

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) is major cause of death in individuals with diabetes, and asymptomatic CAD develops more frequently in person with diabetes than in the healthy population. The prevalence of asymptomatic CAD and the incidence of sudden cardiac death are much higher in patients with a long duration of diabetes than in those with a short duration [1]. Thus, the integrated management of multiple risk factors including hypertension, dyslipidemia, and diabetes is essential for the prevention of future cardiovascular disease (CVD) [23]. In addition, early detection of patients at a high risk of CVD is critical.
Pulse wave velocity (PWV) is a simple, noninvasive method for estimating arterial stiffness, and it is a predictor of the severity of vascular damage [4] and the prognosis of CVD in patients with hypertension [5] and diabetes [6]. Brachial ankle pulse wave velocity (baPWV) measurements have recently become available as a tool for estimating PWV and baPWV can be measured more simply than the carotid-femoral PWV, which is not easy to measure in routine clinical settings. The baPWV is considered to be a simple tool for assessing vascular damage reflecting stiffness of the aorta and/or the peripheral arteries. The measurement of baPWV has been validated, and the reproducibility of baPWV was also previously reported elsewhere [78910].
The newest-generation multi-slice computed tomography (MSCT) is considered to be an accurate imaging method for detecting significant CAD; however, radiation exposure and its high cost restrict the use of MSCT as a screening tool to detect asymptomatic CAD [1112]. Recent studies have demonstrated that baPWV was closely associated with risk factors for CVD in patients with occult CAD detected by MSCT. However, in those studies, the participants were relatively healthy, as they drawn from members of the general population who underwent routine health evaluations, and the proportion of patients with diabetes was only 10% to 18% [1314].
However, there is little evidence regarding the relationship between baPWV and the presence of coronary artery stenosis (CAS) as evaluated by MSCT angiography in patients with type 2 diabetes mellitus who have atypical symptoms and equivocal exercise test results. The aim of this study was to evaluate the association of baPWV as an index of arterial stiffness in the lower-extremity arteries and CAS in patients with type 2 diabetes with atypical chest pain using non-invasive MSCT angiography. The associations of various CVD risk calculator with CAS were also evaluated.
METHODS
Study population
We retrospectively enrolled 83 patients over 30 years old with type 2 diabetes who underwent MSCT angiography for suspected CAD because of vague chest discomfort with inconclusive treadmill exercise electrocardiography (ECG) and/or nuclear stress test results between January 2008 and December 2009. An automatic pulse waveform analyzer was used to measure baPWV. The usual anthropometric and clinical laboratory data were collected from patients. Those who had previous atherosclerotic disease, including peripheral artery disease with a low ankle brachial index (<0.9), stroke, chronic kidney disease (estimated glomerular filtration rate <60 mL/min/1.73 m2), previous CAD, a history of percutaneous coronary intervention (PCI) or coronary arterial bypass surgery, or New York Heart Association class II to IV heart failure were excluded from the current study. Written informed consent was provided by all enrolled patients. This study was approved by the Institutional Review Board of Busan St. Mary's Hospital (Busan, Korea, IRB no. BSM 2008-04).
Anthropometric and laboratory evaluations
Blood pressure (BP) in the seated position was measured by a digital sphygmomanometer after at least 5 minutes of rest. The body mass index (BMI) was calculated as the weight in kilograms divided by the squared height in meters (kg/m2), using the values of the height and weight of the patients that were measured just before measuring baPWV. Fasting blood samples were concurrently collected on the day of the study and the usual clinical parameters were checked, such as fasting plasma glucose (FPG), aspartate aminotransferase, alanine aminotransferase (ALT), the lipid profile, and gamma glutamyl transpeptidase (γ-GTP). The fasting state was defined as a fasting duration of at least 8 hours. Hemoglobin A1c (HbA1c) was measured by high performance liquid chromatography using the Variant TM II Turbo (Bio-Rad Laboratories, Hercules, CA, USA). The patients' smoking status, alcohol intake, and medication use were evaluated by an electronic chart review and a questionnaire.
baPWV measurements
Patients were allowed to take their regular medications on the study day, and were examined in the supine position after 5 minutes of rest in a quiet room. A baPWV was measured using an automatic waveform analyzer (VP-1000, Colin, Komaki, Japan) according to the manufacturer's recommendations and a previous validated method [15]. Both left and right baPWVs were measured, and the higher value was defined as the maximum baPWV (max-baPWV) [16].
