

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anaphylaxis is a serious, life-threatening generalized or systemic hypersensitivity reaction.123 Most anaphylaxis symptoms present acutely and worsen in a short period of time. For this reason, most anaphylactic patients report to the emergency department. Therefore, it is important for the medical staff of emergency department who first face anaphylactic patients to make an accurate diagnosis and provide an immediate and appropriate treatment. The incidence of anaphylaxis has been continuously rising worldwide over the past 20 years.45 The prevalence of anaphylaxis in the general population is at least 1.6% higher in the United States6 and ranged from 1.5 to 7.9 per 100,000 person-years in Europe.7 There has been active research on anaphylaxis, but many study subjects are limited to patients registered with anaphylaxis codes. As a result, patients not registered with anaphylaxis codes are excluded as study subjects.8 To accurately determine the rate of anaphylaxis, it is necessary to evaluate whether the symptoms and signs of patients meet the diagnostic criteria of anaphylaxis and to accurately register an anaphylaxis code. However, anaphylaxis codes tend to be underused,910 and are highly likely to be registered under anaphylaxis-associated codes, allergy-related disease codes, and symptom codes related to the symptoms and signs of anaphylaxis rather than under directly specified anaphylaxis codes. Therefore, if a large number of anaphylactic patients are registered under other codes and therefore excluded, accurate research on anaphylaxis incidence, etiology, and clinical characteristics may be affected.
To our knowledge, no previous report has assessed the incidence of anaphylactic patients registered under other codes than anaphylaxis. Therefore, this study determined the frequency and clinical characteristics of anaphylactic patients who met diagnostic criteria but were not registered under anaphylaxis codes in the emergency department by comparing them with those of patients who were accurately diagnosed with anaphylaxis.
Go to : 
MATERIALS AND METHODS
Study population
The subjects of this study included adult patients with anaphylaxis aged over 16 years who had presented to the emergency department of a tertiary hospital for 5 years between January 2012 and December 2016. Anaphylactic patients were defined based on a review of anaphylaxis frequency and characteristics and allergy-related codes.1112 To identify the omitted anaphylactic patients, disease codes related to symptoms and signs suggested in the clinical diagnostic criteria of anaphylaxis were also collected (Table 1).13 During the survey period, all medical records of the adult patients who were registered under the disease codes were reviewed retrospectively in order to re-evaluate whether they were actually diagnosed with anaphylaxis. Subjects were excluded if they did not meet the diagnostic criteria of anaphylaxis (as defined by the 2011 World Allergy Organization Guidelines for the Assessment and Management of Anaphylaxis) after reviewing all medical records for anaphylaxis, allergy-related, and symptom-related codes. The study subjects were divided into the accurate group which was registered under T78.0, T78.2, T78.2B, T78.2C, T80.5, and T88.6 codes with the direct specification of anaphylaxis and into the inaccurate coding group which was registered under allergy-related codes and symptom and sign related codes.
