

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic spontaneous urticaria (CSU), a subtype of chronic urticaria (CU), is defined as episodes of recurrent spontaneous wheals and/or angioedema lasting more than 6 weeks.1 A population-based study of Korea reported that the crude prevalence of CU was 2,256.5 per 100,000 person-years and tended to increase every year between 2010 and 2014.2 Hospital-based study of Korea showed that the prevalence of CU in children is 1.8%, which appears to be similar to that in adults.3 CSU impairs quality of life by affecting many aspects of quality of life, such as sleep and daily activities, and has considerable humanistic and economic impacts.45
Second-generation antihistamines are the first-line agents for the treatment of CSU, and omalizumab (Xolair®; Genentech, Inc., South San Francisco, CA, USA) 300 mg/month is recommended for antihistamine refractory patients in whom high-dose antihistamines fail to control symptoms. Cyclosporin (Sandimmune®; Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA) is recommended for patients who are unresponsive to both antihistamines and omalizuamb.6 Although knowledge of the clinical course of CSU is important clinically for determining patient prognosis and assessing its social and economic burden, it remains unclear. The purpose of our study was to investigate the clinical course of CSU in the Korean adult population using insurance claim data. To our knowledge, this is the first study on the clinical course of CSU using a nationwide database.
Go to : 
MATERIALS AND METHODS
This is a population-based study using the Korean National Health Insurance Service National Sample Cohort (NHIS-NSC) 2002-2013 from the Korean National Health Insurance Service (KNHIS). This database is composed of approximately 1 million nationally representative random subjects and includes all medical claims from 2002 to 2013, and details of database is previously described.7 The KNHIS uses International Classification of Disease, Tenth Revision, Clinical Modification codes.
We used the same definition of CSU as a previous report from our group.8 This definition was validated to have a positive predictive value of 90.4% and a sensitivity of 71.1%.9 We made the CSU group who fulfilled 1 of the 2 criteria in a year between 2003 and 2007 as previously described.8 We excluded subjects under the age of 20. Also, we excluded subjects diagnosed with CSU in 2002 to ensure that the CSU group only included subjects with new episodes. Each patient in the CSU group was tracked whether he or she went into remission or not until 2013. We defined remission as not being diagnosed with urticaria (L50.1, L50.8, or L50.9) for at least 1 year during follow-up. The last date of CSU diagnosis was defined as the date of remission. Subjects who were no longer available to be followed up due to their death during the study periods were excluded for the survival analysis.
All data are displayed as the number of subjects plus the percentage in each group for categorical variables. Kaplan-Meier survival analysis was carried out to analyze the remission rate, and log-rank tests were performed for between-group comparisons. Demographic differences between subjects who went into remission 1 year after the initial diagnosis and those who did not were analyzed using χ2 tests, and P<0.05 was considered statistically significant. To further estimate differences in gender between individual age groups, we calculated odds ratios (ORs) and 95% confidence intervals (CIs).
Go to :
RESULTS
A total of 13,969 subjects included between 2003 and 2007 were followed up during a median period of 2,471 days. Median disease duration in subjects who underwent remission in the study period was 392 days. Among them, 8,626 (61.75%) were female and 5,343 (38.25%) were male. The proportion of subjects in the 20-39, 40-64, and 65+ age groups were 30.63%, 49.69%, and 19.68%, respectively.
Table displays the basic characteristics of the study population and demographic differences between subjects who went into remission 1 year after the initial diagnosis and those who did not. The proportion of subjects in the 65+ age group (P=0.050) and with male gender (P=0.002) was significantly higher among subjects who did not go into remission 1 year after the initial diagnosis compared to those who did. Subjects aged 65+ showed a significant negative association with 1-year remission state compared to those aged 20-39 (OR, 0.86; 95% CI, 0.77-0.97). Female subjects showed a significant positive association with 1-year remission state compared to male subjects (OR, 1.15; 95% CI, 1.53-1.25).