MSCT angiography and image analysis
Data were acquired using a 64 multi-detector computed tomographic scanner (Toshiba Medical Systems, Tokyo, Japan). Angiographic images were acquired with 16×0.75 mm slice collimation, a gantry rotation time of 420 ms, a tube energy of 120 kV, a table feed of 2.8 mm/rotation, and an effective tube current of 500 mAs according to a previously published protocol [1314]. An intravenous contrast agent (Visipaque, GE-Healthcare Amersham, Piscataway, NJ, USA) was injected at a rate of 4 mL/sec. A β-blocker (5 mg of metoprolol) was intravenously injected in all patients with a heart rate >65 beats per minute before the computed tomographic angiography scan. In this study, to estimate the degree of stenosis, we visually traced the coronary lumen at the point with maximal stenosis. Coronary stenosis was considered to be present if ≥20% stenosis of the coronary artery lumen was observed at the maximal stenotic site, and severe coronary stenosis was defined as the presence of ≥50% stenosis at the maximal stenotic site. The quantitative coronary artery calcium (CAC) score was measured using the most widely used method [17].
Coronary artery disease risk calculators
The United Kingdom Prospective Diabetes Study (UKPDS) Risk Engine program was downloaded from https://www.dtu.ox.ac.uk/riskengine/download.php. The American College of Cardiology/American Heart Association (ACC/AHA) atherosclerotic cardiovascular disease (ASCVD) risk estimator was downloaded from http://www.cvriskcalculator.com/ as a Microsoft Excel file. In addition, the Framingham risk calculator was downloaded from http://cvrisk.mvm.ed.ac.uk/calculator/excelcalc.htm as a Microsoft Excel file.
Statistical analysis
Data are expressed as mean±standard deviation (SD). The unpaired t test was used to assess differences in continuous variables, and the chi-square test was applied to categorical variables between subjects with and without CAS. Spearman correlation analysis was performed to evaluate the associations of the severity of CAS, with max-baPWV and other clinical variables. Age- adjusted partial correlation analysis was performed for statistically significant clinical variables. A receiver operating characteristic (ROC) curve analysis was performed to estimate the baPWV cut-off point predicting the presence of CAS. The value with the highest sum of sensitivity and specificity was identified as the cutoff point. The predictive accuracy of the parameters was calculated as the area under the curve (AUC). We used a comparative ROC curve analysis to test the statistical significance of the differences among the various CVD calculators and max- baPWV for predicting CAS. Multivariable logistic regression analysis was performed to assess independent associations between the presence of CAS and baPWV after adjusting for age, sex, hypertension, smoking, and dyslipidemia. MedCalc (MedCalc Software, Mariakerke, Belgium) was used for all statistical analyses. A P values <0.05 were considered to indicate statistical significance.
RESULTS
Clinical characteristics of the patients
The baseline clinical characteristics of the patients with or without CAS (≥20%) are shown in Table 1. The proportion of patients with CAS (≥20%) and severe CAS (≥50%) was 43 of 83 (51.8%) and 34 of 83 (40.9%), respectively. Most patients with CAS (34 of 43, 79.1%) had severe CAS. CAS was associated with old age, current smoking, and a longer duration of diabetes. Max-baPWV was significantly greater in patients with CAS than in those without CAS. The scores of the UKPDS Risk Engine, the ACA/AHA ASCVD risk calculator, and the Framingham risk calculator were significantly higher in patients with CAS. However, there were no statistically significant differences in BMI, BP, HbA1c, total cholesterol, low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol, triglycerides, ALT, GTP, or FPG between patients with and without CAS. There were no significant differences in statin use, anti-platelet agent use, renin-angiotensin system blockers, and insulin therapy between the two groups (Table 1).
