

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the exact incidence of craniofacial clefts remains unknown, it is reported to be between 1.43 and 4.85 per 100,000 births.1 Using the orbit as the primary reference structure, Tessier classified craniofacial clefts into number 0 to 14 in a counterclockwise fashion which extends through the lips, nostrils, maxilla, eyelids, and eye brows.2
Tessier number 0 cleft involves the midline structures of the face.2 Although the etiology of Tessier number 0 cleft remains unclear, it is believed to result from the failure of fusion between the two medial nasal processes in the midline.3 Its typical phenotype includes a bifid nose deformity and a median cleft of the upper lip, with or without hypo- or hyper-telorism.3
Although several cases of Tessier number 0 cleft have been reported, these have documented surgical correction only.1,3,4 Surgical procedures for the correction of Tessier number 0 cleft vary according to the type of involvement.3 For false median clefts, which are characterized by the absence of tissue in the midline, including the prolabium, premaxilla, and nasal septum, it is better to delay corrective surgery up to 1–2 years of age because most patients with severe holoprosencephaly do not survive past this age. For true median clefts, reconstruction of Cupid's bow, philtrum, vermillion, and labial mucosa is necessary. In more severe cases where the nasal dorsum is affected and the nasal septum is duplicated, resection of the excess skin of the nasal dorsum and closure of the midline may be required. Correction of hypertelorism is delayed until approximately 8 years of age.
To the best of our knowledge, the concept of orthodontic and orthopedic treatment for patients with Tessier number 0 cleft, which is generally characterized by congenitally missing maxillary permanent incisors, a bony defect at the premaxilla, and maxillary hypoplasia, has not been reported till date. Therefore, the purpose of this case report was to introduce the concept of orthodontic and orthopedic treatment for a growing patient with Tessier number 0 cleft. This case report was reviewed and approved by the Institutional Review Board of School of Dentistry, Seoul National University (S-D20170007). Written informed consent was obtained from the patient because he was over 20 years of age.
DIAGNOSIS AND ETIOLOGY
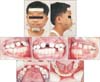
Patient (Figure 1)
A 5-year-old boy with Tessier number 0 cleft and right microphthalmia was referred to Department of Orthodontics, Seoul National University Dental Hospital from the Department of Plastic and Reconstructive Surgery, Seoul National University Hospital, Seoul, Korea.
Medical history
The patient was using an eye prosthesis for the right microphthalmia since 1 month of age (Figure 1). He underwent several surgical procedures at different ages as follows: cheiloplasty at 7 months, palatoplasty (V-Y push back method) at 1 year and 11 months, iliac bone grafting (IBG) at 7 years and 7 months, enucleation of the right microphthalmic eyeball and insertion of an orbital medpor implant at 8 years and 10 months, and several eyelid surgical procedures, including a frontalis sling, at 10 years and 1 month.
Clinical findings and diagnosis (Figures 2 and 3; Table 1)
The patient exhibited widening of the facial midline structures, including hypertelorism, a well-defined groove between the two alar domes, and an increased columellar width. Intraoral examination revealed an anterior openbite (overbite, −2.5 mm) and maxillary arch constriction.
A panoramic radiograph exhibited congenital missing of the maxillary primary and permanent central incisors, a bony defect at the premaxilla, and germination of the maxillary left primary incisor.
Cephalometric analysis showed retrusion of the maxilla and mandible (SNA, 76.3°; SNB, 74.8°; A to N per, −3.9 mm; Pog to N per, −10.0 mm), a normal ANB angle (1.5°), a high mandibular plane angle (FMA, 31.5°) and a large gonial angle (125.4°). The maxillary primary lateral incisor and mandibular primary central incisor were lingually inclined (primary U2 to SN, 89.7°; primary IMPA, 75.6°).
