

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the past few decades, highly sensitive and specific tests for virus detection have been developed, resulting in accurate detection of a long list of viruses associated with wheezing in early life, the risk for developing asthma, and exacerbation of established disease. Human rhinovirus (RV) and respiratory syncytial virus (RSV) top the list, but recently discovered or re-emerging viruses (e.g., human metapneumovirus [HMPV] coronaviruses and enterovirus [EV]-D68) also contribute to acute wheezing in infancy and virus-mediated exacerbations. However, most viral infections are not associated with acute exacerations, and cofactors, including allergic inflammation and airway bacteria, have been described that increase the severity of infection and the probability of exacerbation.12 Detection of both viruses and airway bacteria are associated with acute wheezing illnesses; specifically, co-infections of respiratory viruses and Moraxella catarrhalis, Hemophilus influenza, and/or Streptococcus pneumonia increases the risk for more severe respiratory illnesses and exacerbations of asthma.3 The addition of antibiotics to treatment regimens for asthma exacerbation could materialize in the near future.
Several recent studies have also shown that respiratory allergy may partner with certain viral infections to synergistically produce airway inflammation and increase cold and asthma symptoms.4 Since there is currently no safe and effective antiviral for RV, the targeting of allergic inflammation may prove beneficial in reducing risk of severe virus-induced asthma symptoms.5 There are several possible immunopathologic mechanism(s) that connect viral and bacterial infection, allergy, and acute asthma, as discussed in the following sections.
Go to : 
VIRUSES AND ASTHMA EXACERBATION
Asthma exacerbation is defined as an acute or subacute worsening of symptoms and lung function as compared to the patient's usual health status or, occasionally, the initial presentation of asthma.6 Exacerbations often represent essentially an exaggerated lower airway response to an environmental exposure, with airway inflammation being a key component that promotes airflow obstruction and increased airway hyperresponsiveness.7 Early treatment of asthma exacerbation is considered the best strategy for management,8 and increases in eosinophilic inflammatory markers have been shown to be good predictors of asthma exacerbations.9 Utilizing this idea, tailoring patient treatment based on the direct and objective measurement of the eosinophil, a key component of airway inflammation in asthma, has proven more efficacious (e.g., less frequent and severe asthma exacerbations) than treatment based on clinical symptoms and lung function.10
Exacerbations usually occur in response to a variety of external agents (e.g., respiratory pathogens, allergens, air pollutants, smoke, and cold or dry air); however, it is estimated that up to 85% of asthma exacerbations in children11 and a considerable proportion in adults (76%-80%)12 are linked to viral infections. The severity of the situation is compounded by the lack of specific antiviral strategies. Virus-induced asthma exacerbations are most often associated with detection of RV,5 RSV,13 human parainfluenza virus (HPIV),14 human influenza virus (HIFV),15 and human adenovirus (HAdV).16 More recently, human bocavirus (HBoV), HMPV,17 certain strains of human coronavirus (HCoV) (e.g., HCoV-NL63, HCoV-OC43, and HCoV-229E),18 and EV-D6819 have been associated with asthma exacerbation.
Viral identification in early childhood wheeze
Viral identification in early childhood wheezing illness may provide prognostic information regarding short- and long-term consequences. In the short term, RSV-induced bronchiolitis is associated with longer hospitalization than RV-induced bronchiolitis.20 The risk of reinfection with certain viruses varies; for example, there is a strong likelihood of RSV reinfection in the absence of ongoing passive immunity.21 Two studies found this risk to be as high as 74%22 and 76%23 if the initial infection occurred within the first year of life. Fourth, certain respiratory viruses have a well-documented association with subsequent asthma development and then exacerbation. More severe RSV illnesses in early childhood increase the risk of asthma development,24 and the risk for developing asthma is even greater after a RV wheezing episode in early life.25 Some children may have genetic risk factors for wheezing with RV26 or with RSV.