Correlations between CAS, baPWV, and other variables
The severity of CAS showed significant correlations with age, the amount of cigarette smoking (pack-years), max-baPWV, duration of diabetes, the UKPDS Risk Engine score, the ACC/AHA ASCVD risk estimator score, the Framingham risk calculator score, and the CAC score (Table 2). After age adjustment, the severity of CAS showed a significant correlation with amount of cigarette smoking (pack-years), duration of diabetes, the UKPDS Risk Engine score, the ACC/AHA ASCVD risk estimator score, the Framingham risk calculator score, and the CAC score. However, the severity of CAS was not associated with max-baPWV after adjustment for age (Table 2).
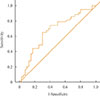
Fig. 1 shows the ROC curve of the association between baPWV and the presence of CAS in patients with type 2 diabetes. The AUC was 0.672 (95% confidence interval [CI], 0.554 to 0.785; P=0.010). ROC curve analysis showed that the best cutoff point for a baPWV value predicting the presence of CAS was 1,650 cm/sec. When a baPWV greater than 1,650 cm/sec was used as the cutoff value, sensitivity and specificity were 68.9% and 63.2%, respectively. In a comparative ROC curve analysis, no significant difference was found between max-baPWV and three CVD estimating calculators (Table 3, Fig. 2).
In the multivariable analysis, a baPWV >1,650 cm/sec was an independent predictor of the presence of CAS (≥20%) after adjusting for potential confounders including age, sex, hypertension, dyslipidemia, and smoking (odds ratio, 4.34; 95% CI, 1.19 to 15.79; P<0.026) (Table 4).
DISCUSSION
The present study showed that baPWV can be used as a screening tool for patients with type 2 diabetes at risk of developing atherosclerosis and that a higher baPWV is a significant predictor of CAS as detected by MSCT coronary angiography. Our study suggests that baPWV value above a cutoff value of 1,650 cm/sec may be an acceptable predictor of occult CAD in patients with diabetes.
PWV reflects arterial stiffness, which is caused by a central elastic component and a peripheral muscular component, and the latter is greater in baPWV than in carotid-femoral PWV [18]. Elevated baPWV values have been observed in patients with CVD risk factors, including hypertension, diabetes, and dyslipidemia. Many studies have evaluated the use of baPWV to predict cardiovascular risk, and it has been widely measured in various clinical situations [16171819]. In patients with diabetes, baPWV was found to be closely associated with age and BP [1619]. Nakamura et al. [20] suggested that baPWV may be useful for assessing macrovascular damage, and Choi et al. [21] reported a close association of baPWV with the CVD risk factors of metabolic syndrome. Various cutoff values have been proposed. In a recent study, a baPWV cutoff value of 1,400 cm/sec was found to be useful for risk stratification by the Framingham score and for detecting of patients with atherosclerotic CVD [22]. Several other studies have proposed baPWV cutoffs of 1,400 to 1,800 cm/sec for the prediction of cardiovascular risk factors or overt CAD with high diagnostic accuracy [131423].
In our study, a baPWV >1,650 cm/sec was an independent marker of the presence of CAS (≥20%) after adjusting for various confounders including age, sex, smoking, hypertension, and dyslipidemia in the multivariable analysis. Therefore, we think that the presence of CAS might be detected by the use of baPWV in patients with diabetes. We also determined the prognostic ability of high baPWV (>1,650 cm/sec) for the presence of CAS in patients with diabetes, finding a sensitivity of 70% and a specificity of 63%. These results suggest that it may be necessary to perform a non-invasive study such as an exercise treadmill test or myocardial scintigraphy if a high value of baPWV is documented in patients with diabetes. However, whether a coronary evaluation of patients is indicated should be decided based on their clinical presentation, including their history of angina symptoms, ECG, and echocardiographic findings.
