

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Food allergy (FA) affects 6% of adults1 and up to 8% of children. The prevalence of allergy and anaphylaxis is increasing.23 Standard management has been strict food avoidance and preparedness with an epinephrine auto-injector (EAI) in the event of a reaction.4 Despite efforts at avoidance, severe reactions may occur in up to a third of food allergic children.5 Given risk for accidental reactions and persistence of FA beyond childhood, there is an unmet need for therapies for FA. A number of allergen-specific methods are being studied, and may become commercially available in the coming years. In this review, we will discuss food allergen-specific immunotherapies (AITs) that are being evaluated in humans.
Go to : 
SECTION 1: WHAT ARE THE METHODS OF AIT FOR FA?
AIT utilize frequent delivery of allergen via various routes to induce tolerance. Food AITs currently under study include oral immunotherapy (OIT), sublingual immunotherapy (SLIT), epicutaneous immunotherapy (EPIT), and subcutaneous immunotherapy (SCIT) with modified allergen, as well as lysosomal-associated membrane protein (LAMP)-DNA based vaccines. An overview of these AIT modalities is provided below and compared in Table 1.
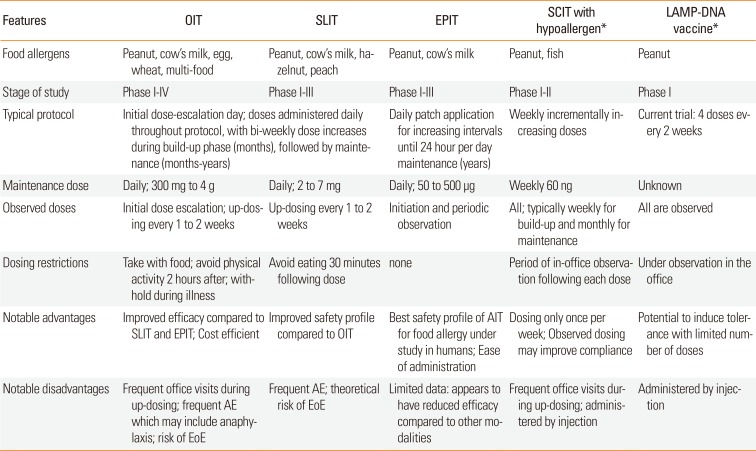
Table 1
Comparison of allergen-specific immunotherapies for food allergy currently under study in human subjects
![]()
OIT and SLIT
In OIT, native or modified food allergen is ingested; whereas in SLIT, liquid allergen extract is applied under the tongue. SLIT and OIT respectively start with sub-threshold doses in 0.0001 µg- and 0.1 mg-range, which are increased under physician supervision during an initial rapid dose-escalation day up to 0.01 µg-range and mg-range. The highest tolerated dose after initial dose-escalation may be repeated on the following day to confirm it will be safely tolerated during daily doses at home. This is followed by a build-up phase during which daily doses are increased every 2 weeks under physician supervision up to maintenance doses in mg-range for SLIT and gram-range for OIT. Daily maintenance dosing is continued for months to years.
EPIT
In EPIT, 50–500 µg (usually 250 µg) of food protein electrosprayed onto a patch is applied to the upper arm or interscapular space. EPIT protocols typically start with 2 hours of patch application under clinician supervision in the office. Thereafter, daily patch application continues at home, with duration of application increased incrementally up to 24 hours per day. During maintenance, a new patch is applied daily and worn 24 hours per day for 1 or more years.67
SCIT
In SCIT, allergen is administered by subcutaneous injection in incrementally increasing doses under clinical supervision. Current SCIT trials utilize alum-adsorbed hypoallergen which has been modified chemically or with site-directed mutagenesis to reduce immunoglobulin (Ig) E-binding capacity.8
LAMP-DNA vaccines
In LAMP-DNA vaccines, DNA encoding allergen is administered in bacterial plasmid vectors, which express both the allergen epitope and LAMP-I for enhanced immunogenicity. They are administered by intramuscular or intradermal injection, every 2 weeks for a limited number of doses.
Go to :
SECTION 2: IMMUNE MECHANISMS
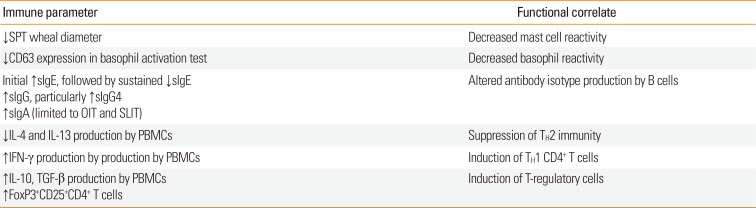
Immune mechanisms by which AIT may induce tolerance are not fully elucidated. The observed changes in immune function (Table 2) appear to hinge on altered allergen-specific T-cells responses, with induction of T-regulatory cells (Tregs) and suppression of TH2 immunity. Mechanisms of alteration in T-cell phenotype through AIT are discussed below and summarized in Fig. 1.
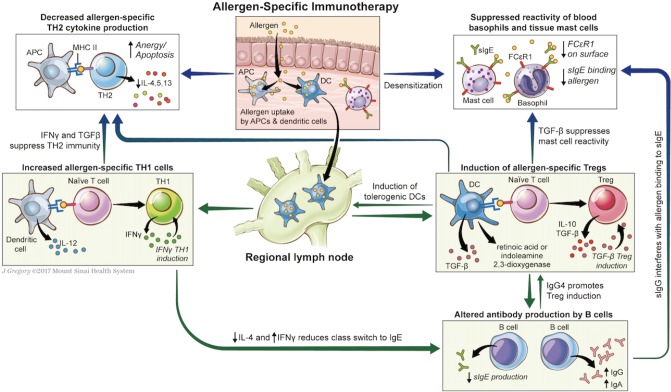 | Fig. 1Putative mechanisms of tolerance induction in allergen-specific immunotherapy. In allergen-specific immunotherapy (AIT), native or modified allergen is taken up by dendritic cells which migrate to regional lymph nodes, where they induce naïve T cells to regulatory T cell phenotype, through presentation of the allergen in context of MHC, secretion of cytokines such as TGF-β, generation of retinoic acid and indoleamine 2,3-dioxygenase, and other mechanisms. Secretion of cytokines IL-10 and TGF-β suppress TH2 immunity and mast cell reactivity, reduce sIgE synthesis, and may increase sIgG and sIgA synthesis. AIT, particularly with LAMP-DNA vaccines, may also enhance tolerance through increased TH1 immunity: presentation of allergen by dendritic cells in context of MHC to naïve T cell may induce TH1 commitment particularly in presence of costimulators; production of IFN-γ by TH1 cells suppresses TH2 responses and reduces class switch to IgE. Other mechanisms of AIT may include increased anergy and apoptosis of TH2 cells through persistent antigenic stimulation.
