

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A smile is an important component of human facial expression. Improvement of smile is often the main motivation for patients seeking orthodontic treatment.1 Two types of smiles have been recognized: posed smile (non-enjoyment or social smile) and spontaneous smile (enjoyment or Duchenne smile). These two types of smiles differ in the involvement of the lips, cheeks, eyes, face, head, and shoulders.2
The spontaneous smile has been considered a person's authentic smile expression because of its unconscious nature.3 The importance of spontaneous smile in evaluating dentofacial esthetics has been highlighted in the literature. However, a spontaneous smile cannot last long,4 and is therefore difficult, time-consuming, and resource intensive to record.5 In contrast, posed smile, which is voluntary and not elicited by an emotion, is widely used as a routine record in esthetic-related treatments, including orthodontics, mainly because of its high reproducibility and convenience to be grasped on command.67 It can be a learned greeting or a signal of appeasement and can be sustained.
In smile analysis, most orthodontists primarily focus on the amount of incisal and gingival exposure, as well as the transverse dimension of the smile.8 However, the amount of dental and gingival exposure can be significantly influenced by the type of smile. Posed smile is usually smaller and therefore has less dental and gingival exposure. Thus, the severity of gummy smile and excessive buccal corridor in spontaneous smiles might be underestimated on the basis of the patients' photographs of posed smiles.
The smiles have also been found to differ between Eastern and Western cultures.910 In most Western countries, a big posed smile is considered a basic element of kindness and friendliness, whereas in many Eastern countries, like China, a smile without the teeth exposed is traditionally preferred. Some Chinese people still feel uncomfortable giving a posed smile. Many patients receiving orthodontic treatment at our hospital are yet unaware of how to give a posed smile; instead, they slightly open their lips to display the teeth when giving a posed smile. The use of the posed smile alone is not sufficient to accurately evaluate dental and gingival exposure, especially in Eastern people like the Chinese.
Compared to conventional photography, digital videography has been found to be a more reliable approach to evaluate smile and dental and gingival exposure.31112 This is because digital videography can capture and provide more information on maximum incisal exposure and buccal corridor than does photography.13 In addition, considering that a smile cycle proceeds in three stages: an initial attack period, a sustaining period, and a fade-out or decay period,4 a photograph acquired during the attack and decay periods, which have been found to occur, is not valid and reproducible and does not provide a reliable evaluation of dental and gingival exposure.13
The aim of the study was to use digital videography to assess the reproducibility of the autonomous maximal smile (AMS) for evaluating dental and gingival exposure. The AMS was defined as the broadest smile that a subject gives with maximum intercuspation.
MATERIALS AND METHODS
Subjects
A total of 100 subjects (34 men and 66 women) were included in the study; their mean age was 22.4 years (range, 20.0–24.8 years). They were all Chinese students from Sichuan University, Chengdu, China. A power analysis was performed before the study to determine the number of subjects required for this investigation.
The following exclusion criteria were strictly followed: (1) developmental or traumatic abnormalities of the face or facial muscle nerve injury; (2) previous esthetic or maxillofacial surgery; (3) missing teeth (except wisdom tooth) or erupted supernumerary teeth; (4) visible enamel defects, dental caries, or periodontal disease; (5) visible crooked, asymmetric, and rotated maxillary incisors or crossbite; and (6) invisible upper incisal edge or buccal corridor in posed smiles.
Each eligible subject signed a consent form granting us permission to acquire and use photographs, albeit without knowledge of the specific purpose of the research. The ethics approval was obtained from West China Hospital of Stomatology Ethics Committee (project number WCHSIRB-D-2014).
Videography
A Nikon D7100 camera (Nikon, Tokyo, Japan) with a 105-mm F/2.8 macro lens (Nikon) was mounted on a tripod. The height of the tripod was adjusted individually to accommodate for the different heights of the subjects. Only the mouth area of the subject was displayed to the photographer to minimize the potential influence of other facial features, such as the eyes and hair. The macro camera lens was manually focused to show a clear maxillary anterior dental view in each subject. The magnification scale was 1:6.
