

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Incident fracture (osteoporosis-related fractures [ORFs]) have major economic and social impacts, with serious morbidities and increased mortality following hip and/or vertebral fractures.[12] Many postmenopausal women at risk of fracture will be missed based on bone mineral density (BMD) assessment alone,[12] a finding that is related to the multiple determinants of bone fragility, including age, fracture history, and deterioration of bone quality.[2] Identifying new biomarker(s) independent of BMD to improve fracture prediction is needed. Bone turnover markers (BTMs), particularly those of bone resorption, can predict fracture risk among postmenopausal women.[3] Such prediction may improve if BTMs are assessed along with BMD.[45] One possible new biomarker is plasma sphingosine 1-phosphate (S1P).
S1P is a bioactive lysophospholipid, autocrine-paracrine signaling molecule that regulates multiple cellular processes, including migration, proliferation, differentiation, and apoptosis, in many cell types.[678] S1P plays an important role in bone metabolism as a coupling factor between bone resorption and formation. It is also produced by osteoclasts to stimulate proliferation, migration, and survival of osteoblasts, possibly leading to bone formation stimulation.[678] Conversely, S1P augments osteoclastogenesis via induction of receptor activator of nuclear factor-κB ligand (RANKL) in osteoclasts and T-cells.[9] A concentration gradient of S1P is formed between circulation and bone tissue whereby osteoclast precursor cell movement is facilitated by chemo-repulsion mediated by S1P receptor 2 (S1PR2) signaling.[10] Such observations suggest that S1P affects osteoclasts, leading to increased bone resorption.[8] Furthermore, S1PR2-deficient mice exhibit moderate osteoporosis due to a decrease in osteoclastic bone resorption.[11] Recently in a case-control study, Kim et al.[12] demonstrated markedly higher S1P levels in 69 postmenopausal women with vertebral fractures than those in 69 non-fractured age and body mass index (BMI) matched controls, with S1P levels inversely correlated with BMD at various sites and positively correlated with bone resorption markers (BRMs). These data suggest that circulating S1P level could serve as a new biomarker of fracture risk. However, Heilmann et al.[13] using systemic FTY720 (an S1P analog) treatment did not improve fracture healing in experimental mice although several in vitro studies demonstrated osteoanabolic effects [1415] and improved bone defect healing.[16]
We hypothesized that postmenopausal women with higher circulating S1P levels have a greater ORF risk. We examined the association between plasma S1P levels and ORF risk in a prospective cohort of postmenopausal women aged ≥50 years in the Center of Excellence for Osteoporosis Research (CEOR) study.
METHODS
1. Study design
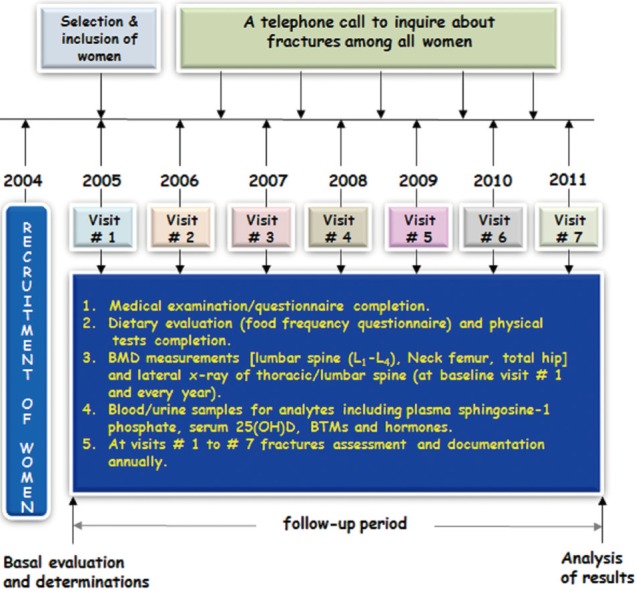
The CEOR study is an ongoing prospective, population-based cohort of 912 women aged ≥50 years residing in the Jeddah area of Western Saudi Arabia who were recruited in 2004. The study investigated the determinants of bone loss and fractures among healthy postmenopausal women. The rationale and design of the study as well as sampling and data collection have been described previously.[517] The baseline evaluation included 3,015 women. At enrollment, women were eligible for the study if they were aged ≥50 years, had been postmenopausal for >1 year (with serum FSH levels >15 mIU/L), were independently mobile and on an unrestricted diet. Exclusion criteria included a cancer history (n=11), regardless of type and stage) and current diagnosis of or prior therapy for osteoporosis (n=15). Women were also ineligible at enrollment if they had diseases or conditions that could interfere with bone metabolism or if they used anti-osteoporotic treatments (n=36), bisphosphonates, estrogen, calcitonin, fluoride salts, calcitriol, strontium or selective estrogen-receptor modulators). Women were also excluded if they had fever (oral temperature ≥38.0℃) or abnormal findings on complete blood cell counts including platelets and/or leukocytes (n=305). Women with abnormal hepatic, renal or thyroid function tests were also