|
Table 2
Immunomodulation in allergen-specific immunotherapy
![]()
Natural tolerance acquisition and that conferred by AIT with native allergen appear to occur through induction of Foxp3+ Tregs. Antigen uptake by immature tissue-resident dendritic cells (DC) in the absence of costimulatory signals results in DC-mediated Treg induction, through secretion of immunosuppressive cytokines and other mechanisms.910 These induced-Tregs suppress allergic responses through secretion of inhibitory cytokines (interleukin [IL]-10, IL-35, and transforming growth factor [TGF]-β), which further amplifies Treg induction. Tregs also express surface receptors which alter DC function and induce target cell senescence.11
Immunotherapy appears to induce a shift away from TH2-predominant immune responses, with reduced allergen-specific production of TH2 cytokines.61213141516 This may occur not only through the immunosuppressive effects of Tregs as elaborated above, but also through a shift towards TH1 immunity.61718 TH1 cytokines such as interferon (IFN)-γ specifically inhibit TH2 immunity and IgE production. Alternative mechanisms include anergy and deletion of allergen-specific TH2 cells through repeated and frequent exposure to high doses of allergen.19
OIT
OIT utilizes the mechanisms underlying oral tolerance, resulting in suppression of allergic responses (Fig. 2). Oral tolerance is likely dependent on induction of Tregs within gut-associated lymphoid tissue.920 The steps through which this occurs include delivery of antigen to lamina propria DC by goblet cells (or other mechanisms); antigen uptake by CD103+DC in the intestinal lamina propria; CCR7-directed migration of DC to mesenteric lymph nodes (MLNs); and interaction between DC and T-lymphocytes within MLNs.920 B-regulatory cells may also play a role in tolerance induction.21 The role of Tregs, B-regulatory cells, and DCs in oral tolerance has recently been reviewed in detail.20
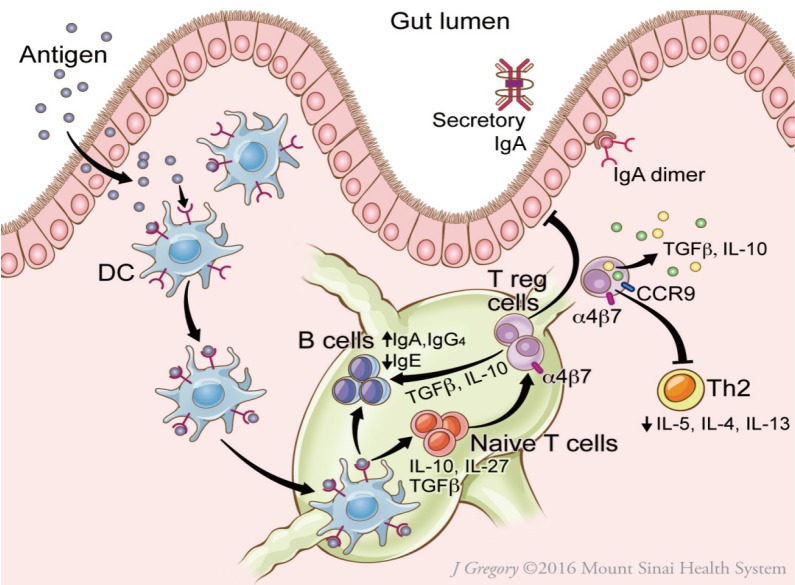 | Fig. 2Putative mechanisms of oral tolerance induction in the gut. On passage through the epithelial barrier, food protein allergen is captured by the dendritic cell (DC). The DC migrates to the nearby mesenteric lymph nodes and produces TGF-β, IL-10, and IL-27, which induce T regulatory cells (Tregs) and promote secretion of IgA and IgG4 by B cells. Tregs express surface receptors CCR9 and α4β7 integrin, which direct migration to the gut. Tregs secrete immunosuppressive cytokines IL-10 and TGF-β, which reinforce tolerance. Reprinted from Journal of Allergy and Clinical Immunology: In Practice (Volume 5), Gernez Y and Nowak-Wegrzyn A, “Immunotherapy for Food Allergy: Are we there yet?”, Page 253, 2017, with permission from Elsevier.
|
OIT is associated with reduced skin prick test (SPT) wheal diameter and reduced basophil reactivity, initial increase followed by a gradual decrease in antigen-specific IgE, sustained increase in antigen-specific IgG4 and antigen-specific IgA, decreased allergen-specific production of TH2 cytokines (IL-4, IL-13), increased allergen-specific production of TH1 (IFN-γ) and Treg cytokines (TGF-β), and Treg induction.61722232425262728 It appears however that some of these immunologic changes may be transient, with reversal on withdrawal of therapy and sometimes during maintenance.2327
SLIT
SLIT utilizes the tolerogenic environment of the oral mucosa. Langerhans cells (LC; skin- and mucosa-homing DC) rapidly take up antigen, which has been transported across sublingual ductal epithelial cells.29 LC migrate to local lymph nodes, where they present allergen to naïve T cells, inducing Tregs through secretion of immunosuppressive cytokines IL-10 and TGF-β.30
EPIT
EPIT is purported to induce tolerance through prolonged application of antigen to intact, non-inflamed skin. In mice, antigen applied to skin is taken up by LC in the stratum corneum and transported to draining lymph nodes, where these LC induce Foxp3+ Tregs locally.32 Treg induction also appears to occur distally with generation of gut-homing LAP+Foxp3− Treg cells, which provide sustained protection against anaphylaxis through direct TGF-β-dependent Treg suppression of mast cell activation.33
SCIT
The mechanisms underlying tolerance induction for SCIT with alum-adsorbed hypoallergen may differ from those for SCIT with native allergen. In SCIT with native allergen, immune tolerance is induced by similar mechanisms described above, with antigen-uptake by immature subcutaneous DC, migration of DC to local lymph nodes, Treg induction by tolerogenic DC, and Treg-mediated suppression of TH2 immune responses.35 In SCIT using hypoallergen, alum-adsorption provides a costimulatory signal that promotes a TH1 response, which also serves to inhibit TH2 immunity. In murine and rabbit studies, subcutaneous immunization with hypoallergenic carp parvalbumin (Cyp c 1) resulted in increased sIgG and decreased sIgE antibodies; and inhibition of IgE-binding, basophil degranulation, and allergic symptoms on challenge.3637
In the only published results of SCIT with hypoallergen for FA in humans, a 2017 abstract reported evidence of immunomodulation with increased peanut-specific IgG4 in subjects treated with subcutaneous injection of chemically modified alum-adsorbed peanut (HAL-MPE1) compared to controls.38
LAMP-DNA vaccines
LAMP-Vax is a next-generation DNA vaccine platform designed to stimulate an immune response against a particular protein, by injecting the DNA encoding the protein. After vaccine administration, antigen-presenting cells (APCs) take up the vector, which translates DNA into allergen associated with LAMP-I.39 LAMP-Vax DNA immunization contrasts with the immune response to conventional DNA vaccines, which are processed and primarily presented through major histocompatibility complex (MHC)-I and elicit a cytotoxic T response. LAMP-Vax DNA immunization initiates a more complete immune response, including antibody production, cytokine release, and critical immunological memory. In the C3H/HeJ peanut allergic mice (sensitized via oral ingestion of peanut and cholera toxin), intradermal injection of 50 µg ASP0892 attenuated allergic symptoms during peanut challenge as indicated by lower disease scores and higher body temperature compared to vector control, reduced peanut-specific IgE levels and increased peanut-specific IgG2a levels.3940
There is currently an ongoing phase I, randomized, placebo-controlled study to evaluate safety, tolerability, and immune response in adults allergic to peanut after receiving intradermal or intramuscular injection of ASP0892 (ARA LAMP-Vax), a single multivalent peanut (Ara h1, h2, h3) LAMP-DNA Plasmid Vaccine (NCT02851277).