RV
RV is the most prevalent human respiratory virus and is classified into 3 species (A, B, and C), with each of these species comprised of a number of different types: A (80 types), B (32 types), and C (up to 55 types).28 Within each species, there is considerable genetic and antigenic heterogeneity;28 while among species, A and C are phylogenetically closer than B and C. RV-A and RV-B were originally classified according to sensitivity to capsid-binding drugs, and RV-C was classified by sequence-based criteria.29 RV circulates throughout the year but in many geographic areas appears to have distinct peaks of incidence in the fall and spring.30 Infection rates remain substantial for the rest of the year.
In both adults and children, RV is the most frequently identified virus associated with acute asthma exacerbation.31 RV enters the body through the respiratory route and infects and replicates in epithelial cells. It was first thought that RV infected only the upper airway, but it is now known that it can also infect the lower airway.32 One of the proposed reasons why asthmatics are predisposed to viral infection is damaged epithelium, which may increase susceptibility to infection and ultimately lead to airway obstruction. Cellular mechanisms involved in this response include higher intracellular adhesion molecule-1 (ICAM-1) expression on respiratory epithelial cells, disruption of epithelial barrier function, impaired apoptosis, increased cell lysis, deficient Th1 response (e.g., interferon [IFN]-γ), and enhanced neutrophil recruitment.7 RV infection also induces pro-inflammatory mediators, including interleukin (IL)-6, IL-8, tumor necrosis factor-α (TNF-α), IL-β, regulated on activation normal T expressed and secreted (RANTES), and granulocyte-macrophage colony stimulating factor (GM-CSF).33
In addition to increasing airway neutrophils, RV-induced asthma exacerbation can also be associated with increases in airway eosinophils (Eos).2 Airway Eos bind to RV and may participate in virus-specific immune responses through antigen presentation and T cell activation.34 Eos may contribute to antiviral responses to RSV in vitro,35 but the clinical significance of these effects is unclear. Eos can have immunomodulating effects, including inducing T cell activation, and eosinophilic cationic protein (ECP) can upregulate ICAM-1 expression on respiratory epithelial cells.36 It should be noted that 90% of RV-A and RV-B serotypes use ICAM-1 as a receptor, which has a pivotal role in movement of inflammatory cells into the airways.37 RV-C types bind to cadherin-related protein-3 (CDHR3), and the corresponding gene has been linked to childhood asthma associated with severe wheezing episodes in early life.38
RSV
The 2 antigenic/genetic subtypes of RSV (A and B) exhibit seasonality, with RSV-A predominating in the fall/early winter and RSV-B in the winter and early spring.39 RSV-A is associated with more severe illness, while RSV-B has been characterized as the milder strain.40 Knowing which subtype a patient is infected with may, therefore, have some clinical value—such as treatment, prognosis, and even prevention—as more therapeutic and prophylactic modalities become available.39
In addition to causing acute wheezing and bronchiolitis in infants, RSV can also contribute to asthma exacerbations in children and adults.41 RSV infection of the airway induces airway inflammation and can promote airway hyperresponsiveness. Airway epithelial cells initially respond to RSV infection by releasing type I IFNs, IL-12, IL-18,42 and a variety of cytokines and chemokines, including IL-8, IL-10, RANTES, macrophage inflammatory protein (MIP)-1α, monocyte chemotactic protein (MCP)-1, and eotaxin.43 After migration to the lymph nodes for viral antigen presentation to T cells, dendritic cells migrate back to the infected epithelium, release mediators again (e.g., IFN-γ, IL-2, IL-4, IL-5, IL-9, and IL-12), and recruit additional inflam-matory cells (e.g., CD8+ T cells and B cells), and granulocytes (neutrophils and Eos).44
Under some circumstances, RSV infection may promote a T helper 2 (Th2) bias in immune responses in humans41 and animals.42 This was also found in a study comparing differential airway inflammatory responses in RSV- and influenza-induced asthma exacerbations. IFN-γ and TNF-α levels were significantly lower in RSV-induced asthma exacerbation when compared to asthmatics infected with influenza.45 Indeed, the weaker Th1 response during viral infection in these individuals may lead to reduced viral clearance and prolonged and/or more serious disease. RSV infection is a potent inducer of chemokines,46 and RANTES and eotaxin in particular have been associated with increased eosinophilia and RSV disease severity in mice.47 Eotaxin appears to be a key component of Th2-driven disease,48 and eotaxin levels correlate closely with eosinophil degranula-tion (i.e., eosinophil-derived neurotoxin [EDN] and ECP) in pediatric asthma.49 Consequently, it may be a good therapeutic target in asthma and other eosinophil-related disease.