excluded (n=1,736). All women provided written informed consent for study participation. The study was approved by the Human Research Ethics Committee of CEOR, King Abdulaziz University. During the follow-up, of the 912 women initially recruited (fulfilling inclusion criteria), 148 were lost to follow-up, 20 died and 37 withdrew. The present study investigated 707 healthy postmenopausal women (mean age, 61 years; range, 53–93 years) from the CEOR cohort at the sixth annual follow-up for whom blood and urine samples were obtained at the baseline and follow-up visits. Women were followed with the intention to treat from the baseline visit to fracture, completion of the follow-up period, withdrawal from the study, or loss to follow-up or death, if no fracture had occurred. The participants received vitamin D and calcium supplementation to maintain the serum 25-hydroxy-vitamin D (25[OH]D) concentration >50 nmol/L and eura parathyroidism. Among the women who completed the study, plasma S1P and BTM levels, along with other analytes, were evaluated during the baseline visit, the 1-year follow-up visit, and annually thereafter (Fig. 1). Additional baseline assessments (using a questionnaire) included information on medical history, menopausal age, years since menopause, socioeconomics, education level, family history of fragility/fracture(s), and occurrence of a fall(s) during the past year. Information on smoking, physical activity (PA), vitamins and medication use were also recorded. Height and weight, as well as hip and waist circumferences, were measured while the women were wearing lightweight clothing with no shoes. BMI and the waist-to-hip ratio were also calculated. Cumulative PA scores from 0 to 27 were constructed based on the 7-day PA record described previously.[1] Women were classified into either sedentary (PA-score ≤14) or moderate/high activity (PA-score >14) groups. Hand-grip strength was measured using a JAMAR-Plus hand dynamometer (Sammons Preston, Bolingbrook, IL, USA) on both hands. Dietary intake of calories, protein, calcium and vitamin D were assessed using a food-frequency questionnaire.[17]
2. Assessment of fractures
Research physicians at CEOR monitored the enrolled women for incident fractures, which were recorded using CEOR's information system network. Two research physicians classified fracture events independently according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10).[18] A radiologist and/or an orthopedic surgeon reviewed all coded events for final fracture classification. Only low-trauma fractures (i.e., falls from standing height or less) were considered and classified as incident fragility fractures. Incident fractures were reported during annual follow-ups, and all peripheral fractures were confirmed by radiographs or a surgical report, as described previously.[17]
We excluded all non-ORFs (i.e., accident-related fractures such as a traffic road accident or a fall from a height higher than a chair or the first rung of a ladder or severe trauma; and all finger, toe, skull, and facial fractures). The specific fractures and fracture follow-up times were recorded at different sites during a follow-up period when a woman sustained an incident first fracture. The follow-up period was calculated as the time from the baseline visit to the first fracture, death, or the end of the study, whichever occurred first.[17] For women lost during the follow-up, the period was computed as the time from enrollment to the date of last contact. For incident vertebral fractures, lateral X-ray films of the thoracic and lumbar spine were obtained at baseline and annual visits for all women, and at the end of the study. All prevalent and incident vertebral fractures were identified by a radiologist as described by Genant et al.[19]. A prevalent fracture was defined as a vertebral body with a semi-quantitative grade ≥1. Any new vertebral fracture was identified by an increase of at least one grade in a vertebral body that was defined as normal at baseline. We excluded vertebral fractures due to major trauma, and/or vertebral deformities with non-osteoporosis causes (e.g., osteoarthritis and/or bone diseases). All vertebral and non-vertebral fractures were included in the final analyses.
