

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the interstitial and appositional growth of greater trochanter post-screw apophysiodesis in Legg-Calve-Perthes (LCP) disease.
Materials and Methods
A total of 17 patients, who were diagnosed with LCP and underwent greater trochanter screw apophysiodesis and metal removal between December 2003 and December 2012, and were followed-up for at least 4 years, were selected. Anterioposterior radiologic images were taken in each process of apophysiodesis, metal removal, and last follow-up. From such images, articulotrochanter tip distance (ATD), trochanter tip-screw distance (TSD), trochanter tip-trochanter lower margin distance (TLD), and screw-trochanter lower margin distance (SLD) were measured. Appositional growth and greater trochanter growth rates were compared using paired t-test, independent t-test, and correlation analysis.
Results
The average ATD of the affected and unaffected sides was 14.2 and 16.8 mm, respectively at apophysiodesis and 9.2 and 14.8 mm at the last follow-up, with a significantly greater decrease observed on the affected side the unaffected side (p=0.030). TLD of the affected side during the follow-up increased 11.0 mm, from an average of 30.8 to 41.8 mm, while the un-affected side increased 14.3 mm, from an average of 26.7 to 41.0 mm. The growth of greater trochanter after the operation in the affected side was 76.7% of that in unaffected side. The ratio of TLD of the affected side to the unaffected side was significantly reduced, from 1.15 to 1.02 (p=0.014) at the final follow-up. TSD was significantly increased from 4.5 to 14.4 mm at metal removal (p<0.001) and increased to 17.0 mm at the last follow-up. Moreover, the ratio of TSD to SLD was significantly increased from 0.20 to 0.74 at metal removal (p<0.001) and increased to 0.84 at the final follow-up.
Figures and Tables
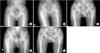 | Figure 1Radiographs of a 7-year-old boy with unilateral Legg-Calve-Perthes disease. The patient received shelf operation and screw apophysiodesis. Preoperative radiograph (A), postoperative radiograph (B), postoperative 4 years radiograph (C), radiograph of metal removal (52 months after screw apophysiodesis) (D), and radiograph of the final follow-up (E).
|
 | Figure 2Schematic drawing of the hip affected by left Legg-Calve-Perthes disease. The measurement of various radiological indices. Line ①: femoral head articular line (perpendicular to Line *), Line ②: greater trochanter tip line (perpendicular to Line *), Line ③: proximal screw neck line (perpendicular Line *), Line ④: greater trochanter lower margin line (perpendicular to Line *), Line *: anatomical axis of femur. ATD, articulo-trochanter tip distance; TSD, trochanter tip-screw distance; TLD, trochanter tip-trochanter lower margin distance; SLD, screw-trochanter lower margin distance.
|



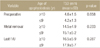
Table 5
TSD between the Two Groups (One Performing Apophysiodesis above Age of 10 Years and the Other Performing Apophysiodesis below Age of 9 Years)
![]()



References
1. Van Tongel A, Fabry G. Epiphysiodesis of the greater trochanter in Legg-Calvé-Perthes disease: the importance of timing. Acta Orthop Belg. 2006; 72:309–313.
2. Matan AJ, Stevens PM, Smith JT, Santora SD. Combination trochanteric arrest and intertrochanteric osteotomy for Perthes' disease. J Pediatr Orthop. 1996; 16:10–14.

3. Maquet P. Importance of the position of the greater trochanter. Acta Orthop Belg. 1990; 56:307–322.
4. Iwersen LJ, Kalen V, Eberle C. Relative trochanteric overgrowth after ischemic necrosis in congenital dislocation of the hip. J Pediatr Orthop. 1989; 9:381–385.
5. Leitch JM, Paterson DC, Foster BK. Growth disturbance in Legg-Calvé-Perthes disease and the consequences of surgical treatment. Clin Orthop Relat Res. 1991; (262):178–184.
6. Gage JR, Cary JM. The effects of trochanteric epiphyseodesis on growth of the proximal end of the femur following necrosis of the capital femoral epiphysis. J Bone Joint Surg Am. 1980; 62:785–794.
7. Litt R, Albassir A, Willems S, Debry R. Coxa vara. Isolated growth of the greater trochanter. Prevention-treatment. Acta Orthop Belg. 1990; 56:301–306.
8. Garrido IM, Moltó FJ, Lluch DB. Distal transfer of the greater trochanter in acquired coxa vara. Clinical and radiographic results. J Pediatr Orthop B. 2003; 12:38–43.
9. Takata K, Maniwa S, Ochi M. Surgical treatment of high-standing greater trochanter. Arch Orthop Trauma Surg. 1999; 119:461–463.
10. Hasler CC, Morscher EW. Femoral neck lengthening osteotomy after growth disturbance of the proximal femur. J Pediatr Orthop B. 1999; 8:271–275.
11. Fernbach SK, Poznanski AK, Kelikian AS, Tachjdian MO, Marzano MJ. Greater trochanteric overgrowth: development and surgical correction. Radiology. 1985; 154:661–664.
12. Schneidmueller D, Carstens C, Thomsen M. Surgical treatment of overgrowth of the greater trochanter in children and adolescents. J Pediatr Orthop. 2006; 26:486–490.
13. Edgren W. Coxa plana. A clinical and radiological investigation with particular reference to the importance of the metaphyseal changes for the final shape of the proximal part of the femur. Acta Orthop Scand Suppl. 1965; Suppl 84. 1–129.
14. Langenskiöld A, Salenius P. Epiphyseodesis of the greater trochanter. Acta Orthop Scand. 1967; 38:199–219.
15. McCarthy JJ, Weiner DS. Greater trochanteric epiphysiodesis. Int Orthop. 2008; 32:531–534.
 XML Download
XML Download