

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atopic dermatitis (AD) is a common chronic inflammatory skin disease frequently accompanied by other atopic diseases and has a substantial impact on the quality of life of affected patients and their families.1 Mild AD can be adequately controlled with basic skin care, environmental control and topical medications. However, moderate-to-severe disease requires more comprehensive and systemic management.2 To date, there has been a paucity of published evidence to guide such approaches. Although there are reports and guidelines regarding the management of AD in Korea,34 differences in the patterns of AD management according to physicians' specialties have never been investigated.
The present study was conducted to identify management patterns in Korea for moderate-to-severe AD, including diagnostic tools, use of laboratory tests and treatment strategies, according to the physician's specialty, namely, allergists, pediatric allergists and dermatologists.
Go to : 
MATERIALS AND METHODS
Study subjects
This questionnaire study was administered to physicians from the Korean Academy of Asthma, Allergy and Clinical Immunology (KAAACI), Korean Academy of Pediatric Allergy and Respiratory Disease (KAPARD), and Korean Atopic Dermatitis Association (KADA). This study was approved by the Institutional Review Board of Seoul Medical Center (approval No. 2016-028).
Contents
The questionnaire consisted of 31 questions divided into 7 sections. We obtained data regarding the demographic and professional characteristics of the respondents, including age, sex, specialty and type of practice hospital. Subjects were asked to report the proportion of pediatric patients they treated (0–5, 6–12 and 13–18 years old) and whether they used skin or serologic testing for specific immunoglobulin E (IgE). For severity assessment, the Eczema Area and Severity Index (EASI) or SCORing Atopic Dermatitis index (SCORAD) was employed.
Survey participants were asked to denote the necessity and feasibility of treatment options including basic skin care of bathing with moisturizing, and avoidance of triggering factors. In addition, education and consultation by medical staff, psychologists or dietitians, and use of topical medications and oral antihistamines were included in the treatment options. Furthermore, providers were asked whether they prescribe nutritional supplements with probiotics, vitamin D, essential fatty acids and zinc. Providers were also asked to indicate their preference for the following systemic treatment options: wet wrap therapy, systemic corticosteroids, cyclosporin, azathioprine, methotrexate, mycophenolate mofetil, interferon-γ and phototherapy.
Finally, the questionnaire explored the use of various treatment guidelines to direct the management of AD as well as perceived barriers to comprehensive treatment of AD.
Statistical analysis
Data analysis was performed using STATA version 10.0 (Stata-Corp., College Station, TX, USA).
Go to :
RESULTS
Study population, practice site and physician characteristics
Ninety-three participants completed the full survey. The demographic and professional characteristics of the respondents are depicted in Table. In total, 40.9% were women; the majority were pediatric allergists (64.5%), 31.2% were dermatologists, and the remaining 4.3% were allergists. Regarding age, 33.3% were in their forties, 28% in their thirties, another 28% in their fifties, and 10.8% in their sixties. Most of the participants (87.1%) worked in university teaching hospitals, and 12.9% in other types of hospitals.