3. Assessment of BMD
The BMD (lumbar spine [L1-4] and the mean of the proximal right and left femur [total and sub-regions]) was measured by dual energy X-ray absorptiometry using the Lunar Prodigy Model (Lunar Corp., Madison, WI, USA). Quality-control procedures were performed according to the manufacturer's recommendations.[17]
4. Measurement of plasma S1P levels and analytes
During the baseline and follow-up visits, venous blood samples were collected between 9:00 and 11:00 a.m. after an overnight fast under standardized conditions. Second-void morning urine samples were collected on the same day of blood sampling. The blood was centrifuged, and plasma (sodium citrate- or EDTA-treated), serum, and urine samples were stored in liquid nitrogen at −190℃ at the Biobank Unit of CEOR until they were analyzed. Plasma (treated with sodium citrate) S1P was measured using a competitive ELISA kit (Echelon Biosciences, Salt Lake City, UT, USA) according to the manufacturer's instructions.[20] All plasma samples showing hemolysis or clotting were discarded. However, no sample was collected immediately following any ORF. For women with ORFs, samples (n=9 women) were collected at least 3 months following the incident, and adjustments were made for the collection time. [17] The lower detection limit was 0.06 µmol/L with intra-assay and inter-assay coefficients of variations equaling 6.3% and 5.9%, respectively. Duplicate samples were assayed, and all results were reported as means. Plasma samples were diluted by a factor of 1/10. Further validation studies were performed for this assay. Linearity was assessed by serially diluting samples with sample diluents (dilutions 1:15, 1:20, and 1:30) and comparing observed values with expected values (observed recoveries range, 101%–109%) (data not shown). Additionally, recovery of spiked standards was tested by adding different S1P concentrations (three different concentrations) to eight different human plasma samples presented with various levels of endogenous S1P. Spiked recovery ranged from 90% to 106% (data not shown). No sample tested had S1P values below the lower limit of detection or above the upper limit of quantitation corresponding to 2.0 µmol/L. Other biochemical tests were performed at the Diagnostic laboratory of CEOR according to standard methods as described previously [2122].
5. Fracture risk assessment tools evaluation
BMD (g/cm2) was determined as described before.
Part of the withdrawn fasting blood sample was used for serum preparation to measure the biochemical BTMs. Moreover, urine samples were obtained in morning. Serum bone alkaline phosphatase (s-bone ALP), serum procollagen type 1 N-terminal propeptide (s-P1NP) , urinary cross-linked C-terminal telopeptide of type 1 collagen (CTX) and serum N-terminal telopeptide of collagen type I (NTx) were measured using competitive inhibition enzyme linked immunoassay by the commercially available kits.
Serum follicle stimulating hormone (FSH), luteinizing hormone, E2 and intact-parathyroid hormone were also, measured by commercially available immunoassays using Elecsys autoanalyzer (Roche Diagnostics GmbH, D-68298. Mannheim, Germany). The intra- and inter-assay coefficient of variations (CVs) were less than 4.0%. Serum 25(OH)D was measured by direct competitive chemiluminescence immunoassay using LIASON autoanalyzer (DiaSorin Inc., Stillwater, MN,. USA). The intra- and inter-assay CVs were 7.8% and 3.8% respectively.
6. Statistical analysis