TREATMENT OBJECTIVES
The treatment objectives were as follows: reconstruction of the bony defect at the premaxilla using IBG and eruption guidance for the maxillary permanent lateral incisors into the graft area for substitution of the missing central incisors, correction of the maxillary hypoplasia through maxillary protraction, and establishment of normal overbite and overjet along with Class I canine and Class II molar relationships.
TREATMENT ALTERNATIVES
Stage 1. Management of the narrow maxillary arch, bony defect at the premaxilla, and congenitally missing maxillary permanent central incisors
Expansion of the maxillary arch using a fan-type expansion plate, IBG in the bony defect area, and eruption guidance for the maxillary permanent lateral incisors into the graft area were proposed. The patient and his parents accepted these treatment approaches.
Stage 2. Management of the maxillary hypoplasia
Three different treatment options were suggested to the patient and his parents: distraction osteogenesis of the maxilla for correction of the maxillary hypoplasia after IBG, growth observation and orthognathic surgery after growth completion, and maxillary protraction using a facemask during the pubertal growth period.
The patient and his parents refused treatment options 1 and 2. Although the possibility of orthognathic surgery or distraction osteogenesis after growth completion was explained to them, they chose facemask therapy for maxillary protraction during the adolescent phase.
Stage 3. Management of the remaining occlusal problems
The necessity for fixed orthodontic treatment to establish Class I canine and Class II molar relationships and normal overbite and overjet was explained. Although the possibility of extraction or orthognathic surgery was explained to the patient and his parents, they chose fixed orthodontic treatment with a non-extraction approach.
TREATMENT PROGRESS
Stage 1 (Figure 4 and Table 2)
Treatment was initiated with maxillary arch expansion using a fan-type expansion plate (slow expansion, 0.25 mm/week). At 7 years and 7 months of age, IBG was successfully performed. Subsequently, the maxillary permanent lateral incisors spontaneously erupted into the grafted area.
Stage 2 (Figures 5 and 6; Table 2)
Facemask therapy included a conventional facemask with tooth-born anchorage during the mixed dentition and early permanent dentition period and a facemask with skeletal anchorage after eruption of the entire permanent dentition.
The former was performed as follows.6 For transmission of the orthopedic force to the maxilla, a labiolingual arch, not a rapid palatal expansion appliance, was cemented because the patient had a surgically repaired hard palate cleft. Facemask therapy with a labiolingual arch (500 g/side, 30° downward and forward from the occlusal plane) was initiated at 8 years and 5 months of age and continued for 3 years and 6 months. The patient was instructed to wear the facemask for 12 to 14 hours/day.
At the time of eruption of the maxillary premolars, the labiolingual arch was removed and fixed orthodontic treatment was in initiated for alignment of the maxillary dentition. During this period, facemask therapy was temporarily discontinued.
To maximize the effects of maxillary protraction in the late adolescent period, facemask therapy with skeletal anchorage (facemask with miniplate [FM-MP]) was performed as follows.7,8 Two surgical miniplates (curvilinear type; Martin, Tuttlinger, Germany) were installed into the right and left zygomatic buttress areas of the maxilla at 15 years and 1 month of age. After 4 weeks, orthopedic forces (500 g/side, 30° downward and forward from the occlusal plane) were applied 12 to 14 hours/day. The FM-MP therapy was continued for 3 years and 5 months.
Stage 3 (Figure 7 and Table 2)
Fixed orthodontic treatment was initiated to align the mandibular dentition and establish stable occlusion with normal overbite and overjet at 19 years and 2 months of age and continued for 1 year and 10 months. After debonding (21 years and 0 month of age), fixed retainers were placed in the maxillary and mandibular arches, and a Hawley retainer was placed only in the maxillary arch.
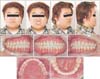
RESULTS
The total treatment duration was 15 years and 10 months. Class I canine and Class II molar relationships and normal overbite and overjet were achieved. Although the retrusive maxilla was significantly protracted by the long-term facemask therapy, the patient exhibited Class III profile because of continued mandibular growth. Reduction and setback genioplasty was recommended for correction of the chin prominence; however, the patient and his parents refused the procedure.