Host factors may be critical in determining RSV-induced disease severity, even when taking age-related effects, current/recent infection, air pollution, and allergen exposure into account.44 Host genetic studies have found several polymorphisms to relate to RSV severity, including those in the chemokine receptor CCR550 (which binds a number of inflammatory CC-chemokines, including MIP-1α, MIP-1β, and RANTES), CXCL8, IL-4, and promoter variants of IL-9, IL-10, and TNF-α.51 Thus, gene-environment interactions may contribute to susceptibility to virus-induced disease.
EV-D68
All EVs, including poliovirus, circulate mostly in the summer and fall in temperate and year-round in tropical climes.52 There are more than 100 nonpolio human EVs, with the newer numbered ones being classified into 4 species, EV-A, EV-B, EV-C, and EV-D. EV-D includes 3 serotypes known to cause disease in humans: EV-D68, EV-D70, and EV-D94.53 Although EV-D68 is not new, having first been isolated in 1962 from a small group of US children with lower respiratory tract infection, it has emerged in the past decade as an important respiratory pathogen, with reports from North America, Europe, and Asia. Its association with severe respiratory disease is of special note in children with asthma.19 Exactly how it is able to cause lower respiratory tract disease is currently unknown because the virus binds specifically to cell receptors found predominantly in the upper respiratory tract;54 however, additional mediators are required for EV-D68 to enter cells.55 There is evidence that recent strains of EV-D68 that are associated with lower respiratory tract infection may have gene mutations that influence antigenicity or trophism for lower airway cells.
Go to :
COFACTORS FOR VIRUS-INDUCED EXACERBATIONS OF ASTHMA
Most asthma exacerbations are associated with viral infection. However, infections with RV and other respiratory viruses are quite common, and most natural (or experimentally induced) infections in asthmatics do not result in exacerbations.12 As discussed above, RV species and host genetics can influence the severity of illness and the probability of wheezing illnesses. Additional factors that influence the severity of viral infection and the risk of developing an asthma exacerbation are allergic sensitization and the airway bacteria (Figure).
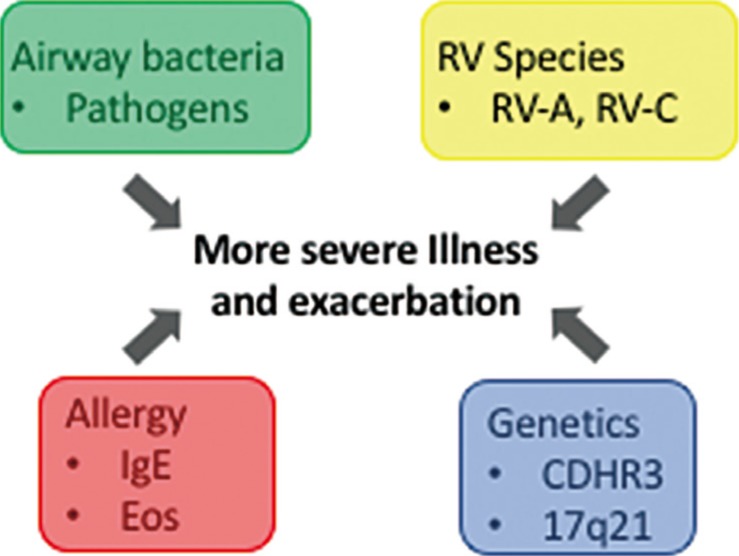 | FigureFactors that can influence the severity of RV infections and the risk of RV-induced exacerbations of asthma. In children and adults with asthma, the severity of RV infection is positively related to the probability of exacerbation. Factors that increase the likelihood of more severe RV illnesses and exacerbations of asthma include the species of RV, the presence of bacterial pathogens in the airway, allergic inflammation, and polymorphisms in CDHR3 and the 17q21 region of the genome. RV, rhinovirus; CDHR3, cadherin-related protein-3; IgE, immunoglobulin E; Eos, eosinophils.