Results are presented as means±standard deviation (SD), and categorical variables are expressed as frequencies. Data were analyzed using SPSS version 17.0 software (SPSS Inc., Chicago, IL, USA). Analysis of variance or the Mann-Whitney test was used, as appropriate, to examine differences among the groups for different variables and χ2 test for categorical variables to test for significant differences among groups. Correlation analysis was performed using Pearson's test. Partial correlation analysis was performed to adjust for various possible confounders. The relationship between incident fracture risk and various plasma S1P levels was evaluated using SD score changes and quartile-based analysis. The SD score was calculated using the formula (S1Pi–S1Pm)÷SD, where S1Pi is the individual S1P level, S1Pm is the mean cohort S1P level, and SD is the SD of cohort S1P levels. This calculation was used to determine the change in incident fracture risk for each incremental increase of 1-SD in S1P levels. Similar calculations were made for BTMs. Plasma S1P and BTMs were categorized into Quartiles, and the lowest Quartiles were compared to the fourth (highest) or other Quartiles. Quartiles were calculated for the following variables: age, years since menopause, dietary calcium intake, serum 25(OH)D, PA score, hand-grip strength, and BMD measurement at all sites. Cox proportional hazards regression analysis was used to estimate fracture risk. Data were used to estimate the hazard ratios (HRs) by Quartile and per SD increase in plasma S1P and other BTMs, and results were reported as HRs with estimation of 95% confidence intervals (CIs). In the Cox model, the follow-up time describes the time from the baseline visit to (a) the first fracture; or (b) completion of the follow-up period; or (c) death, if no fracture had occurred. The first fracture was considered the analysis endpoint. HRs were computed by comparing women with and without a fracture. Cox regression analysis was performed for different times: 2.0, 3.0, 5.0, and 6.0 years after collecting samples of the baseline visit. All fracture risk estimates were adjusted for age, BMI, and other confounders as appropriate. The population attributable risk (PAR) proportion was calculated according to the formula {Px(RR–1)÷ [1+Px(RR–1)]}×100, where P is the percentage of the population exposed, and RR is the relative risk.[23]
RESULTS
1. Baseline characteristics
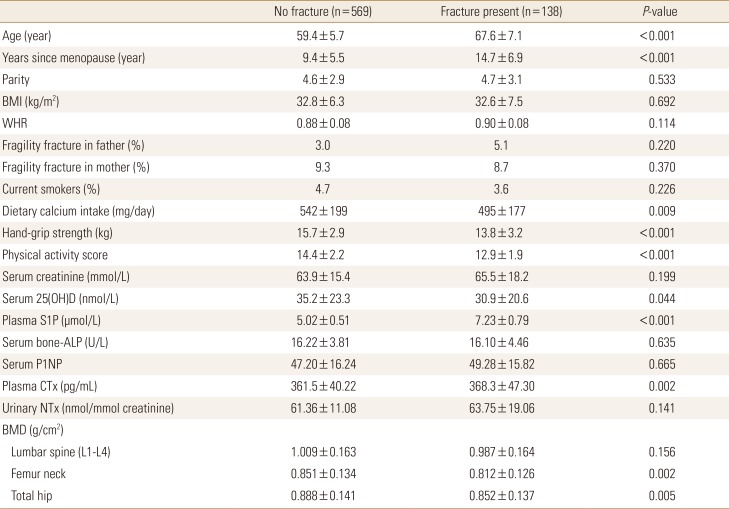
Baseline characteristics of the participants are presented in Table 1. During the mean follow-up period of 5.2±1.3 years, 138 women sustained ORFs: 44 vertebral fractures and 104 non-vertebral fractures (52 wrist, 12 hip, 21 rib, 8 humerus, 4 ankle, 5 metatarsal, and 2 pelvic) were documented. Women who had no fracture (n=569) were used as age and BMI matched control group in all analyses. As expected, women with ORFs were older, had higher number of years since menopause, lower values for BMD and lower hand-grip strength and PA-score values. Plasma S1P levels were significantly higher in women with ORFs than in women without fractures (7.23±0.79 vs. 5.02±0.51 µmol/L; P<0.001) with no significant difference in BTMs except for plasma CTX (p-CTX) (P=0.002). The mean plasma S1P values at baseline and at different time-point measurements are shown in Table 2. The plasma S1P levels remained stable during the follow-up period with only minor but significant increases (1.94%/year; P<0.001) for all women studied. Approximately 76% to 93% of women remained in the same plasma S1P Quartile at baseline and at the 5-year interval (data not shown). Of those at the highest Quartile at baseline, 89% remained at the highest Quartile also 5 years later (data not shown). Women who had fractures during the follow-up period had constantly high plasma S1P at baseline and at different time-point measurements (Table 2).
Stratifying the participants into three groups according to the number of incident fracture (i.e., no fracture, single or multiple fractures) demonstrated that plasma S1P levels (µmol/L) were significantly higher in women with single (7.03±0.71) or multiple fractures (7.92±0.64) than in those without fractures (5.02±0.51), (P-value for trending P<0.001). After adjustment for BMD value of the lumbar spine (L1-4) or total hip, statistical significance persisted. Plasma S1P levels in vertebral fractures (7.12±0.87) was not significantly different from women with non-vertebral fractures (7.27±0.75).