Go to :
SECTION 3: DESIGN OF AIT CLINICAL TRIALS
With OIT, SLIT, and EPIT being the focus of most published AIT clinical trials, much of the below discussion is based on published data evaluating these therapies. A general schematic of OIT and SLIT is provided in Fig. 3.
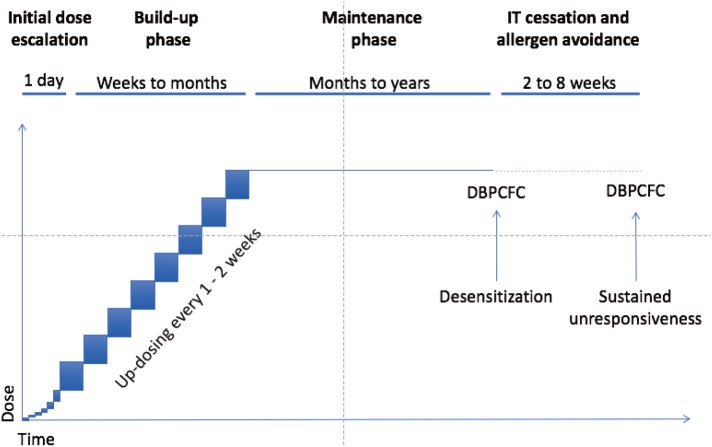 | Fig. 3Typical protocol for oral and sublingual immunotherapy. Initial doses of OIT and SLIT are generally given under medical supervision. Initial dose escalation day(s) starting at subthreshold dose with increasing doses given every 30 minutes over several hours is more common for OIT than for SLIT. Highest tolerated dose given under observation is then continued daily at home, and increased every 1 to 2 weeks under supervision during the build-up phase. The dose achieved at the end of the build-up is continued daily during a maintenance phase. After a few months or years of maintenance, double-blind placebo-controlled food challenge (DBPCFC) to the food is performed to assess for desensitization. Daily dosing may then be discontinued for a period of 4–12 weeks and reintroduced during DBPCFC, to assess sustained tolerance (SU). Reprinted from Journal of Allergy and Clinical Immunology: In Practice (Volume 5), Gernez Y and Nowak-Wegrzyn A, “Immunotherapy for Food Allergy: Are we there yet?”, Page 253, 2017, with permission from Elsevier.
|
Goals of therapy
While the most desired outcome of AIT would be permanent tolerance, clinical trials investigating immunotherapies for FA typically use practical endpoints of desensitization and sustained unresponsiveness (SU). Desensitization is a temporary state of hyporesponsiveness, which is induced and maintained by frequent (daily) exposure to the offending antigen. Immune reactivity may return upon withdrawal of antigen exposure for a sufficient period of time. SU is a prolonged antigen hyporesponsiveness which persists after a period (typically 2–12 weeks) of cessation of therapy and avoidance of allergen.
Design of AIT clinical trials
Shared features of AIT clinical trials
Clinical trials share a number of features. For recruitment, entry criteria typically include a history of reaction to the food or physician-diagnosed FA, with evidence of IgE-sensitization. Typical exclusion criteria include history of life-threatening anaphylaxis, poorly controlled asthma, other form of concomitant immunotherapy, medications that either suppress immune response or increase risk of reactions, and certain chronic conditions. Most of the rigorous studies will require a double-blind placebo-controlled oral food challenge (DBPCFC) to determine the threshold prior to initiation of therapy, to confirm presence of the FA, and to eliminate subjects who are tolerant of the food or reactive to placebo.
For randomized, controlled trials (RCT), subjects are then randomized to AIT or to the control group (placebo and/or strict avoidance of allergen). To evaluate immunomodulation on AIT (Section 3), clinical trials may perform allergen-specific evaluation prior to AIT initiation, at various time-points during the study and at the conclusion of therapy. Therapy protocols are undertaken for various forms of AIT as described in Section 1. Adverse events (AEs) are monitored through out the trial. Subjects may withdraw for any reason. Common reasons include persistent and/or severe AE, anxiety related to doses or oral food challenge (OFC), inability to comply with protocols, or new medical problems or medications.
At the conclusion of therapy, desensitization is typically evaluated with DBPCFC, and reported as the portion of subjects tolerating standardized dose of food or as the increase in the maximum tolerated dose of allergen compared to prior to IT. For those trials also evaluating SU, subjects avoid therapy as well as native food for a period (typically 2–12 weeks) after which DBPCFC is again undertaken. Some trials may report consumption of the food years out from therapy, to evaluate long-term success with AIT.
Divergent features of AIT trials
Direct comparison of results of various studies is hampered by variation in trial design. The following frequently differ between trials: allergic profile of individuals enrolled in the trial; duration of initial dose-escalation, build-up, and maintenance phases as well as avoidance period prior to SU-OFC; daily maintenance dose; and dose administered during OFCs to define desensitization and SU. Though all trials report moderate or severe AE as well as administration of epinephrine, reporting of minor AE may differ, with some trials reporting only what are deemed clinically-relevant dose-related AE, and others with a lower threshold to report minor AE.
Go to :
SECTION 4: ORAL IMMUNOTHERAPY TRIALS
Overview of OIT trials
OIT remains a subject of active investigation, with most trials demonstrating efficacy limited by safety and compliance. Published studies have evaluated OIT with major food allergens, including milk, egg, peanut, and wheat, with safety and efficacy varying by food allergen. In recent years, investigators have evaluated OIT with modified proteins, with multiple foods, and/or combined with immunomodulatory agents.
Efficacy
Oral administration of gradually increasing quantities of food protein during OIT effectively induces desensitization in a majority of food allergic subjects, provided they can tolerate and comply with therapy. A portion of those achieving desensitization go on to demonstrate SU 2–12 weeks post-OIT.122441 For those achieving SU, long-term follow-up studies demonstrate continued consumption of offending food months to years after OIT completion.4243
Safety
The use of OIT in routine clinical practice has been limited by its AE, which are most often mild, but can include anaphylaxis, chronic gastrointestinal (GI) discomfort, and eosinophilic esophagitis (EoE). Safety varies by allergen, with milk carrying increased risk of AE compared to peanut, egg, and perhaps wheat. The majority of subjects experience some symptoms with OIT, including oropharyngeal pruritus, rhinitis, abdominal discomfort, vomiting, urticaria, angioedema, atopic dermatitis flare, cough, and wheeze. Most of the time, these are non-severe and self-resolving; sometimes administration of antihistamine, short-acting beta agonists, or systemic steroids is required. Though uncommon, most OIT trials are accompanied by a few severe reactions requiring administrations of epinephrine. Persistent, frequent, or severe symptoms often interfere with adherence and result in drop-outs accompanying virtually every OIT trial. While severe reactions occur most often during initial dose escalation and build-up, they can occur with home administration of previously tolerated doses. A major development in reducing IgE mediated AE with OIT has been concomitant administration of omalizumab, discussed in section “OIT with omalizumab.”44
Cofactors
Adverse reactions occurring with previously tolerated doses often occur in the setting of cofactors which lower allergic threshold, such as viral infection, febrile illness, active allergic rhinitis in the pollen season, physical exertion, or administration on an empty stomach.454647 To address cofactors, most OIT protocols advise dose adjustments in the setting of viral infection, avoidance of exertion in the hours following a dose, and administration after a full meal.
