individuals who had their blood analyzed, positive tests were reported to recombinant compared to natural Fel d 1 at 94.1% and 96.1%, respectively.37 Recombinant Fel d 1 provides a high quality source of purified protein for in depth analysis and characterization that has led to advances in clinical diagnosis and care.
Cat lipcalins
Fel d 4 and Fel d 7 are cat lipocalins. Fel d 4 is found primarily in saliva and is associated with atopic dermatitis in children with cat allergies.54 It is generally accepted that Fel d 4 is the second most frequent sensitized feline protein affecting between 30%–40% of study groups55 to a high of 63%.56 Children sensitized to Fel d 4 were also found to be sensitized to Fel d 1 also, but not vice versa.57 Fel d 7 binds IgE in 38% of cat allergic individuals.58 Fel d 7 share 62% sequence identity with Can f 1 and may suggest a molecular mechanism of cross-reactivity and co-sensitization.
Cat albumin
Fel d 2 is a minor cat allergen with about 15% IgE binding. As with other mammalian albumins, they cross-react. Interestingly, a unique feature of Fel d 2 was discovered through detailed analysis in groups of patients who report pork-cat syndrome who had rapid onset of reactions with eating pork.59 Initial sensitization was though to occur through cat albumin which subsequently resulted in pork albumin sensitization and now allergic reactions.
Management options for dog and cat allergic patients
Current recommendations for controlling clinical symptoms caused by dog and cat allergens primarily includes avoidance to exposures. Bathing animals at least twice per week reduces allergens and can eliminate reactions.60 Immediate removal of the pet from the household will not alleviate symptoms particularly if the owner has carpeting in their home. Mammalian allergens are very stable and persist in house dust up to 6 months.
Symptomatic management with the use of anti-histamines and localized steroids are used when avoidance strategies have been utilized but symptoms still continue. Data on dog allergen subcutaneous immunotherapy (SCIT) show evidence of effectiveness, but is clinically less effective than for cats. This slow introduction of allergens to gradually larger doses and consistent exposure to high levels of allergen during immunotherapy for 3–5 years is associated with changes in T cell function that suggests a shift away from T helper (Th) 2 to Th1 phenotype and induction of regulatory T cells.61 The first studies in dog immunotherapy reported in 1963, showed symptom alleviation in a case series of 11 patients treated with dog extract.62 Since then, numerous trials have been conducted to define the true efficacy of dog immunotherapy. Immunologic markers are altered after dog immunotherapy similar to that seen in cats, but, acetone-precipitated extract containing 15.0 µg of Can f 1 per 0.5 mL maintenance dose was required.63 It is unclear if lower levels of Can f 1 in the other commercial extracts will yield similar results since they only contain around 2.5 µg of Can f 1 per 0.5 mL maintenance dose. In contrast, SCIT for cat allergies have been demonstrated to have clear efficacy. Even as early as 5 weeks, nasal symptom and nasal provocation data showed good response (P<0.001).64
The treatment of dog and cat allergies with immunotherapy depends on reliable and consistent allergen extracts. Unlike cat allergen extracts, differences in the manufacturing of dog allergen extracts exist even today. In the United States, allergens are typically manufactured in an aqueous solution. In Europe, products used for SCIT are usually prepared with aluminum hydroxide which forms a complex with the active allergens and is thought to act as a depot thereby releasing the allergens more slowly. Without adequate standardization, the amounts of different specific protein allergens vary enormously, thus making assessment of therapeutic improvement impossible. Safety of SCIT is also an issue, if a patient is highly sensitive, different manufactured lots even from the same manufacturer with different amounts of component allergen proteins can lead to adverse reactions when those individuals are suddenly exposed to high levels.
Novel therapies under development
Component testing measuring patient specific sensitization patterns to dogs and cats will help determine primary sensitization vs. symptoms due to cross-reactivity. These specific components can also be therapeutic targets. Recombinant proteins, peptides, recombinant hypoallergens which mimic natural proteins but are modified to be less allergenic during immunotherapy, and multimeric recombinant allergens are being developed for use in dog and cat allergic individuals with some showing promise. Of these, linear peptide sequences of native allergens have been studied as a novel method to be used in allergy vaccinations for Can f 1.65 These peptides are thought to be less allergenic since they have a reduced ability to cross link IgE epitopes and thus do not initiate cascades of mast cell degranulation. Linear peptide sequences are hypothesized to induce T cell tolerance through the induction of regulatory T cells that can secrete the immunoregulatory interleukin (IL)-10. But, clinical trials suggest that side effects may still exist with peptide treatments. In subjects given intradermal vaccinations of short overlapping peptides of the major cat allergen Fel d 1, 9 out of 40 (22.5%) exhibited late asthma reactions without early or cutaneous responses that may be major histocompatibility complex (MHC) restricted.66 Further refinement of specific peptides and personalization with an individual's MHC will be important. Since dog allergic individuals are not all allergic to only Can f 1, combinations of the appropriate component allergens will be required for optimal therapeutic interventions. To address this, a multimeric recombinant Can f 1, Can f 2, Can f 4, and Can f 6 allergen was created for diagnostic and therapeutic purposes with initial studies showing promise.67 Although the ultimate goal is effective therapeutic intervention with curative treatments, the inability to accurately diagnose dog allergic individuals severely hampers advances. This key factor of having standarize cat allergen extracts amoung others (Table 3), has faciliated advances in treating cat allergies as compaired to dogs.