2. Plasma S1P levels in relation to fracture risk and BMD
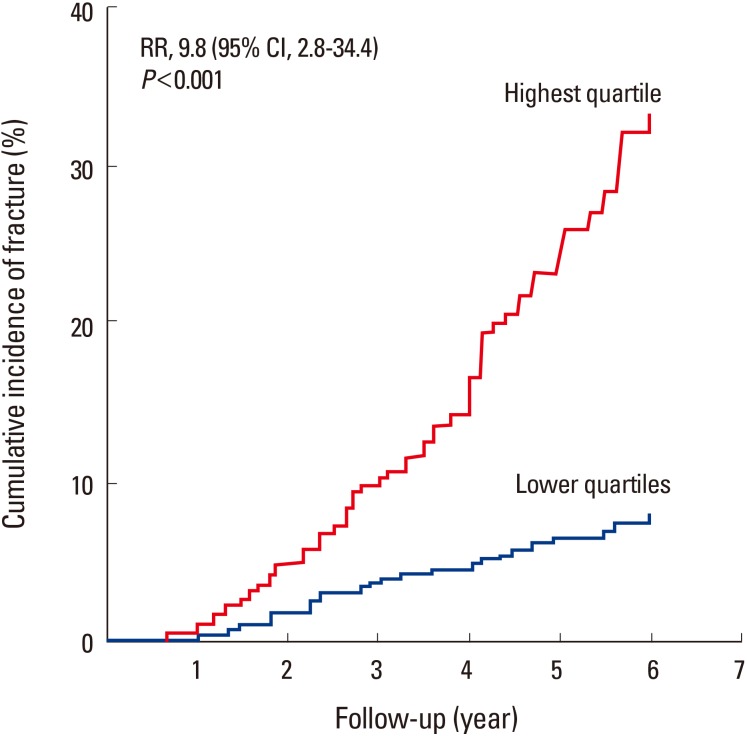
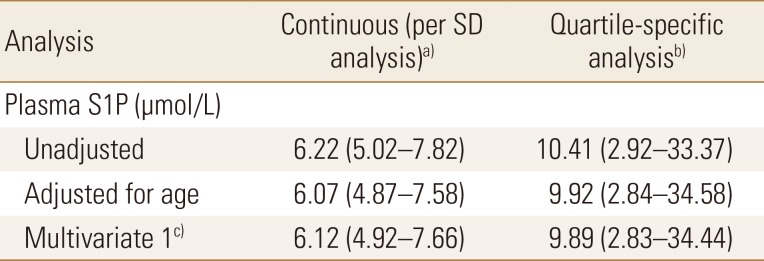
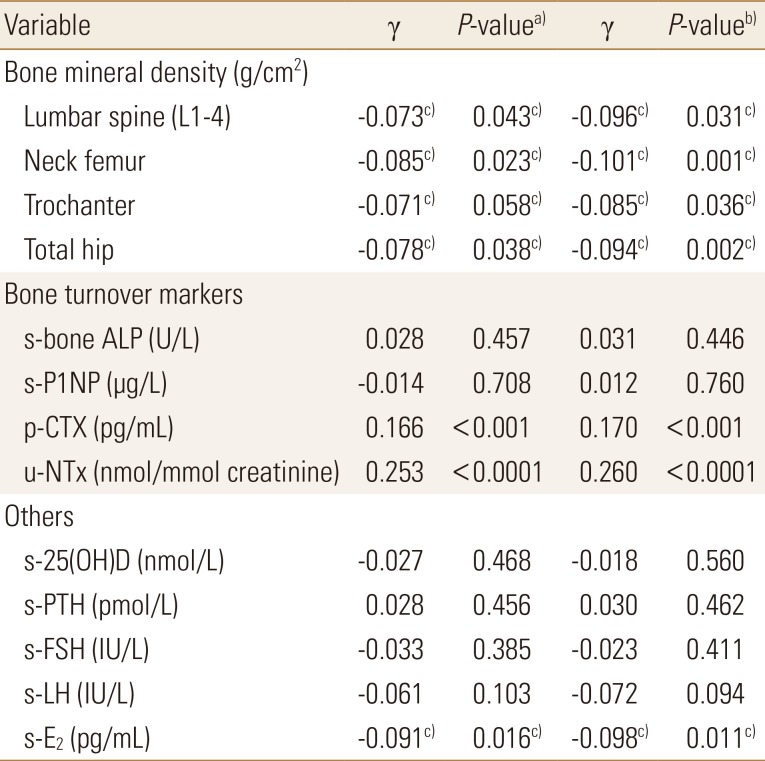
High plasma S1P levels were associated with increased incident fracture risk (Table 3). After adjusting for age and other potential confounders, the ORF risk for each increment increase of 1-SD of the S1P level was greater than 6-fold among postmenopausal women. Women in the highest Quartile (risk group) had an increased incident fracture risk, so the risk was more than 10-fold as high as the risk in the lower three Quartiles combined (reference group) (Table 3). Significant negative correlations were observed between the plasma S1P levels and BMD at different sites studied, and the adjustments for controlling factors strengthened the statistical significance (Table 4). When we included BMD in multivariate regression analyses, risk estimates were not significantly affected (Table 3). Figure 2 shows the cumulative incidence of fractures in the cohort according to the specific Quartile of the plasma S1P level.