EoE
A meta-analysis by Lucendo and colleagues48 concluded that EoE may develop in up to 2.7% of OIT subjects, and often resolves on withdrawal of OIT. It is possible that more subjects develop OIT-related EoE than is reported, as some discontinuing OIT for GI symptoms suspicious for EoE are not evaluated with endoscopy.47 It is not clear whether OIT unmasks EoE to the culprit food or increases the likelihood of EoE.
Adherence
OIT requires significant commitment from families and patients in order to adhere to therapy. Families and patients need the flexibility in their schedules and access to transportation to return many times during the protocol. Initial dose escalation may require a full day (or several days depending on the protocol) in an inpatient setting. For build-up phases (which may take weeks to months), patients must return every 1 to 2 weeks for observed dosing. Finally, subjects must take their dose every day for months to years; for patients with taste aversion, parents and patients with anxiety, and families with significant life events, this may prove challenging. As a consequence, most OIT studies report withdrawals from the protocol for issues not specifically related to AE.
Quality of life (QoL)
Despite its risks and frequent adverse effects, OIT appears to improve QoL,49 alleviating risk with accidental exposure, food-related anxiety, and social and dietary limitations.
Cost-effectiveness
Peanut-OIT with probiotic was found to be cost efficient compared to avoidance in a long-term economic model, with an incremental cost-effectiveness ratio of $2,142 per quality-adjusted life year. However, peanut-OIT subjects were more likely to experience peanut-related allergic reactions and anaphylaxis; this appeared to be of particular relevance to subjects who experience a low rate (<25%) of allergic reactions related to accidental exposure, or when probability of SU was less than 68%.50
Details of the specific OIT-studies are presented in the tables; cow's milk (CM; Tables 3 and 5), egg (Tables 4 and 5), peanut (Table 6), and wheat (Table 7).
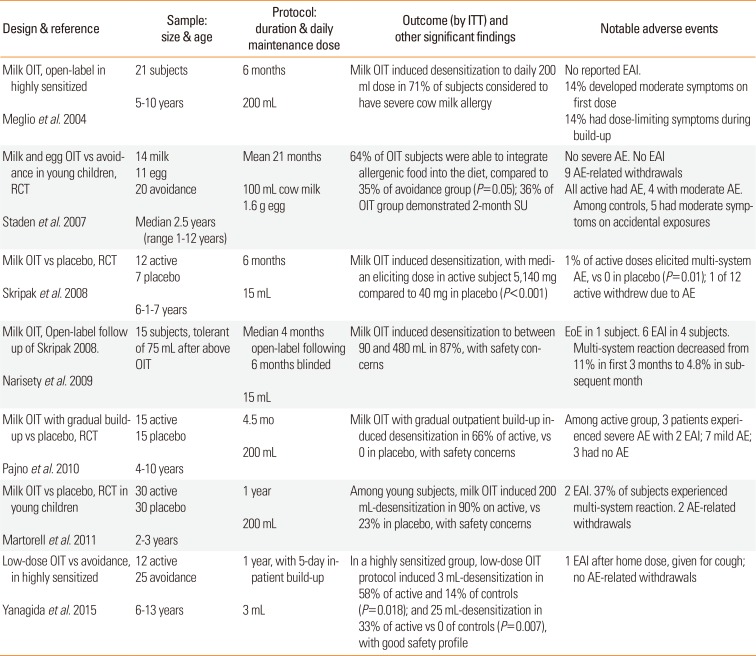
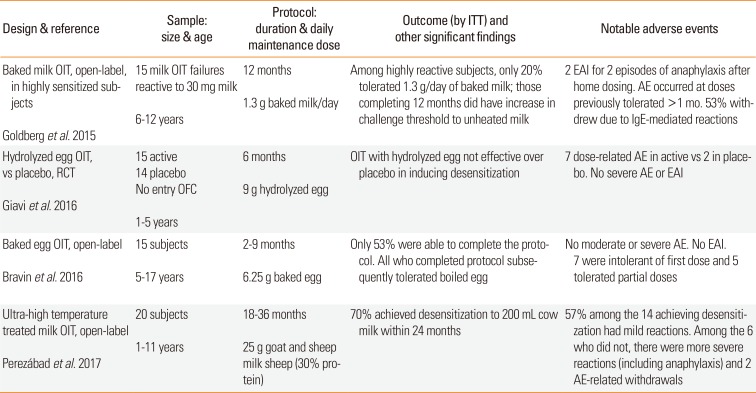
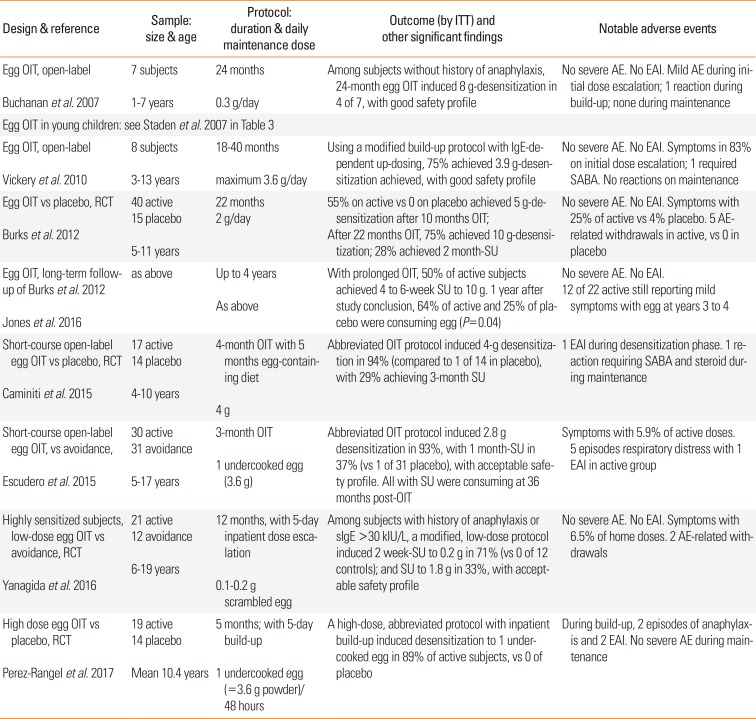
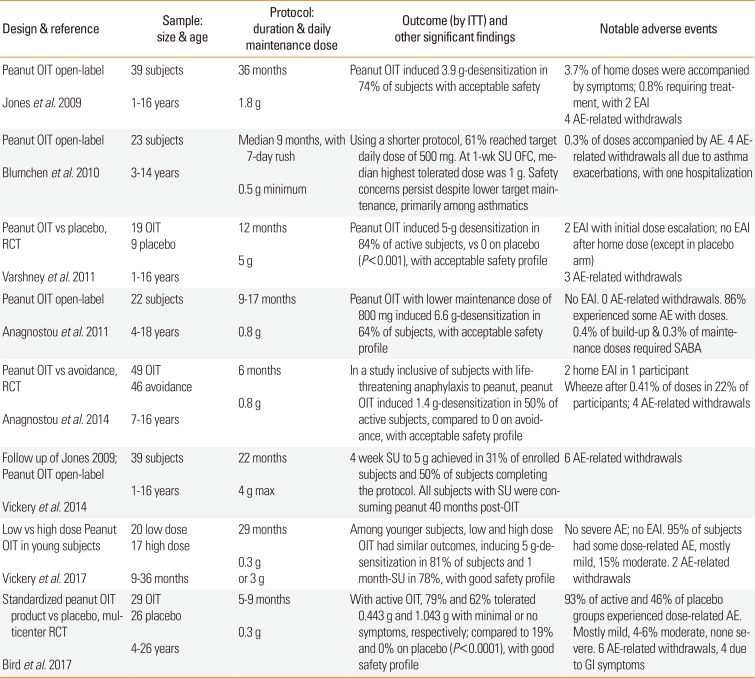
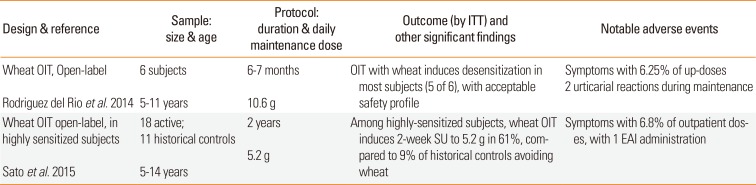
Table 3
Representative milk oral immunotherapy clinical trials
![]()
Table 5
Oral immunotherapy with modified egg and milk proteins
![]()
Table 4
Representative egg oral immunotherapy clinical trials
| Design & reference | Sample: size & age | Protocol: duration & daily maintenance dose | Outcome (by ITT) and other significant findings | Notable adverse events |
|---|---|---|---|---|
| Egg OIT, open-label | 7 subjects | 24 months | Among subjects without history of anaphylaxis, 24-month egg OIT induced 8 g-desensitization in 4 of 7, with good safety profile | No severe AE. No EAI. Mild AE during initial dose escalation; 1 reaction during build-up; none during maintenance |
| Buchanan et al. 2007 | 1–7 years | 0.3 g/day | ||
| Egg OIT in young children: see Staden et al. 2007 in Table 3 | ||||
| Egg OIT, open-label | 8 subjects | 18–40 months | Using a modified build-up protocol with IgE-de-pendent up-dosing, 75% achieved 3.9 g-desensitization achieved, with good safety profile | No severe AE. No EAI. Symptoms in 83% on initial dose escalation; 1 required SABA. No reactions on maintenance |
| Vickery et al. 2010 | 3–13 years | maximum 3.6 g/day | ||
| Egg OIT vs placebo, RCT |
40 active 15 placebo |
22 months |
55% on active vs 0 on placebo achieved 5 g-de-sensitization after 10 months OIT; After 22 months OIT, 75% achieved 10 g-desensitization; 28% achieved 2 month-SU |