The subject was asked to relax the facial muscles by looking in a mirror before filming. The subject was seated at a natural head position, at a distance of 1 m from the camera. The video camera was turned on after the subject was seated stably. During the video recording, the subject was guided by two verbal directives. The first verbal directive was “keep your teeth closed, and give me a smile to show your teeth,” in order to give the posed smile. Thereafter, the subject was asked to “keep your teeth closed, and smile to both sides as wide as you can,” in order to give the AMS (Figure 1). The video clip of each subject lasted 15 to 20 seconds, and was recorded at the rate of 30 frames/second. A periodontal probe was used as a standard ruler to measure the width of the maxillary central incisor edges (Figure 2) for further measurement using a software. The same procedure was repeated for each subject in the same environment a total of three times at 1-week intervals.
Video editing
Raw digital video clips were transferred to a computer and converted into individual frames by using Sony Vegas (version 13.0; Sony, Tokyo, Japan). The frame of a posed smile was one of the 30 consecutive frames that barely changed. The frame of the AMS was identified by the broadest smile shown in the dynamic frames. The two selected frames for each subject were saved as TIFF files without compression.
Image measurement
All the images were opened and measured in Photoshop (version CC; Adobe, San Jose, CA, USA). Lip-teeth relationship width (LTRW) and buccal corridor width (BCW) were measured (Figure 3). LTRW was the amount of vertical distance between the inferior border of the vermilion and the edge of the maxillary central incisors. BCW was the sum of the horizontal distance from the most lateral aspect of the most posterior visible tooth to the inner commissure on both the left and right sides.
Statistical analysis
Two-way mixed intraclass correlation coefficients (ICCs) were used to assess the validity and reproducibility based on the findings of previous publications,141516 i.e., an ICC < 0.4 indicated poor reproducibility, 0.4 < ICC < 0.75 indicated fair-to-good reproducibility, and ICC > 0.75 indicated excellent reproducibility.
According to the Landis and Koch17 criteria, the number of repetitions of measurement necessary for the ICC level to become excellent beyond 0.75 was based on the Spearman-Brown formula16:

In the formula, m-value is the number of repetitions of measurement required, and r1 is 0.75.
A paired t-test was also performed to compare the means of LTRW and BCW between the posed smiles and AMS, and between the sexes. All statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA).
RESULTS
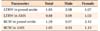
The reproducibility of the AMS was significantly higher than that of the posed smile (Tables 1 and 2). The ICCs of the posed smiles were 0.62 and 0.65 for LTRW and BCW, respectively, indicating fair-to-good reproducibility. The m-values of the posed smiles were 1.85 and 1.59 for LWRW and BCW, respectively. The ICCs of the AMS were 0.77 and 0.74 for LWRW and BCW, respectively, indicating excellent reproducibility. The m-values of the AMS were 0.88 and 1.05 for LTRW and BCW, respectively. Taken together, compared with the posed smile, the AMS had higher reproducibility and lower m-value.
Dental and gingival exposure of the AMS was significantly greater than that of the posed smile. LTRW of the AMS (9.34 ± 2.29 mm) was on average 1.41 mm larger than that of the posed smile (7.93 ± 1.99 mm) (p < 0.001), with one subject showing the largest difference of 5.36 mm. Among the subjects, 12.0% (12 of 100) showed a considerable increase of LTRW (the mean of three repetitions was over 3 mm) from the posed smile to the AMS (Figure 4A and 4B). BCW of the AMS (12.99 ± 3.39 mm) was on average 2.04 mm larger than that of the posed smile (10.95 ± 2.80 mm) (p < 0.001), with one subject showing the largest difference of 9.43 mm (Figure 5). Among the subjects, 10.0% (10 of 100) showed a considerable increase of BCW (the mean of three repetitions was over 5 mm) from the posed smile to the AMS (Figure 4C and 4D).
Considering the sex difference, men had bigger smiles than did the women, except for BCW of the posed smile. However, the difference was less than 1 mm, and no statistically significant difference was found (Figure 6). As to reproducibility, the ICCs and m-values for men and women are shown in Tables 1 and 2. Only the difference in BCW of the posed smiles showed a large margin of 0.17 for ICC (0.76 to 0.59), which was less than half the m-value (0.97 to 2.12).
DISCUSSION
The smile has been extensively studied, but few studies have investigated the validity and reproducibility of different types of smiles for evaluating dental and gingival exposure,311 and most of the studies have observed subjects from Western countries. In this study, we assessed the dental and gingival exposure of the posed smile and AMS, and found that the AMS displayed greater dental and gingival exposure, while having a significantly higher reproducibility, than did the posed smile. This indicated that the AMS could be an adjunctive or alternative approach for evaluating smile esthetics.