3. Possible confounding variables
Circulating S1P levels were positively correlated with age (r=0.339; P<0.001), age at menopause (r=0.103; P=0.006), BMI (r=0.212; P<0.001), and years since menopause (r= 0.189 P<0.001). Furthermore, in the women of the present cohort, plasma S1P showed a significant positive correlation with BRMs: p-CTX (r=0.166; P<0.001) and urinary NTx (u-NTx) (r=0.253; P<0.001) (data not shown). Conversely, bone formation markers (BFMs) s-P1NP (r=−0.014; P=0.708) and s-bone ALP (r=0.028; P=0.457) were not associated with plasma S1P, respectively, before or after adjustment for covariates (Table 4).
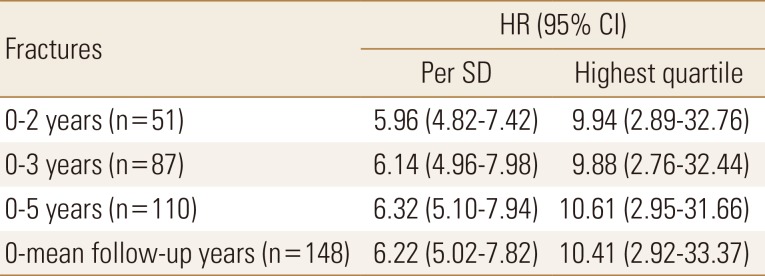
4. How long can plasma S1P predict fractures?
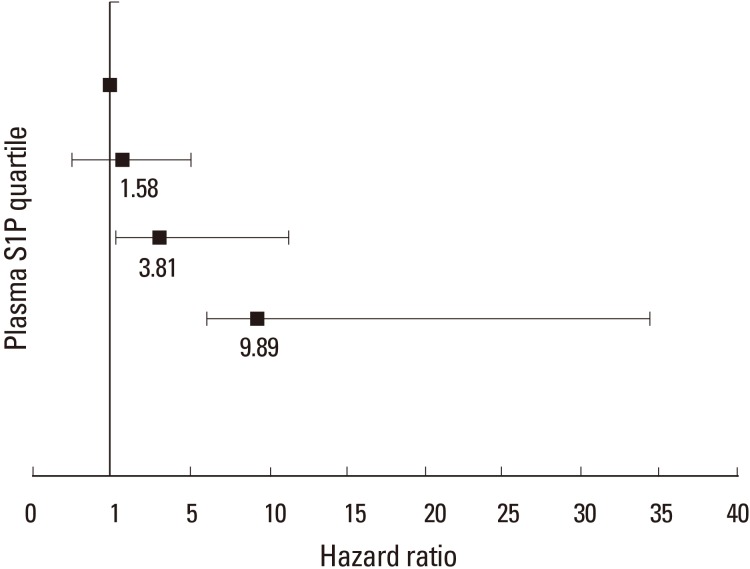
Circulating S1P levels could predict ORFs 1 year from the baseline visit with HR (95% CI, 6.36 [5.08−7.94]) for a 1-SD increase and 10.23 (2.87–34.46) for levels lower than the highest Quartile (data not shown). HRs for incident fracture prediction was of similar magnitude or slightly lower but remained significant when the follow-up was extended to 2, 3, and 5 years after enrollment (Table 5). There was no apparent increase in the risk of incident fractures in Quartile 2 as compared with quartile 1, but it became significant for Quartiles 3 and 4 (Fig. 3). There were positive significant correlations between plasma S1P levels measured at baseline visit and at 1 year (r=0.812; P<0.001), 2 years (r=0.851; P<0.001), 3 years (r=0.802; P<0.001), and 5 years (r=0.846; P<0.001), after the basal visit.