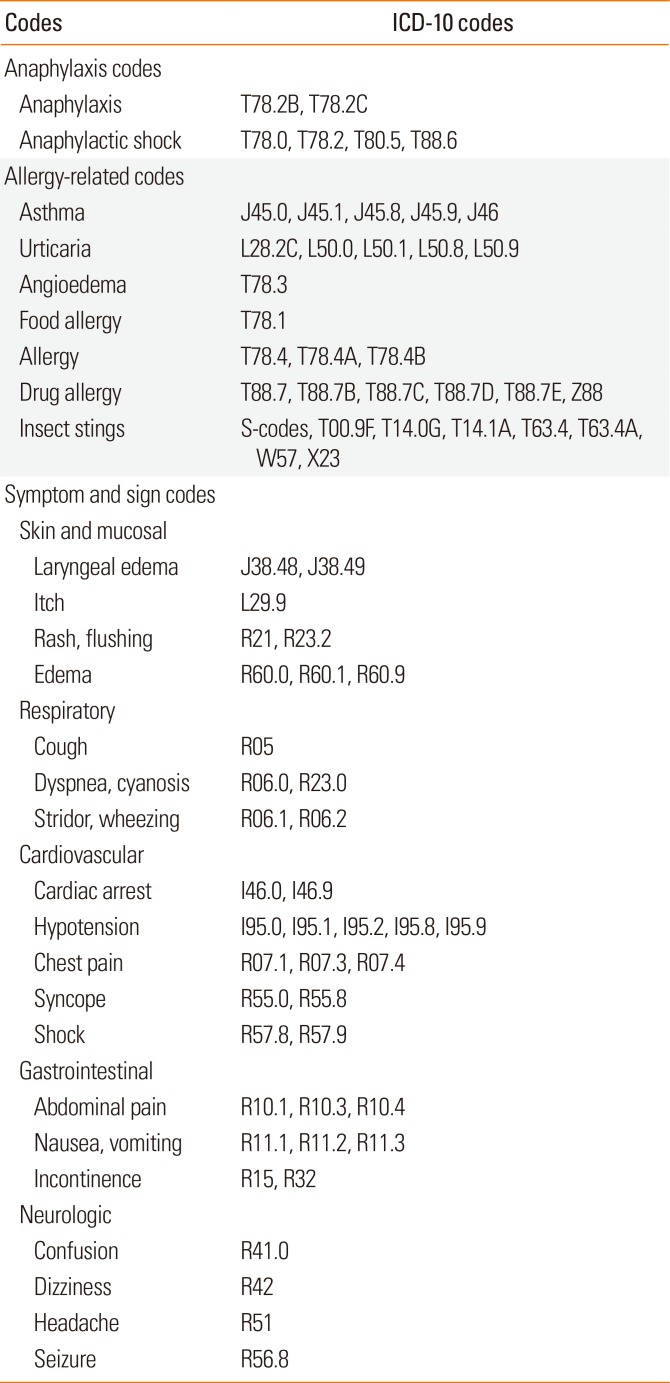
Table 1
International Statistical Classification of Diseases 10th Revision (ICD-10) codes associated with anaphylaxis
![]()
As the diagnostic criteria of anaphylaxis, the clinical criteria for diagnosing anaphylaxis suggested by 2011 World Allergy Organization Guidelines for the Assessment and Management of Anaphylaxis was applied.13
Anaphylaxis is highly likely when any one of the following 3 criteria is fulfilled.
1) Acute onset of an illness with involvement of the skin, mucosal tissue, or both and at least one of the following:
2) Two or more of the following that occur rapidly after exposure to a likely allergen for that patient
Involvement of the skin-mucosal tissue (e.g., generalized urticarial, itch-flush, swollen lips-tongue-uvula)
Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, hypoxemia)
Reduced blood pressure or associated symptoms (e.g., hypotonia [collapse], syncope, incontinence)
Persistent gastrointestinal symptoms (e.g., crampy abdominal pain, vomiting) or
3) Reduced blood pressure after exposure to known allergen for that patient
Data collection
Relevant materials were surveyed to evaluate the patients' general characteristics, causes of anaphylaxis, clinical characteristics, and treatments. We also collected demographic data including patient age, gender, transportation to the emergency department, elapsed time from exposure to symptom onset, elapsed time from symptom onset to emergency department arrival, history of allergic diseases, comorbidities, smoking status, and drinking status. Transportation to the emergency department was classified into public ambulance, transfer from another medical facility, and individual transportation. History of allergic diseases was classified into anaphylaxis, asthma, rhinitis, atopy, drugs, and foods. The causes of anaphylaxis were classified into drugs, radiocontrast media, insect stings, food, exercise, and idiopathic factors. For more detailed causes, drugs were categorized into nonsteroidal anti-inflammatory drugs, penicillin, cephalosporin, vaccines, and acetaminophen; insect stings were categorized into bee, ant, and other insects. Foods were classified into seafood, wheat, buckwheat, nuts, egg, and pork. Aside from those, exercise-induced causes, food-dependent exercise-induced causes, and idiopathic causes were also investigated. Regarding clinical manifestations, the patient symptoms were classified into skin and mucosal, respiratory, cardiovascular, gastrointestinal, and neurologic symptoms. In addition, the severity of hypersensitivity reactions, blood pressure at the time of emergency department arrival, and consciousness were surveyed. On the basis of the method reported by Brown,14 the severity of the hypersensitivity reactions was classified into severe and non-severe grades depending on hypoxia (SpO2 ≤92%), hypotension (systolic blood pressure <90 mmHg), and neurologic symptoms. Regarding prehospital treatment, the oxygen supply, fluid administration, and epinephrine administration were investigated. With regard to treatment in the emergency department, the oxygen supply, endotracheal intubation, fluid administration, steroid administration, epinephrine administration, bronchodilator administration, and cardiopulmonary resuscitation were investigated.