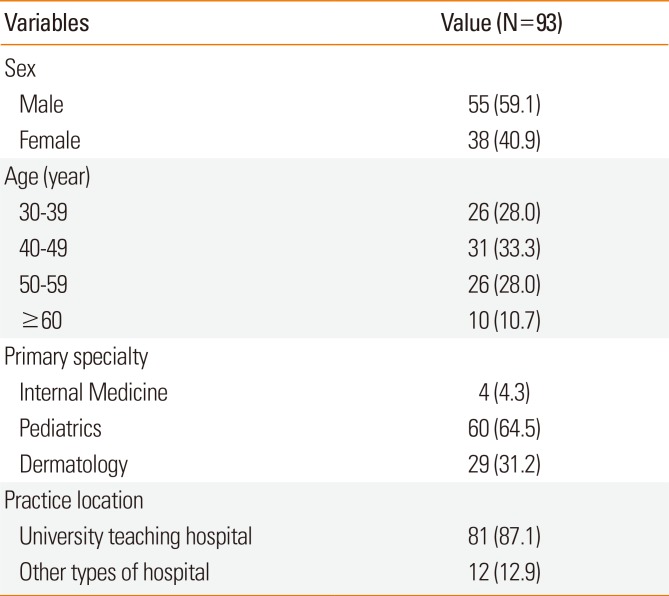
Table
Demographic and professional characteristics of the participants
![]()
Distribution of patient age groups and proportion of moderate-to-severe AD
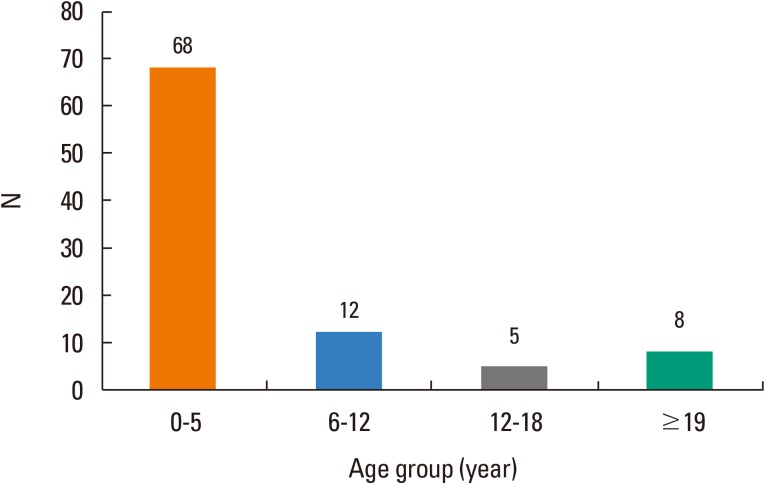
A total of 68 respondents (73.1%) reported that their major patient age group was “less than 5 years,” while 12 (12.9%), 8 (8.6%) and 5 (5.4%) respondents reported that their major patient age group was “6–12 years old,” “more than 19 years old” and “13–18 years old,” respectively (Fig. 1). All of the pediatric allergists responded that their major patient age group was aged “less than 5 years” (100%, 60/60). The major age groups were “6–12 years old” for dermatologists (38%, 11/29), and “more than 19 years old” for allergists (75%, 3/4).
Thirty-nine respondents (40.8%) reported the proportion of moderate-to-severe AD in their practice as “10%–25%,” while 24 (25.8%), 19 (20.4%), and 1 (1.1%) respondents reported the proportion as “26%–50%,” “<10%”, and “>51%,” respectively.
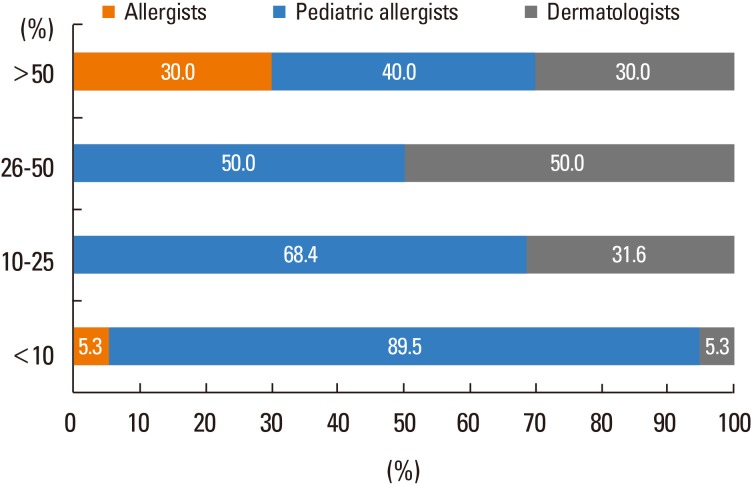
The proportion of moderate-to severe AD was higher in the practices of dermatologists and allergists, compared to pediatric allergists. Twenty-six pediatric allergists (43.3%) reported that the proportion of moderate-to-severe AD in their practice was “10%–25%,” and 30% (18/60) reported the proportion was “<10%.” On the other hand, 41% of dermatologists reported that the proportion of moderate-to-severe AD they treated was “10%–25%,” and another 41% answered that the proportion was “26%–50%.” In the case of allergists, 75% (3/4) reported that the proportion of moderate-to-severe AD in their practice was “>51%,” while 25% (1/4) reported that the proportion was “<10%.”
