

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the increased interest in facial esthetics, facial asymmetry is one of the most common complaints of orthodontic patients, and thus, it is necessary to understand the underlying causes and aspects of facial asymmetry.
Facial asymmetry was known to be influenced more by the mandible than the maxilla12 and menton deviation has been reported to be the primary contributing factor in perceiving facial asymmetry.34 A previous study showed that mandibular asymmetry is influenced by a variety of factors including the condylar growth center, which directly or indirectly regulates the size of the condyle, and the length of the condylar neck.5 Moreover, persistently high condylar blood supply,6 condylar hyperplasia,7 fracture of the mandibular condyle,8 and internal derangement of the temporomandibular joint (TMJ)9 on one side influence facial asymmetry. However, these studies either used two-dimensional (2D) radiographic images5789 or were in vitro.6 Evaluation of the TMJ using 2D radiographic images has a number of limitations such as distortion, elongation, and superimposition of the TMJ onto other anatomic structures.
The advances in three-dimensional (3D) technology such as computed tomography (CT) have overcome the limitations of 2D radiographic images.1011 CT scan data can be used to assess linear and angular measurements after separating a necessary part such as the maxilla or mandible.121314 Moreover, evaluation of the TMJ using CT has been reported to show higher accuracy than that using 2D radiographic images.1516 For these reasons, CT data were used to evaluate the morphology of the normal TMJ,171819 the correlations between pathologic changes of the TMJ and facial asymmetry,2021 and TMJ morphology in facial asymmetry.222324 However, these studies used 2D rather than 3D measurements.
Few studies have reported comparisons of mandibular condyles between adults with and without facial asymmetry. Fraga et al.23 compared the anteroposterior position of the condyle in the mandibular fossa between individuals with normal occlusion and patients with Class I, Class II division 1, and Class III malocclusions. They reported that the greatest condylar decentralization was observed in the Class II group, whereas the least condylar decentralization was found in the normal occlusion group. Kim et al.25 investigated the condyle-fossa relationship in skeletal Class III malocclusion patients with and without asymmetry and found statistically significant bilateral differences in the axial condylar angles in the group with asymmetry, whereas there were no significant differences in the symmetry group. Kim et al.26 evaluated the volume and position of TMJ structures in patients with mandibular asymmetry and showed that the volume of the condyle on the smaller condyle side was significantly smaller in the asymmetry group than in the control group. However, these studies evaluated the mandibular condyle in facial asymmetry using only 2D measurements of the TMJ space2325 and axial condylar angles.25 Although Kim et al.26 performed a 3D evaluation of TMJ volume, they compared volumes between smaller and larger condyle sides, not between the deviated and non-deviated sides.
The purpose of the present study was to compare the 3D structure of mandibular condyles between adults with and without facial asymmetry and determine whether it influences menton deviation. The hypothesis was that the differences of condylar structure between deviated and non-deviated sides in facial asymmetry affect menton deviation.
MATERIALS AND METHODS
Study subjects
Institutional review board approval was granted by the committee of Chonnam National University Dental Hospital (No. CNUDH-2017-005). The present retrospective study included 60 adults, 30 (15 females and 15 males; mean age, 23.2 ± 3.8 years; 15 skeletal Class I and 15 skeletal Class III) in the asymmetry group and 30 (17 females and 13 males; mean age, 24.6 ± 3.2 years; 15 skeletal Class I and 15 skeletal Class III) in the symmetry group. The inclusion criteria were as follows: age, > 20 years; no orthodontic treatment; no orthognathic surgery; no prosthetic treatment for more than a single crown; no pathologic TMJ changes; no systematic arthritis; no facial trauma; no craniofacial anomaly; and frontal and lateral cephalograms and CT acquired for orthodontic diagnosis before treatment. Patients with skeletal Class II malocclusion, which is commonly caused by abnormalities of the mandible,27 were excluded.
Subjects were divided into two groups, symmetry and asymmetry, based on the amount of menton deviation,34 which is the angle between the line drawn from the anterior nasal spine (ANS) to the menton and the vertical reference line drawn from the crista galli to the ANS, on postero-anterior (PA) radiographs acquired before treatment. A menton deviation on PA radiographs exceeding 2° toward the left was considered to indicate asymmetry; menton deviation not exceeding 2° toward the right or left was considered to indicate symmetry.28 The asymmetry group consisted of subjects with menton deviation toward only the left side. Thus, the right side was the non-deviated side, and the left side was the deviated side in the asymmetry group.
Image acquisition and processing
CT scans were obtained with a CT scanner (Light Speed QX/i; GE Medical Systems, Milwaukee, WI, USA) under the following conditions: 2.5-mm slice thickness, 0.8-second scan time, 120 kV, 200 mA, slice pitch: 3, scanning matrix: 512 × 512 pixels, field of view: 180 mm, gantry angle: 0°. All patients were placed in the supine position with the Frankfort horizontal plane (FH plane) perpendicular to the ground, and the midline of the maxillary dental arch was adjusted to match the axis of the X-ray beam.