Statistical analysis
Frequency analyses of the registered codes were conducted in both the accurate and inaccurate coding groups. To compare the patients' general characteristics, causes of anaphylaxis, clinical manifestations, and treatments between the 2 groups, univariate comparison analysis was performed using χ2 test, Fisher's exact test, and Mann-Whitney U test. To identify the factors which were highly likely to be registered in the accurate group, those factors that had statistical significance were included in multivariate logistic regression analysis performed after correcting for patient gender. The statistical analyses were performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as a P value less than 0.05.
Ethics statement
This study was exempted for review by the Institutional Review Board due to retrospective study.
Go to :
RESULTS
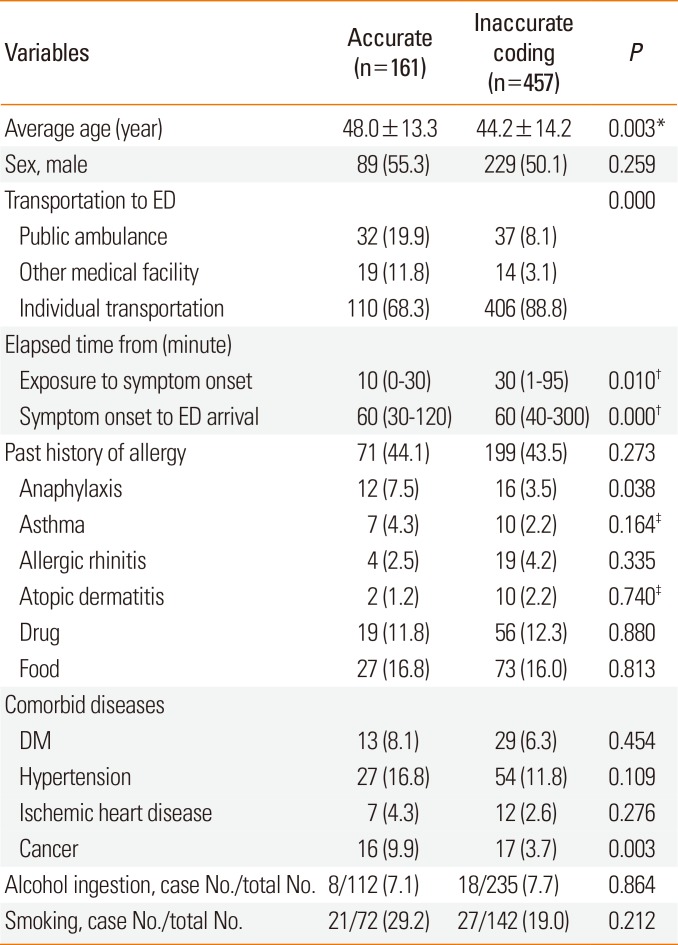
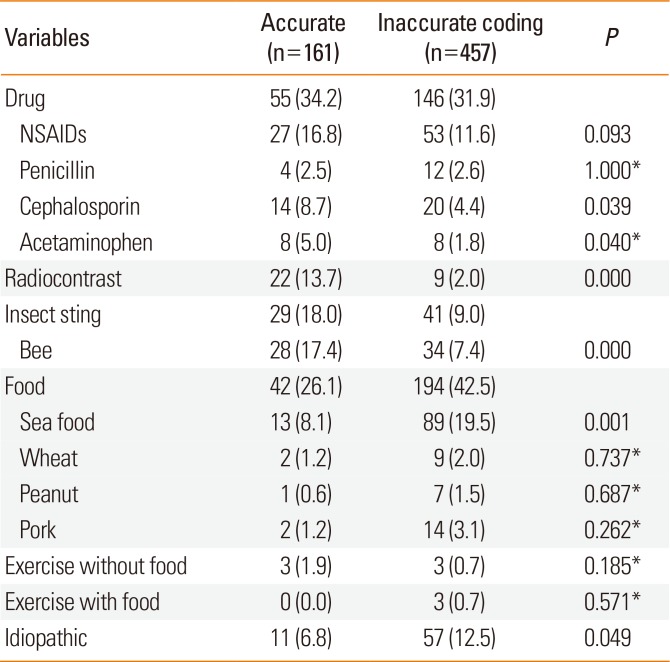
During the 5-year study period, of 211,486 total adult patients who presented to the emergency department, we reviewed all medical records of 63,826 with International Statistical Classification of Diseases 10th Revision (ICD-10) codes that were associated with anaphylaxis, including anaphylaxis, allergy-related, and symptom-related codes. After excluding cases that did not meet the diagnostic criteria of anaphylaxis in each group, of 618 anaphylaxis patients, 161 (26.1%) and 457 (73.9%) were assigned to the accurate and inaccurate coding groups, respectively; 365 patients had allergy-related codes and 92 had symptom codes (Figure). The average ages were 48.0±13.3 and 44.2±14.2 years in the accurate and inaccurate coding groups, respectively. The 2 groups had no difference in gender. Regarding transportation to the emergency department, 68.3% of the accurate group and 88.8% of the inaccurate coding group had individual transportation. The inaccurate coding group had longer elapsed times from exposure to symptom onset and from symptom onset to emergency department arrival. With regard to past history of allergy, 7.5% of the accurate and 3.5% of the inaccurate coding groups had anaphylaxis history. Regarding comorbid diseases, 9.9% of the accurate and 3.7% of the inaccurate coding group had cancer history. The 2 groups had no differences