No severe AE. No EAI. Symptoms with 25% of active vs 4% placebo. 5 AE-related withdrawals in active, vs 0 in placebo |
| Burks et al. 2012 | 5–11 years | 2 g/day | ||
| Egg OIT, long-term follow-up of Burks et al. 2012 | as above | Up to 4 years | With prolonged OIT, 50% of active subjects achieved 4 to 6-week SU to 10 g. 1 year after study conclusion, 64% of active and 25% of placebo were consuming egg (P=0.04) |
No severe AE. No EAI. 12 of 22 active still reporting mild symptoms with egg at years 3 to 4 |
| Jones et al. 2016 | As above | |||
| Short-course open-label egg OIT vs placebo, RCT |
17 active 14 placebo |
4-month OIT with 5 months egg-containing diet | Abbreviated OIT protocol induced 4-g desensitization in 94% (compared to 1 of 14 in placebo), with 29% achieving 3-month SU | 1 EAI during desensitization phase. 1 reaction requiring SABA and steroid during maintenance |
| Caminiti et al. 2015 | 4–10 years | 4 g | ||
| Short-course open-label egg OIT, vs avoidance, |
30 active 31 avoidance |
3-month OIT | Abbreviated OIT protocol induced 2.8 g desensitization in 93%, with 1 month-SU in 37% (vs 1 of 31 placebo), with acceptable safety profile. All with SU were consuming at 36 months post-OIT | Symptoms with 5.9% of active doses. 5 episodes respiratory distress with 1 EAI in active group |
| Escudero et al. 2015 | 5–17 years | 1 undercooked egg (3.6 g) | ||
| Highly sensitized subjects, low-dose egg OIT vs avoidance, RCT |
21 active 12 avoidance |
12 months, with 5-day inpatient dose escalation | Among subjects with history of anaphylaxis or sIgE >30 kIU/L, a modified, low-dose protocol induced 2 week-SU to 0.2 g in 71% (vs 0 of 12 controls); and SU to 1.8 g in 33%, with acceptable safety profile | No severe AE. No EAI. Symptoms with 6.5% of home doses. 2 AE-related withdrawals |
| Yanagida et al. 2016 | 6–19 years | 0.1–0.2 g scrambled egg | ||
| High dose egg OIT vs placebo, RCT |
19 active 14 placebo |
5 months; with 5-day build-up | A high-dose, abbreviated protocol with inpatient build-up induced desensitization to 1 under-cooked egg in 89% of active subjects, vs 0 of placebo | During build-up, 2 episodes of anaphylaxis and 2 EAI. No severe AE during maintenance |
| Perez-Rangel et al. 2017 | Mean 10.4 years | 1 undercooked egg (=3.6 g powder)/48 hours | ||
![]()
Table 6
Representative peanut oral immunotherapy clinical trials
![]()
Table 7
Wheat oral immunotherapy clinical trials
![]()
OIT with omalizumab
A major development in improving safety of OIT has been the use of omalizumab (Table 8). Its use as pretreatment and continued administration through build-up offers significant protection from IgE-mediated reactions, allowing for more rapid and safe dose escalation, with less withdrawals due to dose-related AE. However, reactions to previously tolerated doses may occur after cessation of omalizumab.445152
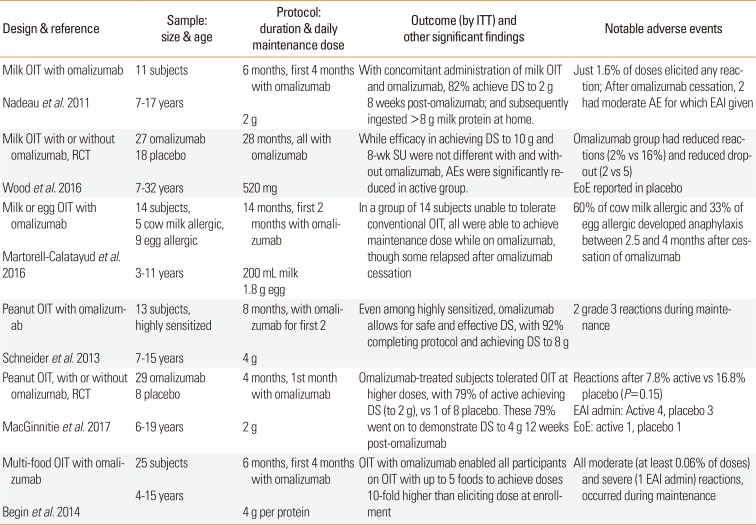
Table 8
Oral immunotherapy with omalizumab
![]()
CM-OIT with omalizumab
In 2011, Nadeau and colleagues44 published results of a 24-week protocol with 9 weeks of omalizumab pretreatment and 16 weeks of CM-OIT with omalizumab, followed by a maintenance phase without omalizumab. In this uncontrolled pilot study, 82% of 11 enrolled subjects reached goal daily maintenance dose, demonstrated desensitization to 7.25 g of milk protein, and subsequently continued home ingestion of >8 g milk protein daily. Though all patients experienced some AE, only 1.6% of doses elicited any reaction, significantly less than 35%–50% observed in some of the first milk OIT trials.4553 However, after cessation of omalizumab during maintenance therapy, 2 of 9 subjects administered EAI for moderate reactions after home doses.
