

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the incidence of gastric carcinoma is declining, it remains one of the leading causes of death from malignant tumors worldwide. A large number of patients are diagnosed at a late stage with non-curative factors, and the prognosis of gastric carcinoma patients with non-curative factors is still poor.1 Surgery is the only potentially curative modality for localized gastric carcinoma. However, the benefits of resection in gastric carcinoma patients with non-curative factors remain controversial. Several studies reported that resection might provide some survival benefits to these patients, regardless of curability.2345 However, other studies reported no survival advantage for resection in gastric carcinoma patients with non-curative factors.67 In the current study, we analyzed the records of gastric carcinoma patients with non-curative factors retrospectively to identify their clinicopathological characteristics and outcome. We also evaluated the benefits of resection in this group of patients.
MATERIALS AND METHODS
1. Patients
A total of 3,299 patients were diagnosed with gastric carcinoma and treated at the Division of Gastroenterologic Surgery, Department of Surgery, Chonnam National University Hospital, Gwangju, Korea in the 15 years from 1996 to 2010. The current study reviewed the records of only the 467 patients with non-curative factors. The effects of age, gender, tumor size, tumor location, the presence of hepatic metastasis and peritoneal dissemination, histological type, intravenous chemotherapy, the number of non-curative factors, and the effects of resection on survival were examined. Pathological evaluations were performed according to the Japanese Gastric Cancer Association guidelines.8 A gastric resection was defined as being non-curative in cases with at least one non-curative factor (non-resectable distant metastases-liver, bone, lung, and para-aortic lymph nodes, non-resectable lymph nodes, or peritoneal metastasis). All were palliative in this study. The data were analyzed statistically using Chi-squared tests. The overall survival rates were calculated using the Kaplan-Meier method, and the differences between the curves were evaluated using log-rank tests with p-values of <0.05. Multivariate survival analysis was performed with the Cox proportional hazards model in a stepwise manner with a likelihood ratio test for selection of variables. This study was approved by the Institutional Review Board of the Clinical Research Institute of Chonnam National University Hwasun Hospital (IRB No. CUHH-2017-168).
RESULTS
Of the 3,299 patients diagnosed with gastric carcinoma treated in our hospital during the 15-year study period, 467 (14.2%) had non-curative factors. Table 1 summarizes the clinicopathological features of the 305 (65.3%) of these gastric carcinoma patients who underwent resection and the 162 patients that did not (bypass and exploration). No significant differences were observed in the mean age of the patients who did or did not undergo resection (56.5 vs. 56.7 years, respectively). Of the 305 patients who underwent resection, 217 (71.1%) were male and 88 (28.9%) were female, compared with 124 males (76.5%) and 38 females (23.5%) in the group that did not undergo resection. There were more males than females in each group (71.1 vs. 76.5%, respectively); however, the difference in the gender ratio between the groups was not significant. The mean tumor size was smaller in patients who underwent resection compared with those who did not undergo resection (6.9 vs. 7.9 cm, respectively); this difference in mean tumor size was significant (p<0.001).
In the patients undergoing resection, most of the gastric carcinomas were located in the lower third of the stomach (185 cases; 60.7%), and the difference in tumor location between the groups was significant (p<0.001). According to the grade of anaplasia, most gastric tumors in both groups were undifferentiated adenocarcinomas (62.3 vs. 85.2%, respectively); the difference in histological type between the groups was significant (p<0.001). Hepatic metastases were found in 27.2% of the resection group and 28.4% of the non-resection group; this difference was not significant. However, there was a significant difference in the frequency of peritoneal dissemination between the two groups (25.6 vs. 70.4%, respectively p<0.001). In resection group, 277 individuals (90.8%) had one non-curative factor and 28 had more than two factors. There was a statistically significant difference in the number of non-curative factors in patients who underwent resection compared with those who did not (p<0.001). Using Cox's proportional hazards regression model, two factors were independent, statistically significant prognostic parameters, peritoneal dissemination (risk ratio, 0.74; 95% confidence interval, 0.57–0.96; p<0.05) and intravenous chemotherapy (risk ratio, 2.84; 95% confidence interval 1.19–2.47; p<0.05) affecting survival for gastric carcinoma patients with non-curative factors. The clinicopathological variables tested using univariate analyses are shown in gastric carcinoma patients who had non-curative factor with resection in Table 2. The factors that influenced the survival rate were tumor size and the presence of peritoneal dissemination. Using a Cox's proportional hazards regression model, only one factor was an independent statistically significant prognostic parameter: the presence of peritoneal dissemination (risk ratio, 1.37; 95% confidence interval, 1.04–1.79; p<0.05) (Table 3).