in smoking history and alcohol consumption at the time of symptom onset (Table 2). Drugs were the cause of anaphylaxis, in 47.8% and 33.9% of the accurate and inaccurate coding groups, respectively. Analysis of the detailed causes revealed the differences between the 2 groups in cephalosporin (8.7% vs 4.4%), acetaminophen (5.0% vs 1.8%), and radiocontrast media (13.7% vs 2.0%). Insect stings accounted for 18.0% of the accurate group and 9.0% of the inaccurate coding group. Foods accounted for 26.1% and 42.5% of the accurate and inaccurate coding groups, respectively. The 2 groups had no difference in exercise. Idiopathic cases accounted for 6.8% of the accurate group and 12.5% of the inaccurate coding group (Table 3).
 | FigureThe numbers of accurately and inaccurately registered anaphylaxis patients. We excluded patients (a) without ICD-10 codes that are associated with anaphylaxis (anaphylaxis, anaphylaxis-related, and symptom-related codes). We further excluded (b) patients with allergy- and symptom-related codes who did not satisfy the diagnostic criteria of anaphylaxis patients among those with ICD-10 codes associated with anaphylaxis.
|
Table 2
General characteristics of accurate and inaccurate anaphylaxis registration
![]()
Table 3
Causes of accurate and inaccurate anaphylaxis registration
![]()
Among anaphylaxis symptoms, the accurate group had more cardiovascular (77.0% vs 34.8%) and neurologic (29.8% vs 9.8%) symptoms than the inaccurate coding group, whereas the inaccurate coding group had more cutaneous symptoms (92.3%) than the accurate group (74.5%). Severe symptoms occurred in 57.1% of the accurate group and 9.8% of the inaccurate coding group. Non-alert consciousness was present in 14.3% and 0.9% of the patients in the accurate and inaccurate coding groups, respectively. Regarding prehospital treatment, the accurate group more often had oxygen supply (4.3% vs 1.1%) and epinephrine use compared to the inaccurate coding group (2.5% and 0%). Regarding emergency department treatment, the accurate group had more oxygen supply (34.8% vs 9.8%), endotracheal intubation (4.3% vs 0%), and epinephrine use (57.8% vs 14.7%) than the inaccurate coding group. Fluid administration, steroid use, and bronchodilator use did not differ between the 2 groups (Table 4).