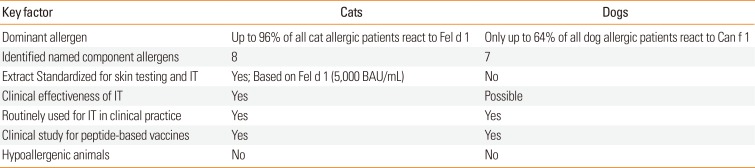
Table 3
Summary of key factors in cat and dog allergies
![]()
Hypoallergenic dog and cats
There has been much debate on the existence of hypoallergenic pets. As noted, of the identified and named specific dog protein allergens, there is none that dominates all others to the extent that Fel d 1 does in cats. Even in cats, there are still 8 specific allergenic proteins that would need to be targeted. The elimination of just Fel d 1 would only help a minority of cat allergic patients who are mono-sensitized to only Fel d 1. Similarly, in dogs, there is concurrently co-sensitization with other dog component allergens most notably Can f 2 with Can f 1. To date, there is no truly hypoallergenic cat nor dog since all of the protein allergens would need to be inactivated.
“Hypoallergenic dog breeds“ though have been used to market dogs that are thought to be less allergenic than other breeds, however, allergen levels vary enormously within breeds and between them.30 The amount of shedding and length of hair are thought to be protective since pet dander and saliva stick to hair and are not released into the environment, but studies find that there was no difference in the air or on the floor.68 In a study measuring the level of allergen Can f 1 via enzyme-linked immunosorbent assay (ELISA) in breeds thought to be “hypoallergenic” (Labradoodle, Poodle, Spanish Water Dog, and Airedale Terrier) found levels in the hair and coat of dogs as well as floor and airborne dust to be similar to non-hypoallergic breeds (Labrador Retriever and a control group).68 As many of these allergens are still being characterized with respect to their allergenicity, their true function in vivo in dogs and cats still remain unclear and inactivating all of them may have a detrimental impact on these animals.
Unmet needs and future directions
Numerous unmet needs continue to plague the diagnosis and treatment of allergies especially to dogs (Table 4). Of primary importance is the need to create a high quality well characterized dog allergen preparation. Currently, different manufacturers use different processes with different raw materials to create crude extracts of uncharacterized quality and content. These products are not generic, but differ widely in compositions and therefore IgE binding capacity.69 This yields widely variable results in IgE testing as well as SPT. No international standard nor standardization method has been developed to date. All the different commercial products perform differently on patients leading to inconsistent results and data. This results in conflicting data that cannot be extrapolated and interpreted on overall dog allergies and the effectiveness of different therapies. Advanced protein isolation techniques should be used to manufacture pure extracts free of contamination with high component allergen protein concentrations. Data suggests that recombinant allergens may be comparable to natural proteins and should be considered.

Table 4
Unmet needs and challenges in allergies to dogs and cats
![]()
The utility of component diagnosis is currently limited to academic studies. Though important, commercial labs detect IgE only to commercially available Can f 1, Can f 2, Can f 3, and Can f 5 and not the entire complement of named dog allergens. Additionally, these components have yet to be characterized in crude extracts used in skin testing for diagnosis and in extract mixtures used in therapeutic immunotherapy. Without adequate quantification of each component, quality studies on the efficacy of immunotherapy (both subcutaneous and sublingual) will be limited. No common structural feature of all allergens has been described due to the limited numbers of clearly defined allergen structures. Increased characterization of protein allergens will lead to better information regarding cross-reactivity thereby helping in the counseling of patients. The definition of an allergen is based solely on the ability of eliciting an IgE response in susceptible individuals. Future directions dictate continued utilization of 2-dimensional (2D) gel electrophoresis coupled with mass spectrometry when screening serum of individuals with clinical symptoms to dog exposure to identify potentially novel allergens. Continued efforts should be committed to fully characterizing these proteins including resolution of their native structure with confirmation not just of their immunogenicity, but also their true clinical allergenic nature with the use of provocation tests. Evidence suggest that each component allergen protein may illicit a unique symptom profile which needs to be defined. Longitudinal studies are required to define which component is protective, at what level, and which induces localized, systemic, or asthmatic symptoms.
Go to : 
CONCLUSION
The use of allergen immunotherapy over a 3–5 year period of treatment leading to persistence of tolerance thereafter has been shown to be cost effective.70 Data has predominately been based on well characterized allergens such as in cat allergies, but has been extrapolated as being effective with other allergens. Significant advances have been achieved in the diagnosis and treatment of cat allergies that should be applied to advance science of allergies to dogs. Inconsistent and contaminated extracts may not be identifying all dog allergic individuals and conversely may also be identifying individuals who are not dog allergic, but sensitized to the contaminants in the extract. Appropriate medical management is not utilized and avoidance guidelines are therefore not reviewed with those patients resulting in sustained morbidity as continued exposures occurs. Direct evidence on the benefits of immunotherapy with current crude dog extract is limited. Expanded molecular diagnosis of component dog allergens will improve diagnosis and treatment of patients. It is critically important to define the exact molecular allergens that each individual is susceptible since there are dramatic implications in the development of allergic disease as well as treatments. New, improved, and pure dog extracts are needed to improve the diagnosis of dog allergies and the effectiveness with dog specific immunotherapy.
Go to :
 XML Download
XML Download