Wood and colleagues54 published results of a 30-month CM-OIT protocol in which participants were randomized to OIT with or without omalizumab until month 28. For omalizumab and placebo groups (respectively), efficacy in achieving desensitization to 10 g CM protein OFC (89% and 71%) and 8 week-SU (48% and 36%) were similar. AEs to CM-OIT were significantly reduced in the group on omalizumab: the median percent of doses with symptoms per subject were 2.1% and 16.1%, and dose-related withdrawals were 0 and 4, respectively.
Peanut-OIT with omalizumab
Schneider and colleagues recruited highly sensitized peanut allergic subjects for open-label study of peanut-OIT with omalizumab, which was given for 12 weeks preceding OIT and continued through 2 months of OIT build-up.55 Twelve of 13 subjects reached 4 g maintenance, continued with 8 months OIT, and subsequently demonstrated desensitization to 8 g peanut protein (PP) during OFC. The most severe AEs were 2 grade 3 reactions, both of which occurred during maintenance.55 In 2016, MacGinnitie and colleagues47 conducted a study randomizing peanut-OIT subjects to omalizumab or placebo as pretreatment and during build-up phase to daily maintenance dose of 2 g. Though reaction rates were similar for omalizumab and placebo, omalizumab subjects tolerated therapy at higher doses and significantly more omalizumab subjects (79% of 29) tolerated the 4 g PP challenge 12 weeks after omalizumab cessation compared to placebo (1 of 8).
Multifood-OIT with omalizumab
Multifood-OIT addressing up to 5 foods was the subject of an open-label study, in which 25 subjects received omalizumab as pretreatment and during 8 weeks of build-up therapy to attain daily maintenance dose of 4 g food protein. All participants reached doses equivalent to a 10-fold increase in allergen tolerance by 2 months of therapy, and mean time to maintenance was just 4.5 months. Regarding safety, initial dose escalation and build-up phases were limited to mild reactions; the most severe reactions occurred during maintenance, with 0.06% of doses causing moderate chest symptoms and 0.02% moderate abdominal symptoms. One severe reaction after a home maintenance dose was treated with EAI.52
Recurrence of symptoms after cessation of omalizumab
Significant adverse reactions have been reported with continued OIT in the weeks following omalizumab cessation: Nadeau and colleagues44 reported 2 moderate AE (treated with EAI) among 11 subjects; Schneider and colleagues55 reported 2 grade 3 reactions among 13 subjects. In Begin et al.'s study with 25 subjects, all moderate reactions (with 0.06% of doses) and one severe reaction (treated with EAI) occurred during maintenance after omalizumab cessation.52
OIT with other immunomodulatory agents
OIT with probiotic
An Australian study has evaluated peanut-OIT combined with probiotic (PPOIT). Tang and colleagues56 reported that 31 PPOIT subjects, who were treated with active OIT and Lactobacillus rhamnosus CGMCC 1.3724 (NCC4007; Nestlé Health Science, Konolfingen, Switzerland) at a fixed dose of 2×1010 colony-forming units (freeze-dried powder) once daily for 18 months, had higher rates of desensitization (90% vs. 7%) and 2-5 week-SU (82% vs. 4%) compared to 28 placebo (placebo PPOIT and placebo probiotic) subjects. Regarding safety on home dosing, the PPOIT group had 6 severe AE with 3 EAI administrations compared to 4 severe AE with 2 EAI administrations on placebo. A follow-up study published in 2017 found that after a mean of 4.2 years from cessation of PPIOT, 67% of 24 PPOIT subjects were consuming peanut on a regular basis; and 58% of 12 PPOIT subjects demonstrated 8-week SU, compared to 1 of 12 placebo.43 The impact of this RCT is significantly limited by the lack of a proper control for the effect of peanut-OIT alone as well as the lack of blinding and no DBPCFC to confirm peanut allergy at baseline.
OIT with Chinese herbs
FAHF-2 is a 9-herb formula based on traditional Chinese medicine that blocks peanut-induced anaphylaxis in a murine model. In phase I studies, FAHF-2 was found to be safe and well tolerated; there was laboratory evidence of immunomodulation without appreciable clinical benefit. No significant differences in allergen-specific IgE and IgG4 levels, cytokine production by peripheral blood mononuclear cells (PBMCs), or basophil activation between the active and placebo groups were detected. In vitro studies reported that subjects' baseline PBMCs incubated with FAHF-2 and food allergen produced significantly less IL-5, greater IL-10 levels, and increased numbers of Treg than untreated cells.57 A clinical trial is underway evaluating combination of FAHF-2, multi-food-OIT, and omalizumab (NCT 02879006).
Go to :
SECTION 5: SLIT TRIALS
Overview of SLIT trials
SLIT trials have evaluated utility in treatment of hazelnut, peanut, and CM allergy (Table 9).13315859 SLIT significantly increases threshold for reactivity in subjects who comply with therapy, though with reduced efficacy compared to OIT.2426 AE, which are typically mild and limited to oropharyngeal pruritus, are common in SLIT. Moderate and severe AE occur with less frequency in SLIT compared to OIT.13 Cofactors, as described with OIT, appear to lower threshold for reactivity to SLIT.58 Occurrence of EoE in association with aeroallergen SLIT6061 suggests a theoretic risk for EoE with food SLIT.
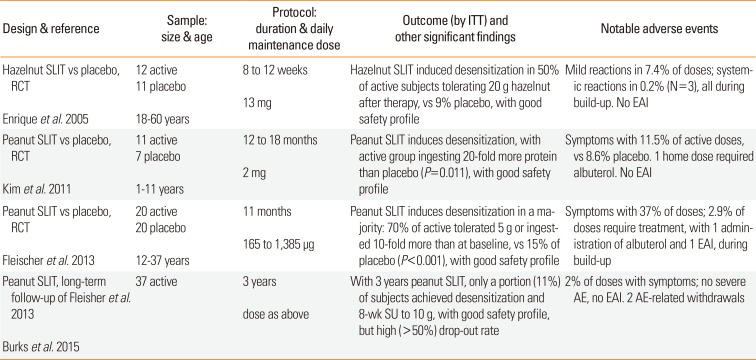
Table 9
Clinical trials of sublingual immunotherapy
![]()
SLIT trials
Hazelnut-SLIT
The first SLIT trial published in 2005 reported desensitization to 20 g hazelnut (approximately 14 hazelnuts) in 50% of 12 SLIT subjects compared to 9% of 11 placebo subjects, after 8–12 weeks of therapy. Mean eliciting dose increased significantly from 2.3 to 11.6 g in SLIT subjects (P=0.02). Regarding safety, there were 3 systemic reactions, all of which occurred during build-up and responded to antihistamine. Mild reactions accompanied 7.4% of doses.58
Peanut-SLIT
Using a 12–18 month peanut-SLIT protocol enrolling subjects aged 12–37 years, Kim and colleagues13 reported that 11 active younger SLIT subjects (1–11 years) consumed 20 times more peanut than 7 subjects randomized to placebo. Compliance was similar on SLIT and placebo. Symptoms accompanied 11.5% of active and 8.6% of placebo doses; 0.26% of home SLIT doses were treated with antihistamine, 1 with albuterol; none with EAI. Using a 44-week SLIT protocol among older SLIT subjects (12–37 years), Fleischer and colleagues59 reported that 70% of 20 SLIT subjects were considered responders (ingested 5 g PP or 10-fold more than baseline), compared to 15% of 20 on placebo (P<0.001). Symptoms accompanied 37% of doses; 2.9% required treatment, with 1 administration of albuterol and 1 of EAI (during build-up). In open-label follow-up study of the same subjects, 11% of 37 subjects continuing with SLIT were desensitized to 10 g PP, with all 4 subsequently demonstrating 8-week SU. There were no EAI administrations. Twenty-five withdrew for various reasons, including 2 for dose-related AE.31
SLIT vs OIT trials
Trials compareing SLIT and OIT are presented in Table 10.