The percentages of respondents who reported that the proportion of patients with moderate-to-severe AD in their practice was “less than 10%” were 89.5% for pediatric allergists, 5.3% for dermatologists and 5.3% for allergists. The percentages who reported that the proportion of such patients they saw was “10%–25%” were 68.4% for pediatric allergists, 31.6% for dermatologists and none for allergists (Fig. 2).
Outcome measures for severity assessment and allergy tests
Most respondents (76.3%) utilized the EASI for measuring AD severity, whereas some (19.4%) preferred the SCORAD. To detect allergen-specific IgE in serum, ImmunoCAP (Phadia, Uppsala, Sweden), the multiple-antigen simultaneous test (MAST) (Hitachi Chemical Diagnostics Inc., Mountain View, CA, USA) and skin prick testing were performed in 82 (88.2%), 70 (75.3%), and 57 (61.3%) participants, respectively.
Gap between ideal and real-world practice for AD treatment modalities
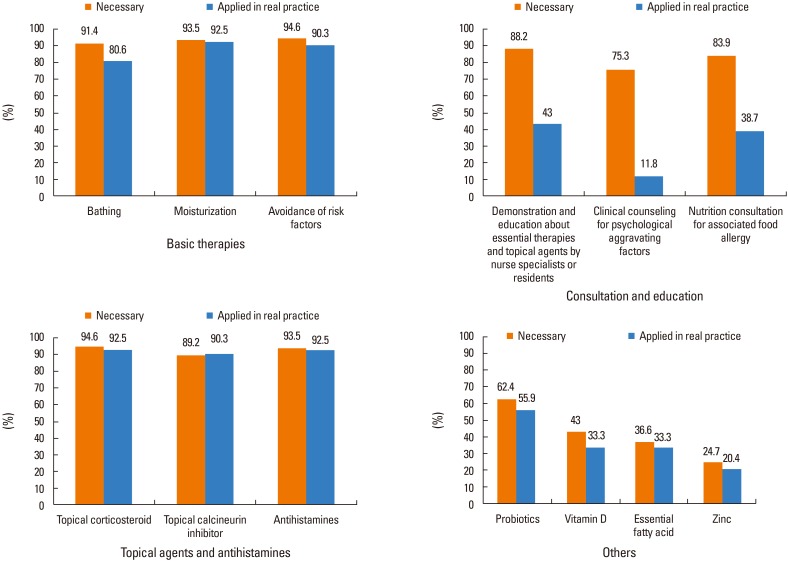
Basic skin care including proper bathing, moisturizing and avoidance of triggers are appreciated as the necessary treatment modalities by most respondents. However, the perceived necessity and the actual application of proper bathing were 91.4% and 80.6%, respectively.
Respondents agreed on the necessity of education including the demonstration of basic skin care and application of topical therapies (88.2%), nutritional consultation (83.9%), and psychological counseling (75.3%). However, less than half of physicians conducted education and counseling in real practice.
The percentages of respondents who regarded topical corticosteroids and topical calcineurin inhibitors as necessary were 94.6% and 89.2%, respectively, and the percentages who prescribed them in real practice were 92.5% and 90.3%, respectively. Regarding antihistamines, 93.5% of respondents thought they were necessary and 92.5% actually prescribed them in real practice. For other supplementary measures including probiotics, vitamin D, essential fatty acids and zinc, 62.4%, 43.0%, 36.6%, and 24.7% of the respondents considered each of them necessary, and 55.9%, 33.3%, 33.3%, and 20.4% of the respondents used them in real practice, respectively (Fig. 3).
Preferred systemic treatments for severe AD according to specialty
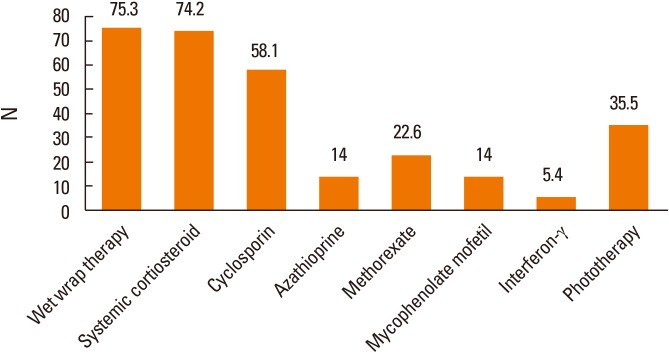
Among all respondents, preferred systemic treatments for moderate-to-severe AD were wet wrap therapy (75.3%), systemic corticosteroids (74.2%), cyclosporin (58.1%), and phototherapy (35.5%) (Fig. 4).