Cephalometric analysis showed a slightly retrusive maxilla (SNA, 79.1°; A to N per, −5.0 mm; horizontal distance from point A to VRP, 57.5 mm), a slightly protrusive mandible (SNB, 80.2°; Pog to N per, −7.2 mm; horizontal distance from Pog to VRP, 57.4 mm), a low ANB angle (−1.1°), a normal mandibular plane angle (FMA, 29.5°), a normal gonial angle (119.8°), normal inclination of the maxillary incisor (U2 to SN, 106.7°), and lingual inclination of the mandibular incisor (IMPA, 85.0°). Normal overjet and overbite were obtained (overbite, 1.7 mm; overjet, 1.9 mm) (Figures 8 and 9; Tables 3).
The treatment outcomes were well maintained after a follow-up period of 2 years (Figures 10 and 11; Tables 1 and 3).
DISCUSSION
We described a case of 5-year-old boy with Tessier number 0 cleft, who successfully underwent orthodontic and orthopedic treatment for resolving the skeletal and dental problems. Because there are no previous studies on the cephalometric evaluation of patients with Tessier number 0 cleft, it is difficult to understand the effects of growth and facemask therapy for maxillary protraction in this patient. Therefore, we consider it necessary to indirectly compare the cephalometric parameters of the present case with those of oral cleft patients from previous studies.
Initial growth pattern of the present case (Table 1)
At the initial visit, the patient exhibited a retrusive maxilla (SNA, 76.3°; A to N per, −3.9 mm; horizontal distance from point A to VRP, 50.1 mm), a high mandibular plane angle (FMA, 31.5°), and a large gonial angle (125.4°). These findings are similar with the initial growth pattern observed before secondary alveolar bone grafting (ABG) in a study by Seo et al.,9 who reported that the unilateral cleft lip and palate (UCLP) and cleft palate only groups exhibited a more retrusive maxilla and a more hyperdivergent pattern compared with unilateral cleft lip and alveolus group. In other words, because the cleft in this patient involved both the primary and secondary palate, the possibility of a retrusive maxilla and hyperdivergent pattern could have increased.
Bone grafting in the bony defect area and monitoring of tooth eruption
After IBG, the maxillary permanent lateral incisors spontaneously erupted into the grafted area (Figures 4 and 5). This result was similar with those of Enemark et al.10 and De Riu et al.,11 who reported 80% probability of spontaneous eruption of the maxillary canine when IBG is performed before its eruption. Schultze-Mosgau et al.12 suggested that controlled eruption of a tooth into the grafted area or orthodontic closure of the cleft gap might decrease the resorption of the grafted bone compared with orthodontic opening of the cleft gap. Therefore, in our patient, the missing maxillary central incisors were substituted by the maxillary lateral incisors, and the remaining space after eruption of the lateral incisors was subsequently closed by fixed orthodontic treatment.
Superimposition of lateral cephalograms obtained at different stages (Figure 12; Tables 1 to 3)
Changes between stage 0 (initial) and stage 1 (3 months after IBG)
Both the maxilla and mandible appeared to grow downward and forward (ΔSNA, 2.0°; ΔA to N per, 0.5 mm; Δhorizontal distance from point A to VRP, 2.0 mm; Δvertical distance from point A to HRP, 1.6 mm; ΔSNB, 3.5°; ΔPog to N per, 3.9 mm; Δhorizontal distance from Pog to VRP, 6.4 mm; Δvertical distance from Pog to HRP, 2.7 mm). However, the amount of forward growth of the mandible was greater than that of the maxilla, probably because of the post-surgical scar tissue in the upper lip and palate.
Changes between stage 1 (3 months after IBG) and stage 2 (mid-term use of FM-MP)
Susami et al.13 reported that, although conventional FM therapy with tooth-borne anchorage was effective for maxillary protraction in patients with UCLP, its effects were highly variable. Baek et al.7 and Ahn et al.8 suggested that the FM-MP therapy might be an effective alternative treatment modality with minimal unwanted side effects in cleft patients with maxillary hypoplasia. Therefore, sequential facemask therapy with conventional and skeletal anchorage methods was applied to this patient.
