

 PDF
PDF ePub
ePub Citation
Citation Print
Print


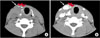
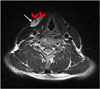
A 34-year-old man presented with a 1-month history of a slowly growing mass on the rightside anterior neck. The patient did not present any symptoms related to the neck mass. On physical examination, a compressible, non-pulsatile mass on the neck was enlarged with the Valsalva maneuver (Video). The Doppler ultrasound demonstrated a low-flow vascular lesion in the right-side of the neck. Non-contrast computed tomography (CT) scan showed a isodense mass about 2.7 cm with phleboliths which was heterogeneously enhanced after contrast media administration (Fig. 1). On magnetic resonance imaging (MRI), the mass appeared hyperintense on the fat-saturated T2-weighted image and had low signal-intensity foci which was indicative of phleboliths (Fig. 2). The mass showed diffuse enhancement on the enhanced T1-weighted image. Based on these findings, the patient was diagnosed with a venous malformation. Although the main treatment of venous malformation is sclerotherapy, the patient underwent surgical excision. A histopathological examination of the resected specimen was consistent with venous malformation. The patient is doing well on follow-up. This study was approved by the institutional review board of the Chonnam National University Hwansun Hospital.
Vascular malformations include capillary malformation, venous malformation, lymphatic malformation, arteriovenous malformations, and combined malformations.12 Venous malformation is the most common type of vascular malformation.123 Venous malformation is a low-flow vascular malformation like capillary and lymphatic malformations. Doppler ultrasound, CT scans and MRI are useful and reliable imaging methods used for diagnosis of venous malformations.12 Treatment for venous malformations is percutaneous embolization, percutaneous sclerotherapy, and surgery.1 The main treatment of venous malformation is sclerotherapy. However, considering the form, location, and extent of the venous malformation, the patient underwent complete surgical resection.
In conclusion, we report the case of venous malformation, which was successfully diagnosed by physical examination and several radiologic examinations, such as Doppler ultrasound, CT, and MRI. In addition, we finally confirmed the venous malformation through histopathologic examination.
 XML Download
XML Download