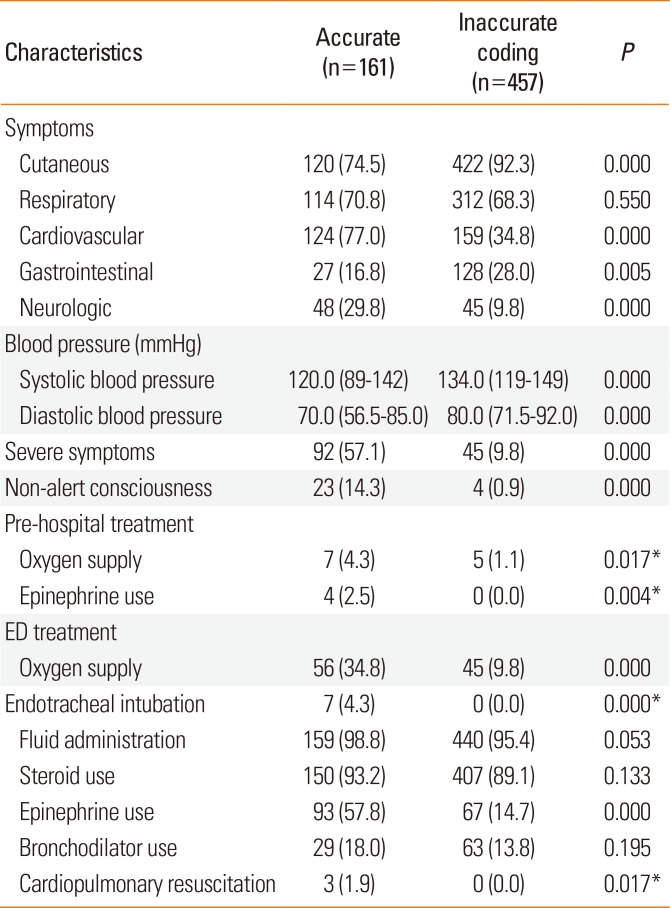
Table 4
Clinical characteristics of accurate and inaccurate anaphylaxis registration
![]()
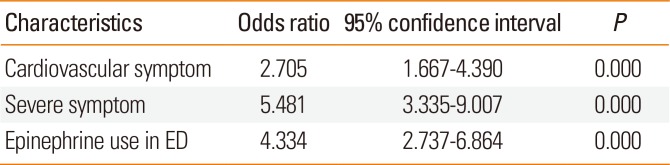
The factors with statistical significance in univariate comparison analysis were included in the multivariate logistic regression analysis after adjusting for gender. The results indicated that anaphylactic patients with cardiovascular symptoms, severe symptoms, and epinephrine use in the emergency department were likely to be registered with anaphylaxis codes (Table 5).
Go to :
DISCUSSION
Anaphylaxis is a hypersensitivity reaction, ranging from urticaria to fatal systemic cardiovascular compromise. Its symptoms and signs vary and its causal relation with allergens is not clear. For this reason, relevant patients may be registered using other codes related to the symptoms and signs rather than anaphylaxis codes. Although anaphylaxis patients are registered under urticaria or angioedema symptom-related codes rather than anaphylaxis codes, any appropriate patient treatment is not incorrect. Nevertheless, registration of patients under other codes rather than anaphylaxis codes makes it difficult to accurately determine the anaphylaxis incidence. To our knowledge, there is no research on anaphylactic patients registered under other related codes. Therefore, future research on anaphylaxis should also consider inaccurately registered anaphylactic patients, as shown in this study.
In this study of patients who had presented to the emergency department for 5 years, 618 patients met the diagnostic criteria for anaphylaxis; of these, in the inaccurate coding group were registered under other codes than anaphylaxis codes, a number greater than that in the accurate group (161 patients). In the inaccurate coding group, the most common registered code was urticaria (173 patients), followed by angioedema (130 patients) (Figure). This finding indicates that skin features arising in urticaria and angioedema are easily observed with the naked eye. Additionally, compared to objective symptoms, subjective symptoms such as abdominal pain and shortness of breath are unclear or mild; therefore, patients meeting the diagnostic criteria were likely to be registered as having the subjective symptoms or angioedema, which are relatively clearer than anaphylaxis. In particular, if patients had clear skin features but other mild symptoms, they were often registered under urticaria. Patients with clear mucosal edema accompanied by respiratory symptom were often registered under angioedema. In the inaccurate coding group, 92 patients (14.9%) were registered under the codes in which the symptoms and signs are directly specified. The patient group registered under their respiratory symptom was the largest (31 patients), followed by skin and mucosal symptoms (29 patients). This is most likely because the medical staff was unable to accurately understand diagnostic criteria of anaphylaxis and to make a diagnosis; thus, the patients were registered under their chief complaint as a symptom code. Therefore, to accurately survey the anaphylaxis incidence rate, it is necessary to educate the medical staff of emergency departments to accurately understand the anaphylaxis diagnostic criteria.