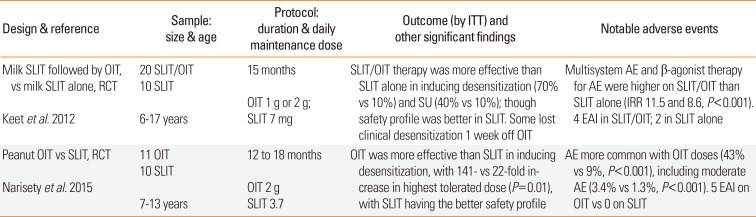
Table 10
Clinical trials comparing oral and sublingual immunotherapy
![]()
Peanut-SLIT vs OIT
Peanut-OIT subjects experienced a 141-fold mean increase in the highest tolerated dose compared to a 22-fold mean increase among SLIT-subjects after 1 year of therapy. One-month SU was achieved by 3 of 10 OIT-subjects compared to 1 of 10 SLIT. SLIT-subjects experienced less severe AE, with 5 EAI administrations related to OIT vs none with SLIT.26
CM-SLIT vs OIT
In a study comparing CM-SLIT alone to therapy with SLIT for initial up-dosing followed by CM-OIT, SLIT/OIT subjects were significantly more likely to demonstrate desensitization (70% of 20) and 6-week SU (40% of 20) compared to subjects receiving SLIT alone (1 of 10). Multisystem reactions and medical intervention (antihistamine, albuterol, and EAI) were more frequent with OIT.24
Go to :
SECTION 6: EPIT TRIALS
Overview of EPIT
Peanut and CM-EPIT have been shown to increase threshold for reactivity in 3 published trials.6 Though efficacy is more modest compared to OIT and SLIT, EPIT appears to have a more favorable side effect profile. Most AEs are limited to local cutaneous symptoms at the patch application site; occasional systemic reactions have been non-severe and resolved with antihistamine. With reduced AE and fewer visits at a medical facility for up-dosing, adherence might be better with EPIT compared to OIT and SLIT.
EPIT trials
EPIT clinical trials are summarized in Table 11. The randomized, double-blind, placebo-controlled phase 1b trial of peanut-EPIT conducted in 5 centers in the US included 100 subjects, aged 6–50 years, randomized 4:1 (peanut/placebo) to receive Viaskin Peanut (VP) treatment in dosing cohorts at doses of 20, 100, 250, and 500 µg or placebo. This trial reported an overall acceptable safety and tolerability after 2 weeks of therapy. There were no severe AE and no EAI administrations; 2 systemic reactions were thought to be related to protein transfer to mucosal surface. Three of 49 active subjects withdrew due to treatment-related symptoms.7
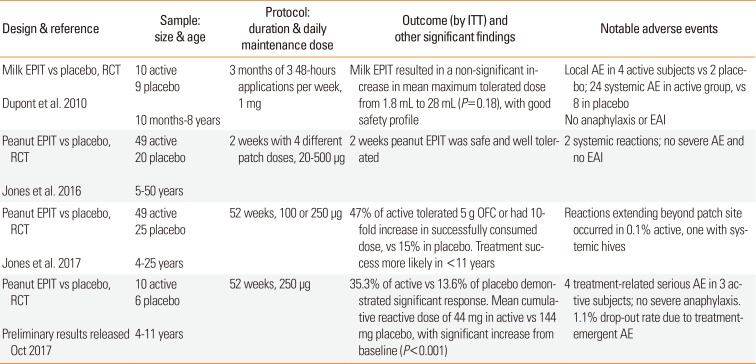
Table 11
Clinical trials of epicutaneous immunotherapy
![]()
In the multicenter-RCT conducted by the Consortium for Food Allergy Research, 74 peanut allergic individuals (ages 4–25 years) were treated with placebo (n=25), VP 100 µg (n=24) or VP 250 µg (n=25), for 52 weeks. The primary outcome was defined as passing a 5,044-mg PP DBPCFC or achieving at least 10-fold increase in successfully consumed dose from baseline. Treatment success was seen in 3 (12%) placebo-treated participants, 11 (46%) VP100-participants, and 12 (48%) VP250-participants (P=0.005 and P=0.003, respectively, compared with placebo; VP100 vs VP250, P=0.48). Median changes in successfully consumed doses were 0, 43, and 130 mg PP in the placebo, VP100-, and VP250-groups, respectively (placebo vs VP100, P=0.014; placebo vs VP250, P=0.003). Treatment success was higher among younger children (P=0.03; age 4–11 vs >11 years). Regarding AE, 80% of EPIT doses had local reactions vs 14.4% placebo. Non-patch site reactions were reported at similar frequency in EPIT and placebo-groups (0.1% and 0.2%, respectively); no EAI or albuterol was required. There were 3 withdrawals from each group, one for treatment-related symptoms in the EPIT group.6
In October 2017, preliminary results of Peanut EPIT Efficacy and Safety (PEPITES) phase III trial evaluating the safety and efficacy of VP in children 4-11 years of age were released (https://globenewswire.com/news-release/2017/10/20/1151107/0/en/DBV-Technologies-Announces-Topline-Results-of-Phase-III-Clinical-Trial-in-Peanut-Allergic-Patients-Four-to-11-Years-of-Age.html). PEPITES reported a statistically significant response, with 35.3% of patients responding to VP 250 µg after 12-months, compared to 13.6% of placebo-patients (difference in response rates=21.7%; P<0.001; 95% confidence interval [CI], 12.4%–29.8%). The primary endpoint, defined as the 95% CI in the difference in response rates between the active and placebo arms, did not reach the 15% lower bound of the CI that was proposed in the study's Statistical Analysis Plan (SAP).
Regarding the Cumulative Reactive Dose (CRD), a key secondary endpoint measuring threshold reactivity during DBPCFC at month-12, patients treated with VP 250 µg and placebo reached a median CRD 444 mg and 144 mg PP, respectively. Median CRD at baseline was 144 mg in both groups. This increase from baseline was statistically significant compared to placebo (P<0.001). PEPITES reported 12 serious adverse events (SAEs) in 10 active-subjects (4.2%), and 6 SAEs in 6 placebo-subjects (5.1%); 4 SAEs in 3 active-subjects (1.3%) were possibly related to treatment; no SAE qualified as severe anaphylaxis. The most commonly reported AEs were mild-moderate patch application site reactions. The discontinuation rate was 10.1%, comparable between the active- and placebo-arms, with a 1.1% dropout rate due to treatment emergent AEs. Mean patient adherence exceeded 95%.