The Digital Imaging and Communication in Medicine data were reconstructed into 3D images using V-works software version 4.0 (CyberMed Inc., Seoul, Korea). Definitions of the landmarks are illustrated in Table 1. The 3D reference planes were constructed as reported in a previous study.29 The FH plane passed through the right and left porions and the right orbitale. The midsagittal reference plane (MSR plane) was the plane perpendicular to the FH plane passing through crista galli and opisthion. The anteroposterior reference plane (PO plane) was the plane perpendicular to the FH plane passing through right and left porions.
In order to ensure the precise identification of landmarks, the mandible was separated from the whole volume rendering image by removing overlapping areas using the sculpt functions of the V-works program. The separated mandible image was exported into a selection of demand (SOD) file. Moreover, for the accurate comparison of the volumetric measurements, the neck SOD file, which included the condylar process for the upper sigmoid notch, and the head SOD file, which included the upper part for the most contracted part of condylar neck, were separated from the mandible SOD file based on the FH plane (Figure 1).
Measurements
The mediolateral dimension was measured from the most medial point (Cdmed) to the most lateral point (Cdlat) of the condylar head, and the anteroposterior dimension was defined as the distance between the most anterior (Cdant) and posterior (Cdpost) points, which were points on the perpendicular line at the midpoint of the line drawn from Cdmed to Cdlat. The neck length was measured from the most superior point (Cdsup) of the condylar head to the sigmoid notch (S) of the mandible. The mediolateral condylar position was defined as the distance from Cdmed to the MSR plane. The condylar angles were measured in degrees between the condylar axis, which was the line drawn through Cdmed and Cdlat, and the FH plane, PO plane, or MSR plane, respectively. The volumes of neck and head were calculated automatically with the V-works program after demarcation of the area in 3D data (Figure 2).
All measurements were performed by a single operator. Twenty images were randomly selected and measurements were performed twice with a two-week interval to evaluate intra-observer reliability.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Co., Armonk, NY, USA). The reliability was assessed using the intraclass correlation coefficient (ICC); ICCs ranged from 0.982 to 0.999 for all variables, indicating excellent intra-observer reliability. The females and males were combined in each group because there were no statistical differences between them in either group. An independent t-test was used to compare the differences between the symmetry and asymmetry groups and the separate right-side and left-side measurements between the two groups. In order to identify the causes of menton deviation, the correlations between menton deviation and the right/left differences were analyzed using Pearson's correlation analysis.
RESULTS
The demographic characteristics of the subjects in each group, including sex, age, amount of menton deviation, ANB which is the angle between the line drawn from nasion to A point and the line drawn from nasion to B point, on lateral cephalograms, and SN-MP which is the angle between the line drawn from sella to nasion and the line drawn from menton to gonion, on lateral cephalograms are presented in Table 2; only menton deviation showed significant differences (p < 0.001) between the symmetry and asymmetry groups.
Comparison of the right/left differences of 3D measurements between the symmetry and asymmetry groups
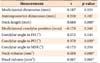
The right/left differences in mediolateral dimension and neck length differed significantly between the symmetry and asymmetry groups (p < 0.01). Comparisons of condylar position also showed significant right/left differences in the condylar angle to the PO plane and the condylar angle to the MSR plane between the two groups (p < 0.05). In the comparisons of volumetric differences, the neck and head volumes showed significant right/left differences between the two groups (p < 0.001 and p < 0.01, respectively). The mediolateral dimension, neck length, condylar angles to the PO and MSR planes, and neck and head volumes showed significantly larger right/left differences in the asymmetry group (Table 3).
Comparison of the 3D measurements of condyles between the two groups on the right and left sides separately
The 3D structures of the condyles on the right side, which was the non-deviated side in the asymmetry group, did not show significant differences between the symmetry and asymmetry groups. On the left side, which was the deviated side in the asymmetry group, the asymmetry group showed significantly smaller neck length and neck and head volumes than the symmetry group (p < 0.05; Table 4).
Correlations between the menton deviation and the right/left differences of 3D measurements in the asymmetry group
In the asymmetry group, menton deviation did not show a significant correlation with the right/left differences in mediolateral dimension or condylar angle to the MSR plane (p > 0.05), but showed a significant positive correlation with the right/left differences in neck length (r = 0.688, p < 0.001), condylar angle to the PO plane (r = 0.378, p < 0.05), the neck volume (r = 0.598, p < 0.001), and head volume (r = 0.567, p < 0.01; Table 5).