The reproducibility of posed smiles for evaluating dental and gingival exposure has been previously studied. Ackerman et al.18 analyzed five consecutive posed smiles in each of 10 subjects by using photography and reported that the ICCs for gingival and incisor exposure varied between 0.90 and 0.86. van der Geld et al.3 filmed the posed smiles of 20 subjects and measured the exposures of the maxillary central incisor and gingiva. They evaluated the reproducibility by using generalizability coefficients, which ranged from 0.99 for the anterior teeth to 0.80 for the posterior teeth, indicating excellent reproducibility. However, Mishima et al.5 used a video-based motion-analyzing system to determine the reproducibility of the posed smile in the Japanese population, and found that the ICC ranged from 0.71 to 0.83, and the minimum number of repeated measurements required for an ICC over 0.8 was two, suggesting that Eastern people may not give a posed smile with high reproducibility.
In the present study, the posed smile showed fair-to-good but not excellent reproducibility. Therefore, we recommend that, clinically, the posed smile should be captured twice by using duplicate procedures to get the average measurement to reach excellent reproducibility. The different reproducibility of the posed smiles between the Western and Eastern cultures is probably due to the cultural differences in sensitivity to the smile, the frequency of posed smiles during social interactions, and genetic variations. Individuals of some Eastern cultures, such as the Chinese, are reticent to show their own emotion in public, i.e., a warm smile with slight opening of the mouth is preferred over a broad smile in social interactions. Therefore, the amount of gingival exposure and buccal corridor may not be displayed adequately in Chinese patients, especially when diagnosing gummy smile. Such investigations will shed light on the roles of sociocultural and genetic factors in the analysis of smile esthetics.
An AMS is actually not a real “smile” but the opening of the mouth as broad as possible, with simultaneous elevation of the upper lip. It cannot please the observers because it is neither emotionally expressive nor socially communicative. However, compared to the posed smile, the AMS had a larger exposure of the teeth and gingiva as well as a larger BCW according to this study, which is probably closer to the situation of a spontaneous smile. Simultaneously, the AMS had higher reproducibility than did the posed smile, and the minimum number of repeated measurements required for an ICC level over 0.75 was just about one. This may be because the AMS does not rely on muscle memory, but instead, it relies on muscle limitation. In addition, the excessive gingival exposure could be caused by the hyperactive lip elevator muscles.19 This was observed in the current study in which 12.0% of the subjects with a considerable increase of LTRW from the posed smile to the AMS had hyperactive lip elevator muscles. Therefore, the AMS may have advantages over the posed smile in diagnosing excessive gingival exposure, especially in patients with hyperactive lip elevator muscles. In other words, since the spontaneous smile is important but hard to capture, the AMS may serve as an effective substitute because it is closer to the spontaneous smile in terms of dental and gingival exposure and is more reproducible than is the posed smile.
Studies have shown that sex can influence the smile, especially in adolescence. The upper-lip smile line was 1.5 mm higher in female subjects than in male subjects.2021 As for the reproducibility of the smile, men demonstrated a greater variation between maximal smiles.22 However, the influence of sex on smile faded when the age of the subject increased, with a limited influence on facial motion in normal adult men and women.23 This is consistent with the findings of our study. All subjects in the present study were adults, with a 2:1 sex ratio. No statistically significant difference in dental and gingival exposure was found between women and men in either the posed smiles or the AMS. However, the reproducibility of the AMS was higher than that of the posed smile for BCW measurements in the men included in this study.
Videography, which was used in the present study, has several advantages over photography. A significant difference in the objective comparison of smiles has been found between the dynamic videography and the static photography regarding the distance from the upper incisal edge to the upper lip of the vermilion.11 This may be because videography could capture more information on and dynamic movements of facial motions.
Buccal corridor space as well as dental and gingival exposure are two crucial parameters for evaluating smile esthetics. Buccal corridor space has been discussed in the literature and described by several investigators as undesirable.2425 Dental and gingival exposure is of great importance in diagnosis and treatment planning in clinical orthodontic settings; it is important for measuring accurately and reproducibly the distances between the lower margin of the vermilion and the edge of the incisors and the margin of the gingiva.26 The present study focused on the evaluation of the reproducibility of the AMS and the posed smile when measuring BCW and LTRW. More clinical parameters should be measured to strengthen the current conclusion and to provide more clinically relevant findings in the future.







 XML Download
XML Download