Go to :
SECTION 7: CLINICAL TRIALS OF ADDITIONAL FORMS OF AIT
Other forms of AIT include SCIT with alum-adsorbed hypoallergen and LAMP-DNA vaccine, both of which are being actively investigated in human subjects. A phase IIb clinical trial evaluating safety and efficacy of SCIT with alum-adsorbed, recombinant fish allergen parvalbumin (NCT02382718) is completed but not as yet published. Preliminary results of a phase I clinical trial evaluating safety and immunomodulation with alum-adsorbed chemically modified peanut extract (NCT02851277)38 have been presented in an abstract form. Subjects were randomized to receive 15–20 incrementally increasing weekly doses of study product (HAL-MPE, n=17) or placebo (n=6). Local and systemic reactions were observed more often in the active group; no late (>4 hours after therapy) systemic reactions were observed. Authors concluded that the therapy was safe and well tolerated.38
Two additional forms of AIT, including SCIT with native peanut allergen and rectally-administered modified PP, were previously studied in humans and abandoned due to unacceptable safety profile.626364
Go to :
SECTION 8: AIT IN CLINICAL PRACTICE
AIT in today's clinical practice
Currently available AIT
Of various modalities of AIT, OIT is the only therapy currently accessible to physicians and patients, as food may be delivered in native form and may be purchased and/or prepared at home. While some physicians have begun offering OIT to families who are eager for therapy, OIT in the clinical setting continues to carry risks observed in research studies: in a retrospective chart review of 352 patients undergoing peanut-OIT in clinical practice, patients did experience 95 severe reactions requiring epinephrine.65
Current recommendations for OIT in clinical practice
Experts have yet to recommend that OIT be part of routine clinical practice, due to safety concerns and uncertainty regarding duration of tolerance, even following prolonged therapy. One exception to this is regular ingestion of baked goods among milk- and egg-allergic children, which appears to safely hasten tolerance acquisition to unheated milk and egg.6667 OIT with native food proteins remains a risky endeavor; and protocols for subject selection and administration of OIT in clinical practice are lacking.
Subject-selection for OIT
When guidelines for OIT in clinical practice become available, selecting appropriate subjects for therapy will be as important as protocol design. There are currently no strict criteria to assist practitioners in choosing subjects for OIT. Patients who are highly sensitized or at high risk for severe anaphylaxis may not be appropriate candidates for OIT. Lower threshold dose at entry challenge, higher sIgE, increased sIgE: total IgE ratio, larger SPT wheal diameter, and personal history of asthma or allergic rhinitis were associated with worse outcomes, as measured by frequency of severe AE, adherence to treatment, and demonstration of desensitization and SU.126869 Virtually every OIT trial excludes subjects with history of severe anaphylaxis, uncontrolled asthma, or other chronic conditions and medications which may put subjects at higher risk for more severe reactions; OIT has thus not been studied in and would not be appropriate for patients with these characteristics.
Most food-allergic patients may be of milder phenotype than those included in OIT trials: while entry OFC for clinical trials requires reactivity at doses <100–300 mg, most reactions (55%) during OFC in practice occur at doses >250 mg.70 Therefore, OFC outcomes among the majority of food-allergic subjects will be better than reported in clinical trials.
Factors unrelated to reactivity will also be important in providing safe and effective OIT. Risks of OIT may be unacceptable among patients and families who express hesitance in administering epinephrine, or who do not understand the importance of dose adjustments for and avoidance of cofactors, which lower threshold for reactivity. Compliance with therapy is likely to be hampered by anxiety surrounding dose administration, taste aversions, and insufficient resources to ensure daily dose administration and regular follow-up.
Discussion of OIT should take place in the context of a growing body of evidence on OIT as well as changing landscape of AIT for FA. With SLIT and EPIT likely to become available in the next few years, it may be that waiting for a safer option is a better strategy. Alternatively, it may become clear that immunotherapies are more effective and/or safer in younger children, and should be started sooner rather than waiting for another therapy to become available. Evidence on the safe and effective use of OIT will continue to accumulate in the coming years, with guidelines from experts likely to follow.
Selecting among AIT options in clinical practice in the future
OIT, SLIT, and EPIT for major food allergens are likely to be part of FA-management in the coming years. Depending on outcomes of other clinical trials for LAMP-DNA peanut vaccines and SCIT with hypoallergens, these too may be options. With availability of multiple options, sufficient understanding of AIT will be necessary to evaluate appropriateness of therapy for individual patients. Clinicians will need to engage patients and families in a discussion of realistic outcomes and adverse effects. This discussion will not only be guided by clinical history and allergy testing, but also by assessment of the patient's and family's goals and ability to adhere to protocols.
Combination therapy may prove to be a helpful strategy if and when multiple therapies are available. As has already been done in some clinical trials, a subject may initiate therapy with SLIT, and then transition to OIT. Sufficient desensitization with a few years of EPIT might make more effective therapies such as OIT a safer option in the future. Immunomodulatory therapies such as omalizumab, dupilumab, probiotic bacteria, and/or Chinese herbs may be combined with AIT to improve safety and efficacy.
Go to :
SECTION 9: FUTURE DIRECTIONS
There is a race to develop commercial treatment for FA fueled by increasing prevalence and severity of food allergies in children, particularly peanut allergy. The multi-center phase III clinical trials of peanut-OIT and EPIT are ongoing. Approved, standardized protocols for food immunotherapy that can be safely and effectively implemented in clinical practice are needed. We also need to establish the minimum effective and safe maintenance dose, duration of AIT, and frequency of maintenance dosing for long-term therapy. Considering that at least 30% of those with persistent FA are allergic to multiple foods, treatments for milk, egg, wheat, tree nuts, seeds, fish, and shellfish allergy, as well as approaches for combining multiple foods, are desirable. Approaches to mitigating side effects of AIT, as well as mechanisms to enhance efficacy and development of permanent oral tolerance such as adjuvants, nanoparticles, DNA vaccines, or combined therapies, need to be explored. Biomarkers predictive of the favorable response to AIT are highly desirable. Patients with the most severe phenotype of life-threatening anaphylaxis are currently excluded from clinical trials, yet they are in the dire need of effective treatment that can be adhered to long-term as it is obvious that such patients will need most likely a life-long therapy. Tremendous progress has occurred in the past decade but the permanent cure for FA remains elusive and further research into tolerance development is necessary.
Go to :
CONCLUSION
Emergence of FA as a global health problem underscores the importance of research to develop effective treatment strategies. A growing body of evidence supports the concept of AIT for subsets of food-allergic patients. Currently studied therapies have significant efficacy limitations and associated adverse effects, and do not offer reassurance regarding long-term protection following discontinuation of treatment. The equipoise between AIT vs food avoidance is reflected by the lack of official guidelines from the allergy societies and regulatory agencies and lack of standardized products. Hopefully within the next few years, clinicians will gain a better understanding of the utility of AIT, discover biomarkers predictive of favorable outcomes and develop strategies to enhance safety and efficacy of AIT.
Go to :
 XML Download
XML Download