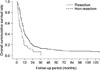
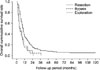
Fig. 1 shows the patient survival rates according to operation type. The 3-year survival rate was higher in gastric carcinoma patients with non-curative factors who underwent resection (13.2%) compared with those who did not (7.2%; p<0.001) (Fig. 1). When the 3-year survival rates of patients with peritoneal dissemination according to the type of operation were examined, the rate was higher in individuals who underwent resection (9.5%) compared with those who did not (0.0 vs. 4.7%, respectively; p<0.001) (Fig. 2).
DISCUSSION
Although the incidence of gastric carcinoma is declining, it remains one of the leading causes of deaths from malignant tumors worldwide. The surgical management of gastric carcinoma patients with non-curative factors remains controversial, and the benefits of resection in these patients are unclear. In this retrospective study, we analyzed the records of gastric carcinoma patients with non-curative factors to identify their clinicopathological characteristics and examine the survival benefits of resection.
Regarding the prognosis of patients with incurable gastric carcinoma, some reports have suggested that resection may increase survival rates.2345 Specifically, the mean survival time of patients who underwent resection was 8.0–16.3 months, compared with 2.4–6.7 months in those who did not undergo resection. In terms of selecting patients for resection, some authors recommended resection only in individuals with a single, non-curative factor.2 Furthermore, some investigators suggested that a total gastrectomy should be performed in some patients because of the high morbidity rates despite a survival benefit.9 In contrast, other studies stated that there was no survival benefit from resection in patients with non-curative factors.67 The authors of these studies suggested that there might be no need for palliative gastrectomy in patients with incurable gastric carcinoma who did not have bleeding or obstruction. The findings of the present study are compatible with those that report a benefit of resection. The 3-year survival rate was higher in patients who underwent resection (13.2%) compared with those who did not (7.2%) (p<0.001), regardless of curability.
In this study, Cox's proportional hazard regression analysis revealed that peritoneal dissemination was the only independent prognostic factor in gastric carcinoma patients with non-curative factors. The management of gastric carcinoma patients with peritoneal dissemination remains controversial, and the benefits of resection are unclear. Generally, palliative resection for gastric carcinoma patients with peritoneal dissemination is indicated for those who have a small number of peritoneal metastases. Some investigators advocated that surgical treatment should not be recommended as long as the patient's food intake and hematological status were good, and that resection should be used instead to improve the patient's status.10 In contrast, others studies reported that resection has beneficial effects on the postoperative course of gastric carcinoma patients with peritoneal dissemination.611 There was also a survival benefit of resection in gastric carcinoma patients with peritoneal dissemination. The 3-year survival rate was higher in patients who underwent resection (9.5%) compared with those who did not (bypass and exploration, 0.0 and 4.7%, respectively; p<0.001).
The reported rates of morbidity and mortality in gastric carcinoma patients with non-curative factors after resection vary. Despite recent advances in operating techniques, nutritional support, and antibiotics, the reported morbidity and mortality related to non-curative resection is 3.8–49% and 0–34%, respectively.251213 Some authors reported that the postoperative morbidity and mortality were 11.9% and 4.7%, respectively, even in elderly patients.14 They recommended that individual surgeons must consider multiple factors whenever considering a treatment plan for these advanced patients, including age, comorbidities, and the extent of the disease. In the current study, the postoperative mortality rate for gastric carcinoma patients with non-curative factors who underwent resection was acceptable: five postoperative deaths occurred after resection. There was a 1.6% mortality rate, which is consistent with that reported previously. The main morbidity was leakage, which was also consistent with a previous report15; this complication was managed successfully. We believe that the low operative mortality rate might have contributed partially to the better survival of patients with incurable factors who underwent gastrectomy.
The effect of postoperative chemotherapy in gastric carcinoma patients with non-curative factors remains controversial. Some investigators found that postoperative chemotherapy does not affect the prognosis of patients with gastric carcinoma.916 In contrast, other reports showed that palliative gastrectomy combined with adjuvant chemotherapy improved the survival of patients with metastatic gastric carcinomas.3712 As the chemotherapy regimen varied throughout the current study period, we did not evaluate the survival benefits of chemotherapy. Nevertheless, we reported a survival benefit of postoperative chemotherapy in gastric carcinoma patients with peritoneal dissemination previously.17
The current results highlight the improved survival of gastric carcinoma patients with non-curative factors who underwent resection compared with those who did not undergo resection. Although resection is not curative in this group of patients, we still recommend performing the procedure.



 XML Download
XML Download