Previous studies reported the principal triggers of anaphylaxis to include foods, insect stings, and drugs; however, there were differences depending on the study population, study design, and geographic area.4101516171819 In this study, the causes of anaphylaxis in the accurate group included drugs, foods, and insect stings in this order of prevalence, compared to foods, drugs, and idiopathic anaphylaxis in the inaccurate coding group. This result was similar to those of previous studies. In the accurate group, radiocontrast media were significantly large. That was because the administration of radiocontrast media in the course of examination in the emergency department triggered anaphylaxis and consequently there was a clear causal relation. In the inaccurate coding group, idiopathic anaphylaxis was significantly large.
Skin signs are the most characteristic symptoms and signs of anaphylaxis, frequently accompanied by respiratory, gastrointestinal, and cardiovascular symptoms.101620212223 In this study, cardiovascular signs, such as hypotension, were most common in the accurate group, followed by skin signs; in the inaccurate coding group, skin signs were most common, followed by respiratory symptoms. The reason for these differences was that the medical staff recognized patients with severe reactions like hypotension as having anaphylaxis and registered them using an anaphylaxis code; however, patients with relatively mild skin signs or mildly labored respiration were judged to meet the diagnostic criteria of anaphylaxis but were registered under other codes. This supports the finding that the accurate group had significantly higher frequencies of severe symptoms and non-alert consciousness.
Anaphylaxis is a medical emergency and prompt management is of vital importance. Epinephrine is an important drug for the initial management of anaphylaxis. Its delayed administration may lead to patient death.1324 This study also revealed that the accurate group had significantly higher use of oxygen supply and epinephrine administration. In particular, patients who were administered epinephrine were accurately registered with anaphylaxis codes 4.3 times more often than those who were not (Table 5). This difference means that patients who received epinephrine experienced severe reactions, such as hypotension or hypoxia. As described earlier, the medical staff clearly recognized these severe reactions as anaphylaxis and registered the patients with anaphylaxis codes. Medical practitioners in the emergency department tend to focus on patients with severe anaphylaxis who present with specific symptoms and treatment, as shown in this study. However, anaphylaxis can present with a wide range of symptom severity, from mild to fatal. No case of anaphylaxis should be overlooked, as anaphylaxis has a high probability of worsening within a short period. Therefore, it is important to continuously educate the medical staff in the emergency department about the manifestations and management of anaphylaxis. To accurately diagnose patients with mild symptoms and signs as anaphylactic patients, the medical staffs in the emergency department need to understand the diagnostic criteria of anaphylaxis and accurately register anaphylaxis codes. As shown in this study, there are cases where patients who met the diagnostic criteria of anaphylaxis were registered under other codes. Therefore, to identify anaphylactic patients, it is necessary to search for study patients including those registered with anaphylaxis-related codes.
The results of this study cannot be generalized as this was a retrospective study that was conducted at a single university hospital. Further prospective multicenter studies will be needed to overcome this limitation. The study subjects were only those patients who had reported to the hospital emergency department and did not include outpatients or patients who were hospitalized and had anaphylaxis. Given that anaphylaxis occurs acutely, the initial treatment is likely to be provided to the patients in the Emergency Department rather than outpatients, except for those who are hospitalized and have anaphylaxis. To search for anaphylactic patients, this study collected the disease codes used in previous works and symptom codes that satisfied the diagnostic criteria of anaphylaxis. Therefore, it is likely to have excluded anaphylactic patients who were registered with different disease codes. This study focused on the registered disease codes for anaphylactic patients in the emergency department of a single university hospital. The emergency department of a research hospital may have high or low registered disease codes for anaphylaxis, making it difficult to generalize the results of this study. Nevertheless, this study shows the potential for the underestimation of the anaphylaxis frequency and incidence rates reported in previous studies on anaphylaxis.
This study revealed that among adult anaphylactic patients who reported to the emergency department, those registered inaccurately outnumbered those registered accurately and that they were sometimes registered not only under allergy-related codes but also under symptom-related codes. Patients with cardiovascular symptoms, severe symptoms, and epinephrine use in the emergency department were highly likely to be accurately registered with anaphylaxis codes.
Go to :
 XML Download
XML Download