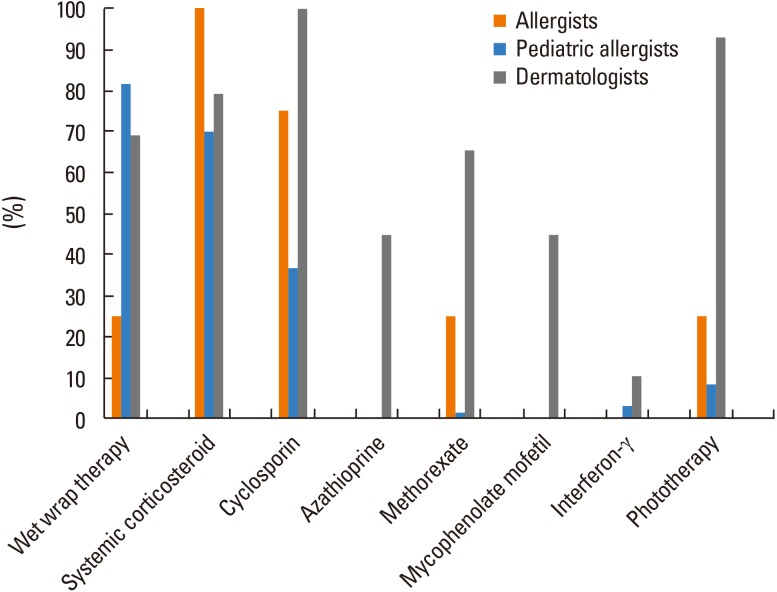
For pediatric allergists, the order of preferred systemic treatment was wet wrap therapy (81.7%), systemic corticosteroids (70.0%), and cyclosporin (36.7%). However, dermatologists ranked cyclosporin (100%), phototherapy (93.1%), and systemic corticosteroid (79.3%) as first-line treatment regimens for moderate-to-severe AD. Allergists preferred systemic corticosteroids (100%), followed by cyclosporin (75%) (Fig. 5).
Preferred guidelines for AD management
The KAPARD guidelines for the management of AD5 were preferred by the greatest number of pediatric allergists (96.5%), followed by the guidelines from the European Academy of Allergy and Clinical Immunology (EAACI)6 (89.7%), and the guidelines from the American Academy of Allergy, Asthma and Immunology (AAAAI)7 (86%).
In contrast, the greatest number of dermatologists favored the guidelines of the European Academy of Dermatology and Venereology (EADV)8 (58.8%), followed by the KADA guidelines9 (57.1%), and the guidelines from the American Academy of Dermatology (AAD)10111213 (56.7%) (Fig. 6).
 | Fig. 6Preferred guidelines for treatment of AD according to the physician's specialty. EADV, European Academy of Dermatology and Venereology; EAACI, European Academy of Allergy and Clinical Immunology; AAD, American Academy of Dermatology; AAAAI, American Academy of Allergy, Asthma and Immunology; KADA, Korean Atopic Dermatitis Association; KAPARD, Korean Academy of Pediatric Allergy and Respiratory Disease.
|
Barriers to comprehensive treatment of AD
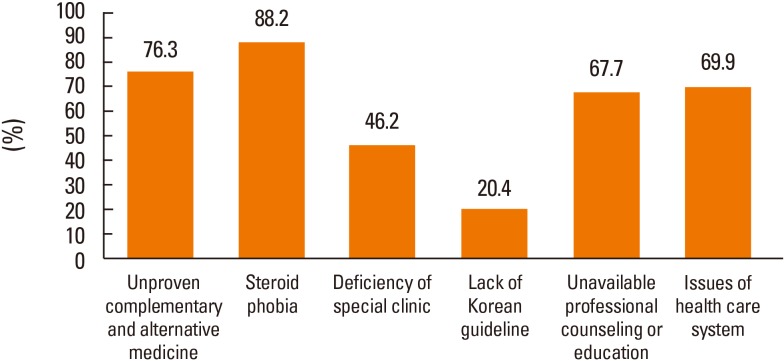
The major factors quoted as barriers to the proper management of AD were steroid phobia (88.2%), unproven complementary and alternative medicine (76.3%), the unreasonable insurance system (69.9%), and a lack of education (67.7%). In addition, some respondents also regarded deficiency of special clinics for AD (46.2%) and a lack of proper Korean guidelines (20.4%) as barriers to the comprehensive management of AD (Fig. 7).
