

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Open fractures require infection prevention, injured soft tissue management, and fracture fixation. Moreover, it should be treated according to the emergency surgery. The main goals of treatment are life preservation, limb preservation, infection prevention, and functional restoration. Treatment procedure is carried out in the following order. Early diagnosis and management in the emergency room, appropriate antibiotic treatment, adequate irrigation and thorough debridement, fracture fixation and wound restoration (temporary stabilization of the fracture and covering of the wound, definite fixation of the fracture and soft tissue coverage). Herein, we discuss the current trends in each treatment phase to be helpful to other clinicians regarding the applicability of these steps in clinical practice.
Figures and Tables

 | Figure 2(A, B) A 61-year-old male with a right shaft fracture of the tibia and (C) open wound (Gustillo-Anderson classification type II). (D–F) Planning of pin placement is essential to avoid a compromise of definitive internal fixation. (G) External fixator was used as a reduction tool.
|
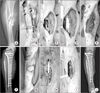 | Figure 3(A) A 42-year-old male with a right shaft fracture of the tibia and open wound (Gustillo-Anderson classification type 3B). (B) External fixator and vacuum-assisted closure was applied. (C) After 5 days of injury, large bone defect was observed when definitive plate fixation was performed. (D) Polymethylmethacrylate was filled in bone defect. (E) Soft tissue defect was reconstructed by gastrocnemius flap. (F) The fibula fracture was fixated at the same time to increase stability. (G) After 6 weeks, the wound was healed without complications. (H, I) Autogenous bone graft was performed using the Masquelet technique. (J) After 7 months, the fracture was united without complications.
|
 | Figure 4(A) A 53-year-old male with a right shaft fracture of the tibia and (B) open wound (Gustillo-Anderson classification type 3B). (C) The fracture was fixated using the minimally invasive plate osteosynthesis technique. (D) At the same time, soft tissue defect was reconstructed by gastrocnemius flap. (E, F) After 1 year, the fracture united and (G) the wound healed without complications. (H) Function of the right limb was normal (images courtesy of CW Oh, M.D.).
|
 | Figure 5(A) A 10-year-old male with a shaft fracture of the right tibia and fibula. (B) The open wound (Gustillo-Anderson classification type 3B) was approximated using a surgi loop. (C) Using surgical gel to prevent skin maceration. (D) The sponge was applied using the OPSITE® (Smith & Nephew). (E) After 6 days, the open wound became smaller. (F) The wound was sutured. (G) The fractures were fixated using a plate at the same time. (H) After 2 weeks, the wound healed without complications.
|
 | Figure 6(A) A 48-year-old male with a right shaft fracture of the tibia and fibula and (B) open wound (Gustillo-Anderson classification type 3B). (C) External fixator was applied and fibula fracture was fixated with a plate. (D) The sponge was applied. (E) After 5 days, the fracture was fixated with intramedullary nail. (F) After 2 months, bone defect was observed. (G) Autogenous iliac bone graft was performed. (H) After 18 months, the fracture was united.
|
 | Figure 7(A) The same patient in Figure 6 with a combined right shaft segmental fracture of the femur and (B) open wound (Gustillo-Anderson classification type 3A). (C) The fracture was fixated with intramedullary nail. (D) After 2 months, the fracture was in union. (E) After 6 months, the fracture was in union. (F) After 18 months, the fracture was united.
|

References
1. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976; 58:453–458.
2. Okike K, Bhattacharyya T. Trends in the management of open fractures. A critical analysis. J Bone Joint Surg Am. 2006; 88:2739–2748.
3. Rivera JC, Wenke JC, Pugh MJ. Open fracture care during war: opportunities for research. JBJS Rev. 2016; 4:01874474-201610000-00003.
4. Morgan BW, Read JR, Solan MC. Photographic wound documentation of open fractures: an update for the digital generation. Emerg Med J. 2007; 24:841–842.