|
Interactions between RV infection and allergy
RV infection and allergic sensitization synergistically increase the risk of wheezing illnesses.56 Atopic asthma can be associated with reduced virus-induced IFN responses, decreased viral clearance57 and increased viral shedding.58 In some studies, atopic asthmatics vs non-atopic controls have reduced peripheral blood mononuclear cell (PBMC) IFN responses.59 Furthermore, some studies have found that bronchial epithelial cells of atopic asthmatics permit increased RV replication, enhanced cell lysis, and deficient release of IFN-β.60 Studies of children with allergic asthma treated with omalizumab indicate that neutralizing immunoglobulin E (IgE)-mediated inflammation can lead to improvements in IFN responses and reduced virus-induced exacerbations.61 This suggests that IgE-mediated inflammation can inhibit antiviral responses and increase the risk for virus-induced exacerbations of asthma.
Virus-bacteria interactions
Several studies have shown that viral infections precede bacterial infections of the upper and lower airways and may affect disease severity (e.g., increased invasive pneumococcal disease during high RV and RSV activity).62 This may occur for several reasons, including virus-induced expression of airway receptors used by bacteria for cell invasion and disruption of airway epithelial layers.63 Viruses and bacteria also increase release of inflammatory cytokines and mediators from epithelial cells and leukocytes, causing increased inflammation with a concomitant increase in symptoms and risk of asthma exacerbation.3
Patients with stable asthma have even exhibited increased colonization of upper and lower airways with Proteobacteria, a group of bacteria predominantly composed of gram-negative species.64 The possible role of bacteria in the early stages of asthma has been demonstrated by Bisgaard et al.65 who found that S. pneumonia, H. influenzae, or M. catarrhalis colonization of the upper airway in early infancy was associated with increased risk of recurrent wheezing leading to asthma. Furthermore, wheezing illnesses in young children are similarly associated with detection of either viral or bacterial pathogens in the airway.66 RV infections can promote increased detection of bacterial pathogens, and the combination of RV infection with detection of respiratory pathogens is associated with a greater risk for illness, including exacerbation of asthma.3 Similarly, acute wheezing illnesses in infants or school-aged children are associated with both viral infections and airway microbiota that are dominated by bacterial pathogens.67
This raises the possibility that selective use of antibiotics or vaccination could be useful in asthma. In wheezing infants, 2 controlled studies have reported that azithromycin produced clinical benefit in infants with acute wheezing.68 Whether this is due to antimicrobial effects or anti-inflammatory effects of the macrolide is uncertain. Given that repeated antibiotic therapy could have adverse effects on commensal bacteria, and could also add to the problem of drug-resistant bacteria, more research is needed on long-term effects of this approach.
Go to :
CONCLUSION
Improved testing methods have helped demonstrate that infections with several respiratory viruses are important contributors to asthma exacerbation and possibly the development of asthma in early childhood. Cofactors, such as genetics, allergic inflammation, and the airway microbiome, also modify the risk of more severe viral illness and exacerbation of established asthma. While practical antiviral strategies are lacking, there may be other opportunities to prevent or treat virus-induced exacerbations by reducing airway inflammation or perhaps targeting microbial cofactors.
Go to :
 XML Download
XML Download