Go to :
DISCUSSION
The pathophysiology of AD is highly complex, and heterogeneous phenotypes are described in terms of different features such as age of onset, severity, IgE sensitization, comorbidity and variable response to conventional treatment.1415 Although there is a lack of consensus regarding management for patients with moderate-to-severe AD, difficult-to-manage patients should be referred to an AD specialist.7 Based on the heterogeneity of this disease and its variable clinical presentation, cooperation between allergists, pediatric allergists and dermatologists is important in the implementation of strategies for the care of patients with moderate-to-severe AD. The KAAACI Work Group on Severe/Recalcitrant Atopic Dermatitis previously suggested the necessity of personalized and comprehensive approaches to severe/recalcitrant AD in a previous report.3 However, there have been significant barriers to proper management in real practice. The present survey provides insight into practical AD management according to physicians' specialties in Korea. As the members of the KAAACI and KAPARD were invited to participate in this questionnaire-based survey, the data obtained in this study might represent the current management practices of consultant physicians in Korea.
Our data showed distinct differences in the age groups and AD severity of the patient populations according to respondents' specialties. Younger children aged less than 5 years are the major patients for pediatric allergists, and 89.5% of pediatric allergists reported that the proportion of moderate-to-severe AD in their practice was less than 10%. On the other hand, the major patient group for dermatologists was “older than 5 years,” and the proportion of moderate-to-severe AD in their practice was relatively higher.
In a previous questionnaire-based survey in Korea, physicians working in secondary and tertiary hospitals were found to perform more allergy tests compared to primary care physicians (89.0% vs 45.8%, respectively), irrespective of their specialties.16 Although most clinicians and patients agreed on the necessity of measuring allergen-specific IgE in the initial assessment of AD,1718
in vivo (skin prick test) or in vitro (ImmunoCAP and MAST) tests were performed in only 59.9% of patients as reported in our other previous study.17 In the present study, 88.2% of respondents employed ImmunoCAP, a finding comparable to previous results focused on secondary or tertiary hospitals.
Saavedra et al.19 reported that significant and distinct differences in AD management patterns exist among physicians according to specialty. Allergists reported greater use of laboratory tests (IgE, skin prick and elimination diet) compared to pediatric allergists and dermatologists. For infants and toddlers with AD, most pediatric allergists and allergists employed formula change as a strategy in some populations, whereas dermatologists favor a pharmacologic approach. Dermatologists utilized higher-potency anti-inflammatory agents more frequently than pediatric allergists or allergists. In comparison, as the present study shows, Korean physicians tend to prescribe short-term systemic therapy more frequently for the treatment of acute exacerbation of early onset AD.
Although there is no universal agreement on the definition of severe/recalcitrant AD, severe disease can be regarded as AD recalcitrant to potent anti-inflammatory topical medications and associated with a considerable impact on quality of life from a clinical point of view. There is a wide variation in prescribing practices or approaches to severe AD, according to a European survey.20 In a recent systematic review, strong recommendation was only possible for the short-term use of cyclosporin A among 12 different interventions for moderate-to-severe AD in 34 randomized controlled trials.21 The present survey identified distinct variations in prescribing patterns of systemic treatment for moderate-to-severe AD. Pediatric allergists preferred wet wrap therapy, systemic corticosteroids and cyclosporin, in decreasing order of frequency. Dermatologists prescribed cyclosporin, phototherapy and systemic corticosteroids as first-line treatment regimens. Although in our study, allergists most strongly preferred systemic corticosteroids, which requires confirmation due to the small sample size. We found that wet wrap therapy was mostly employed by pediatric allergists and dermatologists. Regardless of physicians' specialties, systemic corticosteroids are chosen by most respondents as a first-line treatment regimen; however, phototherapy is mainly preferred by dermatologists. Some dermatologists prescribed azathioprine, methotrexate, mycophenolate modefil and interferon-γ as first-line treatment regimens, but pediatric allergists and allergists rarely used these treatment options. Considering age group and severity of patients according to physician specialty, pediatric allergists may deal with more cases of acute exacerbation rather than chronic persistent lesions. In addition, the questionnaire did not clearly distinguish acute exacerbation and moderate-to-severe cases. Nevertheless, these results confirmed that systemic corticosteroids are still the major systemic treatment regimen in Korea for moderate-to-severe AD, consistent with those of previous surveys in patients.1617
As expected, the preferred referral guidelines for the management of AD varied according to specialty. This finding reflects the differences in approach depending on the physician's specialty. For example, diluted bleach bath, vitamin D, and environmental intervention are more emphasized in the AAAAI guidelines than in the AAD guidelines. In a recent European survey20 investigating the use of systemic therapy in children with severe/recalcitrant atopic eczema (AE), dermatologists were significantly more likely to initiate systemic agents compared to pediatric allergists. The researchers also reported that the first-line systemic agents of choice were cyclosporin and oral corticosteroids, comparable to our results.