Arterial stiffness increases systolic BP, whereas it decreases diastolic BP, resulting in a wide pulse pressure [24,25]. The increased systolic BP has a negative effect on the heart due to an increased workload, while a reduced diastolic BP may limit coronary artery perfusion. Cross-sectional studies have proposed that these effects may explain the association between arterial stiffness and acute coronary syndrome [2627]. However, hemodynamic data and coronary risk factors including BP, pulse pressure, total cholesterol, LDL-C, triglycerides, and plasma glucose were not significantly associated with the presence of CAS in our study. This may be explained by the fact that a significant proportion (>60%) of the patients with CVD risk factors in our study had been previously treated with statins, anti-platelet agents, and renin-angiotensin receptor blockers. The strong association between max-baPWV and the presence of CAS in patients with diabetes observed in our study may provide an additional explanation for the association between arterial stiffness and CVD.
In our study, the presence of CAS (≥20%) was closely associated with baPWV in the AUC analysis but the presence of significant CAS (≥50%) was not. Seo et al. [27] evaluated the predictive value of baPWV for CAD risk, and found that baPWV did not have a significant association with coronary stenosis. We suggest that the finding in this study of no relationship between baPWV and significant CAS was related to the fact that severe CAS was defined by ≥50% occlusion. Because baPWV reflects arterial stiffness, it is likely to be correlated with early-stage CAD, but not advanced CAD.
Various tools have used to evaluate the risk of CVD in advance. The UKPDS Risk Engine was developed to estimate the risk of CAD in diabetic patients [28]. The ASCVD risk estimator can evaluate the 10-year risk of CAD in adults aged 40–79 [29]. The Framingham risk calculator can be used to evaluate the risk of various atherosclerotic CVD events [30]. In our study, the relationship between the presence of CAS and scores on these three risk estimating tools (the UKPDS Risk Engine, the ASCVD risk estimator, and the Framingham risk calculator) was quite strong. In several studies, the predictive value of these evaluation tools was compared with that of non-invasive exams, and the predictive value was found to be improved by using these tools together with non-invasive exams [313233]. In our study, the predictive value of baPWV for CAD was compared with that of various risk evaluation tools, and the value of baPWV was somewhat lower than that of the other risk evaluation tools. However, no significant difference was found between the predictive value of max-PWV and the three CVD estimating calculators (Fig. 2).
In current clinical practice, the management of patients with CAD depends on an initial clinical evaluation, with higher-risk patients referred for a conventional coronary angiogram and PCI in most cases [34]. However, MSCT coronary angiography is a reliable, noninvasive imaging modality for the diagnosis of CAD. The negative predictive value of MSCT angiography is approximately 100%, allowing CAD to be ruled out [3335]. Based on the diagnostic accuracy of MSCT coronary angiography, we used this noninvasive modality as a diagnostic tool to define CAS in our study population instead of conventional coronary angiography.
Our study has some potential limitations. First, the current study was a single-center, retrospective study. Second, a gross examination of the coronary angiographic data was not performed to determine the degree of coronary artery narrowing. Third, there might have been many confounding factors that could not be properly adjusted for in the quantitative analysis of CAS. In addition, we were not able to obtain comprehensive data regarding the total atherosclerotic burden of the entire coronary tree, although baPWV may be more closely related to the total coronary atherosclerotic burden than the severity of coronary stenosis. Last, the present study included a relatively small number of patients.
In conclusion, this study showed a significant correlation between max-baPWV and a noninvasive MSCT angiographic assessment of CAD in patients with type 2 diabetes with atypical symptoms and inconclusive stress test results. In addition, this study suggests that the cutoff value of 1,650 cm/sec for baPWV can be an acceptable marker for predicting CAD in patients with type 2 diabetes. Further studies are needed to evaluate whether specific values of baPWV may be related to adverse clinical outcomes in patients with type 2 diabetes.





 XML Download
XML Download