Facemask therapy resulted in maxillary protraction (ΔSNA, 1.1°; ΔA to N per, −1.8 mm; Δhorizontal distance from point A to VRP, 5.6 mm; Δvertical distance from point A to HRP, 7.7 mm) and labioversion of the maxillary incisors (ΔU2 to SN, 6.6°). However, significant mandibular growth was observed (ΔSNB, 1.1°; ΔPog to N per, −4.0 mm; Δhorizontal distance from Pog to VRP, 5.9 mm; Δvertical distance from Pog to HRP, 20.1 mm), with counterclockwise rotation of the mandible (ΔFMA, −1.7°) and a decrease in the gonial angle (−6.5°).
There are several aspects to be considered with regard to this phase of treatment. First, despite facemask therapy, forward growth of the maxilla was lesser than expected, probably because of the scar tissue caused by cheiloplasty, palatoplasty and IBG. Seo et al.14 reported that secondary ABG resulted in decreased forward growth of the maxilla in patients with unilateral and bilateral cleft lip and palate. However, when considering significant forward growth of the nasion point (Figure 12), the actual amount of forward growth of the maxilla induced by facemask therapy may be more significant than the changes in SNA and A to N per (Δhorizontal distance from point A to VRP, 5.6 mm vs. ΔSNA, 1.1° and ΔA to N per, −1.8 mm). Second, the amount of downward growth of the mandible was larger than that of forward growth despite counterclockwise rotation. These phenomena were helpful in correction of the anterior crossbite and anterior openbite. Third, although the space for congenitally missing maxillary permanent central incisors was completely closed by fixed orthodontic treatment, labioversion of the maxillary lateral incisors (ΔU2 to SN, 6.6°) also helped in correction of the anterior crossbite.
Changes between stage 2 (mid-term use of FM-MP) and stage 3 (debonding)
Slight posterior movement of the maxilla was observed (ΔSNA, −0.3°; ΔA to N per, 0.2 mm; Δhorizontal distance from point A to VRP, −0.2 mm). However, slight counterclockwise rotation of the mandible (ΔFMA, −0.8°) resulted in its forward movement (ΔSNB, 0.8°; ΔPog to N per, 2.8 mm; Δhorizontal distance from Pog to VRP, 2.2 mm). Although downward growth of the maxilla was limited (Δvertical distance from point A to HRP, 0.4 mm), the mandible showed downward growth (Δvertical distance from Pog to HRP, 4.2 mm).
Changes during the entire treatment period
Although facemask therapy resulted in significant downward and forward growth of the maxilla (ΔSNA, 2.8°; Δhorizontal distance from point A to VRP, 7.4 mm; Δvertical distance from point A to HRP, 9.7 mm), the mandible also exhibited significant forward growth with counterclockwise rotation and a decrease in the gonial angle (ΔSNB, 5.4°; ΔPog to N per, 2.8 mm; Δhorizontal distance from Pog to VRP, 14.5 mm; Δvertical distance from point A to HRP, 27.0 mm; ΔFMA, −2.0°; Δgonial angle, −5.6°). Eventually, a decrease in ANB was observed (ΔANB, −2.6°). Although the maxillary and mandibular incisors were both labially inclined (ΔU2 to SN, 17.1°; ΔIMPA, 9.3°), differences in the amount of labioversion between them helped in correction of the anterior crossbite.
CONCLUSION
• The findings from this case suggest that interdisciplinary and customized approaches are mandatory for successful management of maxillary hypoplasia, bony defect, and dental problems in Tessier number 0 cleft.
• Moreover, considering the potential of orthognathic surgery or distraction osteogenesis, meticulous monitoring of mandibular growth until growth completion is important.













 XML Download
XML Download