Our previous study17 showed that appropriate explanation and education based on the test results were not provided to patients and caregivers. Therefore, the accuracy in determining trigger factors and patient satisfaction fell short of expectations. The reasons for hesitating to perform allergy testing in primary clinics could be lack of testing personnel or facilities, lack of belief regarding the clinical importance of allergy testing in the treatment, and difficulty in explaining the test results to patients.1617 The significant burden of chronic diseases on the quality of life of patients and their caregivers as well as the relative complexity of the treatment frequently result in therapeutic failure due to poor adherence. Therapeutic patient education and a comprehensive approach to the treatment of AD are aimed at improving the therapeutic adherence of patients and their caregivers.2223 Many patients acquire indiscriminate or inadequate disease information through various forms of media, without expert supervision.24 However, 70.1% of patients surveyed in a previous study demonstrated willingness to participate in an expert-led education program in a hospital.17 By means of in-depth counseling and education, factors that reduce compliance could be identified and reflected in treatment strategies through multidisciplinary approaches in AD management.2526 In the present study, basic skin care including bathing, moisturization avoidance of risk factors was relatively well employed in real practice. However, demonstration and education about essential therapies and topical agents, clinical counseling for psychological aggravating factors, and nutritional consultation for associated food allergy were not actually implemented well, although they were thought to be essential. Experts have limitations in realizing this ideal approach, associated with insufficient time for education about the disease due to low economic compensation compared to physician's effort. Therefore, medical policy changes and institutional/governmental support are required, considering the high prevalence and psychosocial burden of AD.
There have been compelling but unproven and false beliefs regarding AD and, in particular, a misleading belief on steroid use (steroid phobia) is still widespread.24 Aubert-Wastiaux et al.27 reported that topical corticosteroid phobia was present in 80.7% of AD patients/parents, regardless of disease severity and duration. In a survey on the topical steroid prescriptions of dermatologists,28 45% of the respondents assumed that more than half of the outpatients have topical steroid phobia, and 73% of the respondents in private clinics and 62% in secondary and tertiary hospitals were influenced by patients' negative attitudes toward topical steroid prescription. Concordant with the previous patients/parents survey,27 our study showed that 82% of the respondents ranked steroid phobia as the biggest hurdle to comprehensive treatment of AD, followed by unproven complementary and alternative medicine, an issue related to the unreasonable healthcare system, and absence of professional counseling education. These barriers could lead to poor compliance with treatment and may impact disease outcome. Thus, well-organized patient education should be provided to encourage treatment adherence.
There are several weaknesses of this study. First, our sample size is small and the proportion of moderate-to-severe cases is not high. Secondly, there may be bias in the selection of respondents as we did not perform random sampling.
In summary, we found that there are distinct differences in preferred treatments for moderate-to-severe AD in real practice according to physicians' specialties. Even experts experience many limitations in implementing the ideal approach; therefore, medical policy changes and institutional/governmental support are needed considering the high prevalence and psychosocial burden of AD. We suggest that there is an unmet need for a personalized, evidence-based and multidisciplinary approach including therapeutic patient education in AD in real practice.
Go to :
 XML Download
XML Download