5. BTMs level in relation to fracture risk and the prediction of fractures
Baseline BRMs were associated with fracture risk: the HRs per SD for p-CTX, and u-NTx were 1.29, and 1.41, respectively (data not shown). These values persisted after adjustment for age and other potential covariates. When fracture risk was analyzed for Quartiles, women in the highest Quartiles of BRMs exhibited higher fracture risk. These values persisted following adjustment for age and other potential covariates (data not shown). However, BFMs s-P1NP and s-bone ALP were not associated with fracture risk either when analyzed per SD increase or in quartiles of the BFMs and none was able to predict incident fractures (data not shown). Plasma CTX, and u-NTx levels were able to predict ORFs 1 year from baseline visit with HRs (95% CIs, 1.28 [1.26−1.54]; 1.36 [1.08−1.50]) for 1-SD increase and 1.46 (1.10–1.97), and 1.38 (1.10–1.80) for levels lower than the highest quartiles, respectively (data not shown). The HRs for incident fractures prediction was of similar magnitude or slightly higher but remained significant when the follow-up period was extended to 2, 3, and 5 years (data not shown).
6. PAR
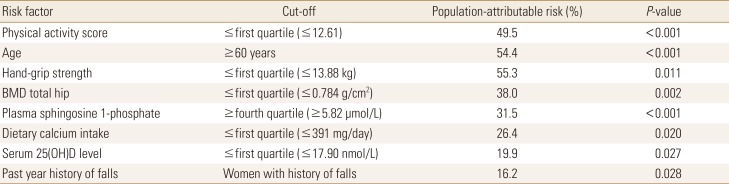
The incident fracture risk attributable to plasma S1P levels (in the highest Quartile) was estimated at 31.5%. The PAR for incident fracture independent risk factors among women studied is detailed in Table 6.
DISCUSSION
Our study is novel because it is the first longitudinal cohort being followed for 5.2±1.3 years with annual sampling and measurement of S1P as well as assessment of incident fractures at each visit. Thus, the fracture risk was not based on one measurement but on several determinations of the predictor plasma S1P. This study also includes a large number of patients (n=707), and both vertebral and non-vertebral fractures were assessed. This study is therefore more informative than that reported by Kim et al.[12], which used a cross-sectional sampling approach of 69 women with vertebral fractures only as a case-control study compared to 69 postmenopausal women without vertebral fractures and based on only one measurement of S1P.
In this study, we report a significant association between increased plasma S1P and incident fracture risk in a population of postmenopausal women followed prospectively for 5.2±1.3 years. We demonstrated that S1P levels were significantly higher with increasing number of incident fractures even after adjustment for possible confounders. A novel aspect of this study is an examination of the relationship between the risk of fracture and plasma S1P levels in postmenopausal women. The association was independent of the known risk factors for fragility fractures, including BMD, prior fractures, recent falls, smoking, low PA-score, and nutritional deficiencies, suggesting that plasma S1P could be a new potential biomarker of fracture risk independent of BMD in postmenopausal women.
Generally, plasma S1P levels in our cohort were similar to those reported for Korean postmenopausal women using the same assay method.[24] Our study is also consistent with the most recent report describing higher plasma S1P levels associated with a greater risk of vertebral fractures in Korean postmenopausal women (a case-control study of 69 women with vertebral fractures versus 69 women without fractures).[12] BRMs (p-CTX and u-NTx) were significantly associated with ORFs for the same follow-up period, with much lower HR values than those obtained for plasma S1P. No association was obtained for BFMs and fracture risk. Our observations of BTMs in relation to the prediction of ORFs are consistent with those of our recent study [5] and those of Ivaska and colleagues [25] and others [4].
In this study, the majority of women that were classified with high plasma S1P (remaining stable over the follow-up period) during one time interval were then classified with high plasma S1P 5.2±1.3 years later. This suggests that a single measurement of plasma S1P could be sufficient to identify women at high risk for ORFs. Thus, plasma S1P metabolism, clearance, and/or production were stable among the women studied. However, we did observe minor changes in the longitudinal plasma S1P levels. Such changes may be related to aging and not analytical variability because plasma S1P measurements were performed under standardized conditions using a validated assay. Plasma levels in women are influenced by age. We observed a positive association between S1P levels and age, confirming previous studies in Korean women.[24] The S1P production increases as women age, but decreased S1P production, clearance, and/or hormonal changes may also contribute to increases in S1P levels. Further work is needed in this regard. Other biological variability, such as diet, PA, and/or other lifestyle factors, cannot be excluded.