DISCUSSION
Each individual perceives the degree of facial asymmetry differently, and these perceptions can be affected by many factors. For instance, greater facial asymmetry is perceived when amount of menton deviation increases.4 Lee et al.3 evaluated the relationship between the PA cephalometric measurements and visual facial asymmetry and reported that menton deviation was the most affected landmark in perceptions of facial asymmetry. Ferguson28 assessed facial asymmetry using PA cephalograms and frontal photographs and found that facial asymmetry was perceived when the menton deviation from the midsagittal line was 2° or more. Menton deviation has been known to be an important indicator of facial asymmetry,34 and it influences both orthodontists' and patients' perceptions of facial asymmetry.3 Thus, it is necessary to understand the underlying causes of menton deviation in order to diagnose facial asymmetry and establish treatment plans.
Mandibular asymmetry is mediated by the condylar growth center,5 and is influenced by genetic and environmental factors. Moreover, mandibular asymmetry is a major cause of facial asymmetry.12 A number of studies have evaluated mandibular condyles in facial asymmetry,22232425 but they evaluated only the condyle-fossa relationship, not any 3D condylar structures. Although Kim et al.26 evaluated 3D condyle volumes, they compared volumes between smaller and larger condyle sides, not between deviated and non-deviated sides. Thus, the present study compared condyle morphology, position, and 3D volume between symmetry and asymmetry groups separately on the deviated and non-deviated sides.
When menton deviation, which is the primary contributing factor to perceive facial asymmetry,3 was more than 2°, facial asymmetry was in fact perceived in a previous report.28 In the present study, subjects were divided into two groups, the asymmetry group with menton deviation more than 2° and the symmetry group with menton deviation less than 2°. The menton deviation in the asymmetry group (5.7° ± 2.5°) differed significantly from that in the symmetry group (0.3° ± 1.3°). However, the ANB and SN-MP angles, which indicate anteroposterior and vertical growth of the mandible, did not show statistically significant differences between the two groups. In terms of the subjects' demographic characteristics, horizontal and vertical growth factors in skeletal structures did not show significant differences between the two groups, whereas only menton deviation showed a statistically significant difference (Table 2). Moreover, considering the changes in the mandibular condyles with age, only adult patients were included, and patients with TMJ arthritis, pathologic TMJ changes, craniofacial anomaly, or facial trauma were excluded. Patients with skeletal Class II malocclusion were also excluded due to the possibility of mandibular growth disorder.27
The mediolateral dimension, neck length, condylar angle to the PO plane, condylar angle to the MSR plane, neck volume, and head volume showed significantly larger right/left differences in the asymmetry group compared to the symmetry group (Table 3). However, comparison of the measurements between the two groups separately on the right and left sides did not show significant differences on the right side, the non-deviated side in the asymmetry group, whereas neck length, neck volume, and head volume showed significant differences on the left side, the deviated side in the asymmetry group (Table 4). These results indicate that in the asymmetry group, the right/left differences in neck length, neck volume, and head volume were caused by the condyles on the deviated side, whereas the right/left differences in mediolateral dimension, condylar angle to the PO plane, and condylar angle to the MSR plane were influenced by the condyles on both the deviated and non-deviated sides.
In addition, the neck was significantly shorter and the neck and head volumes were significantly smaller on the left side, i.e. the deviated side, in the asymmetry group (Table 4). Kim et al.26 also reported that the condyle volumes on the smaller condyle side were significantly smaller in their asymmetry group. These results indicate that the right/left differences in neck length, neck volume, and head volume in the asymmetry group were caused by smaller condyles on the deviated side.
The correlation analysis of menton deviation with the right/left differences in neck length, condylar angle to the PO plane, neck volume, and head volume in the asymmetry group showed significant positive correlations, indicating greater menton deviation with greater right/left differences in these measurements (Table 5). Thus, the right/left differences in neck length, condylar angle to the PO plane, and neck and head volumes need to be considered when evaluating menton deviation in facial asymmetry.
The present retrospective study has several limitations, including the use of the CT data taken in supine position. In supine position, the condyles might be placed more posteriorly which could affect condylar angles. Moreover, menton deviation, one of the contributing factors to facial asymmetry, is influenced by not only mandibular condyles but also mandibular fossa or body. Thus, future studies are needed that identify more correlations between facial asymmetry and mandibular body shape or the condyle-fossa relationship. In addition, the mandibular condyle and menton deviation can be affected by functional adaptation and the neuromuscular system. Although several studies found correlations between mandibular asymmetry and muscles and bone density,30 trabecular bone patterns,31 and occlusal force,32 they did not evaluate 3D structures of the mandible and TMJ. Thus, studies about the effects of soft tissue and function in TMJ are also needed.
Despite these limitations, this study found that the right/left differences of 3D measurements differed between individuals with and without facial asymmetry. Moreover, menton deviation was associated with the right/left differences caused by a smaller condyle on the deviated side, in particular differences in neck length, and neck and head volumes, in individuals with facial asymmetry. These results could help predict aspects of facial asymmetry in adolescents, as well as help understand the aspects of asymmetry in adults with facial asymmetry.






 XML Download
XML Download