5. Gosselin RA, Roberts I, Gillespie WJ. Antibiotics for preventing infection in open limb fractures. Cochrane Database Syst Rev. 2004; (1):CD003764.
6. Hauser CJ, Adams CA Jr, Eachempati SR. Council of the Surgical Infection Society. Surgical Infection Society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt). 2006; 7:379–405.
7. Ryan SP, Boulton CL, O'Toole RV. Open diaphyseal tibia fractures. In : Sethi MK, Jahangir A, Obremskey WT, editors. Orthopedic traumatology: an evidence-based approach. New York: Springer;2013. p. 303–319.
8. Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma. 2011; 70:751–754.
9. Jaeger M, Maier D, Kern WV, Südkamp NP. Antibiotics in trauma and orthopedic surgery: a primer of evidence-based recommendations. Injury. 2006; 37:Suppl 2. S74–S80.
10. Murray CK, Obremskey WT, Hsu JR, et al. Prevention of infections associated with combat-related extremity injuries. J Trauma. 2011; 71:S235–S257.
11. Ostermann PA, Seligson D, Henry SL. Local antibiotic therapy for severe open fractures. A review of 1085 consecutive cases. J Bone Joint Surg Br. 1995; 77:93–97.
12. Zalavras CG. Prevention of infection in open fractures. Infect Dis Clin North Am. 2017; 31:339–352.
13. Haury B, Rodeheaver G, Vensko J, Edgerton MT, Edlich RF. Debridement: an essential component of traumatic wound care. Am J Surg. 1978; 135:238–242.
14. Pollak AN, Jones AL, Castillo RC, Bosse MJ, MacKenzie EJ. LEAP Study Group. The relationship between time to surgical debridement and incidence of infection after open high-energy lower extremity trauma. J Bone Joint Surg Am. 2010; 92:7–15.
15. Schenker ML, Yannascoli S, Baldwin KD, Ahn J, Mehta S. Does timing to operative debridement affect infectious complications in open long-bone fractures? A systematic review. J Bone Joint Surg Am. 2012; 94:1057–1064.
16. Namdari S, Baldwin KD, Matuszewski P, Esterhai JL, Mehta S. Delay in surgical débridement of open tibia fractures: an analysis of national practice trends. J Orthop Trauma. 2011; 25:140–144.
17. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhai JL, Mehta S. Open tibial shaft fractures-- I. Evaluation and initial wound management. J Am Acad Orthop Surg. 2010; 18:10–19.
18. Sambandam SN, Gul A. Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds. J Bone Joint Surg Am. 2005; 87:2588. author reply 2588-9.
19. FLOW Investigators. Bhandari M, Jeray KJ, et al. A trial of wound irrigation in the initial management of open fracture wounds. N Engl J Med. 2015; 373:2629–2641.
20. Roberts CS, Pape HC, Jones AL, Malkani AL, Rodriguez JL, Giannoudis PV. Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect. 2005; 54:447–462.
21. Antich-Adrover P, Martí-Garin D, Murias-Alvarez J, Puente-Alonso C. External fixation and secondary intramedullary nailing of open tibial fractures. A randomised, prospective trial. J Bone Joint Surg Br. 1997; 79:433–437.
22. Bhandari M, Zlowodzki M, Tornetta P 3rd, Schmidt A, Templeman DC. Intramedullary nailing following external fixation in femoral and tibial shaft fractures. J Orthop Trauma. 2005; 19:140–144.
23. Masquelet AC, Fitoussi F, Begue T, Muller G. Reconstruction of the long bones by the induced membrane and spongy autograft. Ann Chir Plast Esthet. 2000; 45:346–353.
24. Apard T, Bigorre N, Cronier P, Duteille F, Bizot P, Massin P. Two-stage reconstruction of post-traumatic segmental tibia bone loss with nailing. Orthop Traumatol Surg Res. 2010; 96:549–553.
25. Flamans B, Pauchot J, Petite H, et al. Use of the induced membrane technique for the treatment of bone defects in the hand or wrist, in emergency. Chir Main. 2010; 29:307–314.
26. Stafford PR, Norris BL. Reamer-irrigator-aspirator bone graft and bi Masquelet technique for segmental bone defect non-unions: a review of 25 cases. Injury. 2010; 41:Suppl 2. S72–S77.
27. Uzel AP, Lemonne F, Casoli V. Tibial segmental bone defect reconstruction by Ilizarov type bone transport in an induced membrane. Orthop Traumatol Surg Res. 2010; 96:194–198.
28. Scharfenberger AV, Alabassi K, Smith S, et al. Primary wound closure after open fracture: a prospective cohort study examining nonunion and deep infection. J Orthop Trauma. 2017; 31:121–126.
29. Dedmond BT, Kortesis B, Punger K, et al. The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibial shaft fractures. J Orthop Trauma. 2007; 21:11–17.
30. Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998; 12:1–7.
31. Tornetta P 3rd, Bergman M, Watnik N, Berkowitz G, Steuer J. Treatment of grade-IIIb open tibial fractures. A prospective randomised comparison of external fixation and non-reamed locked nailing. J Bone Joint Surg Br. 1994; 76:13–19.
32. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001; 83:62–68.
33. SPRINT Investigators. Bhandari M, Guyatt G, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): study rationale and design. BMC Musculoskelet Disord. 2008; 9:91.
34. Shepherd LE, Costigan WM, Gardocki RJ, Ghiassi AD, Patzakis MJ, Stevanovic MV. Local or free muscle flaps and unreamed interlocked nails for open tibial fractures. Clin Orthop Relat Res. 1998; (350):90–96.
35. Clifford RP, Beauchamp CG, Kellam JF. Plate fixation of open fractures of the tibia. Orthop Trauma Direct. 2009; 7:25–29.
36. Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix and flap: the radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br. 2000; 82:959–966.
37. Hertel R, Lambert SM, Müller S, Ballmer FT, Ganz R. On the timing of soft-tissue reconstruction for opesn fractures of the lower leg. Arch Orthop Trauma Surg. 1999; 119:7–12.
 XML Download
XML Download