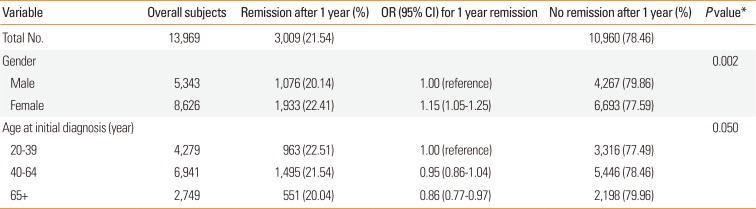
Table 1
Basic characteristics of the study population and demographic differences between subjects who went into remission 1 year after the initial diagnosis and those who did not
![]()
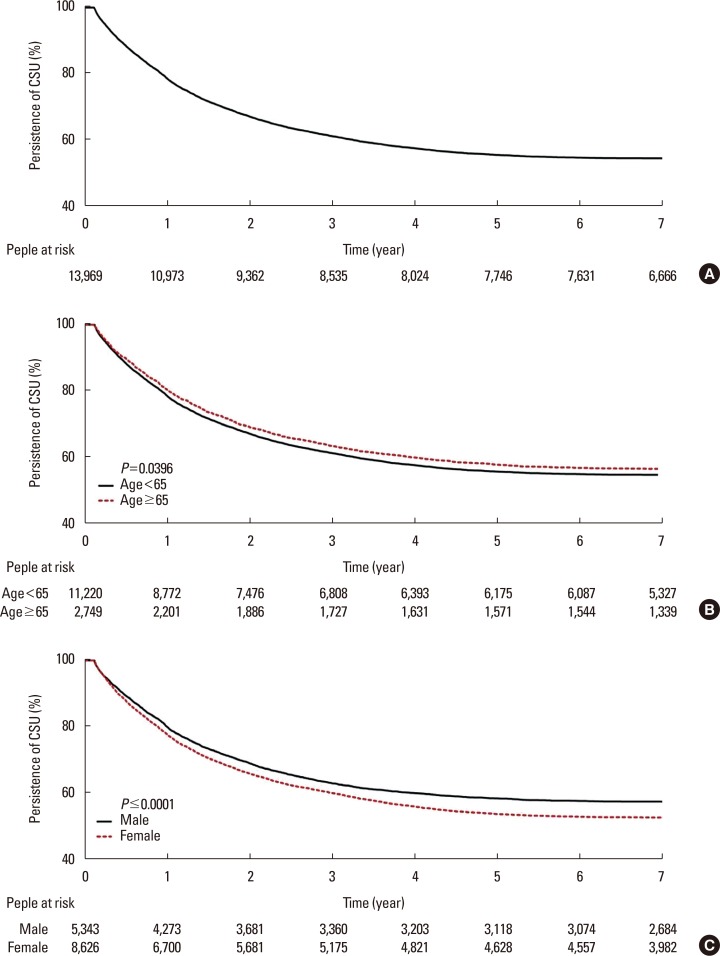
Figure displays the Kaplan-Meier survival analysis of persistence of CSU in the study groups, and between-group analysis. The 1-, 2-, 3-, 4-, and 5-year remission rates of CSU were 21.5%, 33.0%, 38.9%, 42.6%, and 44.6%, respectively. Between-group analysis using the log-rank test showed that there were significant differences in the remission rates of CSU between the 20-64 and 65+ age groups (P=0.040) and between males and females (P<0.001).
Go to :
DISCUSSION
We found that the 1-, 2-, and 5-year remission rates of CSU were 21.5%, 33.0%, and 44.6%, respectively. The clinical course of CSU is unpredictable, and remission rates were variously reported.10 Kozel et al.11 and Kulthanan et al.12 reported that 1-year remission rates of CSU were 35% and 34.5%, respectively. Van der valk et al.13 reported that 5- and 10-year remission rates of CSU were 29% and 44%, respectively. Hiragun et al.14 reported that 1-, 2-, and 5-year remission rates of CSU were 11.5%, 13.9%, and 27.7%, respectively, and Toubi et al.15 reported that 1-, 2-, and 5-year remission rates of CSU were 25%, 48%, and 86%, respectively. The 1-, 2-, and 5-year remission rates found in our study were lower than those in previous studies except for a study by Hiragun et al.14 Their study only included subjects with CSU that was not controlled by a standard dose of antihistamine, which might contribute to the lowest remission rate. In Korea, Ye et al.10 reported that the 6-month remission rate of CSU was 3.4% after treatment according to the guideline. Although remission rate after 6 months was not studied in their study, remission rates were lower than ours. In their study, the study population driven from 3 referral hospitals and relatively strict definition of remission might have contributed to these results.
Previous studies had weaknesses, such as a small sample size with a hospital-based design. Also, they were heterogeneous in terms of the study population, inclusion criteria of CSU, treatment methodology, and definition of remission. Our population-based nationwide study included Korean subjects with CSU, which was defined using disease codes. Not all subjects in our study were treated according to the recent guidelines.1 A multicenter study in Germany found that the majority of CSU subjects were undertreated, had uncontrolled urticaria.16 Likewise, subjects with CSU in our study might be undertreated in real-world practice. Omalizumab has been well demonstrated to safely and effectively control CSU at least partially in approximately 2/3 of cases.17 In Korea, omalizumab was not approved for the treatment CSU in the study period, which could have contributed to lower remission rate. Because this is an observational study, not an interventional study, it is hard to evaluate to the effect of treatment modalities on the prognosis of CSU. The definition of remission used in our study was relatively strict. We speculate that these reasons might influence the lower remission rates found in our study.
In this study, an age of 65+ and male gender were poor prognostic factors affecting the remission rate. However, previous studies reported that age or gender did not affect the clinical course of CSU in the adult population.101418 On the other hand, angioedema, severe CSU, antithyroid antibodies, and/or positive autologous serum skin test findings have been reported to be poor prognostic factors for CSU.101415
This study has some limitations. First, the diagnosis of CSU was defined on the basis of disease codes. Subjects with defined CSU in our study had a possibility that they did not be diagnosed with CSU in real-world practice. Furthermore, medical visit does not assure active urticarial symptoms. Secondly, information on use of over-the-counter medications was unavailable. Thirdly, because the remission rate was defined by disease codes, remission state might have been interpreted as the condition not requiring medical intervention. Also, recurrence of CSU might occur after the defined remission state. Fourthly, right censoring that some patients did not undergo remission state at the end of the study should be considered in the interpretation of the results. However, as this database contained data from 2002 to 2013, each patient was followed up for at least 6 years, which could have contributed to the value of our results. Despite these limitations, our nationwide study included a large number of subjects from the primary care clinics to the referral hospitals.
In summary, our population-based, nationwide study demonstrated that the 1-, 2-, and 5-year remission rates of CSU in the Korean adult population were 21.5%, 33.0%, and 44.6%, respectively respectively. An age of 65+ and male gender were found to be poor prognostic factors for CSU. These results indicate that CSU may have a more persistent course than previously reported.
Go to :
 XML Download
XML Download