The estimated PAR of increased S1P levels was significant, and S1P levels in the highest quartile produced 31.5% of incident fractures. The PARs were lower than those for S1P compared with the well-known fracture risk factors, including low PA-score, low hand-grip strength, and low total hip BMD, among others [5] (Table 6). High S1P levels had an effect that was equal to or greater in magnitude to established ORF risk factors for this cohort.[526]
The mechanisms connecting S1P levels and incident fracture risk remain unclear. S1P mediates bone destruction by inducing the formation of osteoclasts.[927] A gradient exists for S1P in which it is more abundant in circulation than in the bone marrow.[2829] When the difference in S1P levels between these two compartments increases, osteoclast precursors are present in a limited amount in the bone marrow cavity, thus promoting bone resorption.[81011] Accordingly, bone resorption is promoted, and BMD decreases as the plasma levels of S1P become higher in the circulation,[24] resulting in higher fracture risk.[12] Additionally, increased plasma S1P levels may lead to enhanced osteoblast-dependent osteoclastogenesis, which is usually associated with bone loss.[9] Such mechanisms are consistent with our present observations whereby higher plasma S1P levels were only associated with BRMs (Table 4), and plasma S1P levels were negatively associated with BMD at various sites studied. It is possible that one and/or both mechanisms contribute to the effects of S1P on bone. However, because S1P levels within bone marrow plasma are lower than those in circulation, the S1P systemic mechanism is suggested to be more clinically important than the autocrine mechanism. It is interesting that in the present study plasma S1P levels were associated with the risk and number of ORFs, even after additional adjustment for BMD. Such observations could be interpreted by the potential effect of S1P on bone resorption. Thus, elevated osteoclastic activity among postmenopausal women with relatively higher bone resorption results in the deterioration of bone quality and microarchitecture that will contribute to higher risk for fracture out of proportion to the decreased bone mass.[30] It is possible that compromised bone strength by higher levels of S1P may have been mainly due to deteriorated bone quality rather than low bone mass and might contribute to an increased risk of incident fractures. Taken together, these observations provide evidence that S1P controls migratory trafficking of osteoclasts precursors, dynamically regulating bone mineral homeostasis, and possibly identifying a critical control point in osteoclastogenesis.[10]
The present study has several strengths. This is the first report demonstrating that high plasma S1P levels predict incident fractures in a large prospective population-based study. The study had a large sample size for which women were randomly selected from the local population using strict inclusion criteria. We obtained detailed lifestyle characteristics and BTM and BMD measurements along with a large number of fracture outcomes over a follow-up period of 5.2±1.3 years, plus multiple measurements of plasma S1P in relation to BTMs during annual visits. We standardized the sampling time after all of the participants fasted overnight in order to minimize pre-analytic variations due to circadian rhythm and/or food intake. Moreover, both platelets and mast cells can secrete S1P when activated by thrombin or IgE-bound antigen, respectively.[6] Such possible effects were minimized by our inclusion criteria that excluded women who may have had infectious or immune disorders during recruitment. However, neither platelets nor mast cells were shown to play a role in controlling S1P homeostasis in the blood.[31] Plasma S1P levels were measured using a commercially well-validated assay method and no significant differences were evident between basal mean plasma S1P levels and S1P levels in those who died during the follow-up period (data not shown).
The principal limitation of this study relates to the accuracy of self-reported data collection in relation to lifestyle information that may have been subject to report bias. During recruitment, women with osteoporosis were excluded from the study because we wanted to examine and treat fractures and bone loss in a cohort of healthy postmenopausal women. The effect that this exclusion may have had on the study results is unknown. Finally, the number of incident fractures is relatively low for calculating the HRs in relation to a given type of fracture.
The association between higher plasma S1P levels and ORF risk should be confirmed in other larger population studies. Proof of a causal relationship between elevated S1P levels and bone disease could be established by intervention studies that aim to lower plasma S1P levels. Indeed, it was previously demonstrated that treatment with FTY720 relieved ovariectomy-induced osteoporosis in mice by decreasing the number of mature osteoclasts that were attached to bone surfaces.[11] The mechanism of action of S1P is completely different from that of conventional therapies. Controlling the recruitment and migration of osteoclast precursors was suggested to represent a promising new therapeutic target in the treatment of bone disease,[8] including osteoporosis.
Finally, the current study could confirm the results of the previously published works of Kim et al.[32] and Bae et al.[33]. Our study could conclude that high S1P level is significantly associated with increased risk of incident fracture in postmenopausal women. Moreover, S1P in combination with BMD and biochemical markers of bone turnover could be used as a reliable predictors of the risk of incident fracture over a period extending up to 5.0 years duration.

 XML Download
XML Download