

 PDF
PDF ePub
ePub Citation
Citation Print
Print



The mortality rate in non-cardiac surgery is 1.5%, and 42% of cases are associated with cardiac complications [12]. The incidence rate of cardiac arrest during general anesthesia is 1.1–25.5/10,000 [345678]. Since patients at high risk of cardiovascular complications can be identified through preoperative risk stratification, intraoperative cardiac complication such as blood loss, anaphylaxis, or other complications can be anticipated [9]. Major cardiac complications such as myocardial infarction (MI) often occur in patients with risk factors after high-risk surgery, but can also occur unexpectedly in patients without risk factors.
We report a case of cardiac arrest due to an unexpected acute MI in a patient without risk factors during intermediate-risk head and neck reconstructive surgery.
CASE REPORT
A 55-year-old male, non-smoker with hypertension, with American Society of Anesthesiologists class II physical status and body mass index (BMI, height 177 cm, weight 87 kg) 27.8, was admitted for surgery for recurrent squamous cell carcinoma (SCC) of the right lip, maxilla, and buccal mucosa. The patient was initially diagnosed 10 years prior at a different hospital and underwent right maxillectomy, followed by additional mass resection at our dental hospital 2 years prior due to recurrence. The patient had another recurrence and was planned to undergo mass resection, partial maxillectomy, selective neck dissection (right level I, II, III), and reconstruction with anterolateral thigh free flap. He was on lercanidipine and atorvastatin (without aspirin). We performed surgery without additional cardiac evaluation, as the patient was relatively young, with estimated functional capacity > 4 metabolic equivalents (METs).
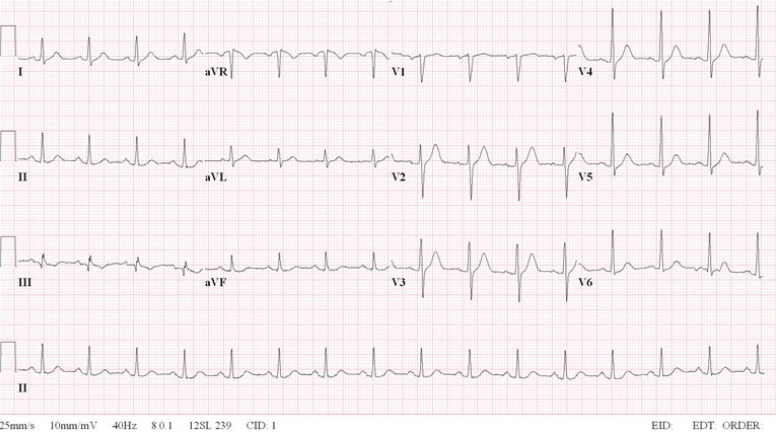
The preoperative electrocardiogram (ECG) was normal (Figure 1). Chest X-ray was unremarkable. Preoperative hemoglobin (Hb) and hematocrit (Hct) were 16.6 g/dL and 46.9%, respectively. Other preoperative laboratory findings were within normal range except alanine aminotransferase (44 IU/L). He had no premedication for general anesthesia.
The process after induction of general anesthesia is outlined in Figure 2. Anesthesia was induced after establishing routine patient monitoring (pulse oximetry, end-tidal CO2, ECG lead II with continuous ST-segment analysis, and noninvasive blood pressure monitoring) and bispectral index. His blood pressure (BP) was 155/89 mmHg, heart rate (HR) was 112 beats/min, body temperature was 36.1℃ and pulse oximetry oxygen saturation (SpO2) was 98%. After sufficient preoxygenation, anesthesia was induced with thiopental sodium (350 mg) and cisatracurium (16 mg). Nasotracheal intubation with an endotracheal tube (RAE cuffed, 7.0 mm) was performed without difficulty. Anesthesia was maintained with an O2/air mixture and adjusted for desflurane (5–7%). The patient was maintained on volume controlled mechanical ventilation with a mean arterial pressure 60–80 mmHg and normal and regular heart rate. Additional cisatracurium (2 mg) was administered as needed. The tidal volume was 6–8 ml/kg, and positive end expiratory pressure (5 cmH2O) was utilized. The respiratory rate was adjusted to maintain partial pressure of end-tidal CO2 at 30–35 mmHg. Invasive BP monitoring and arterial blood gas analysis (ABGA) were performed with the catheter in the right dorsalis pedis artery. Because Post-induction HR level was maintained above 100, esmolol 30 mg and fentanyl 50 µg were administered, and then HR level decreased to below 100.
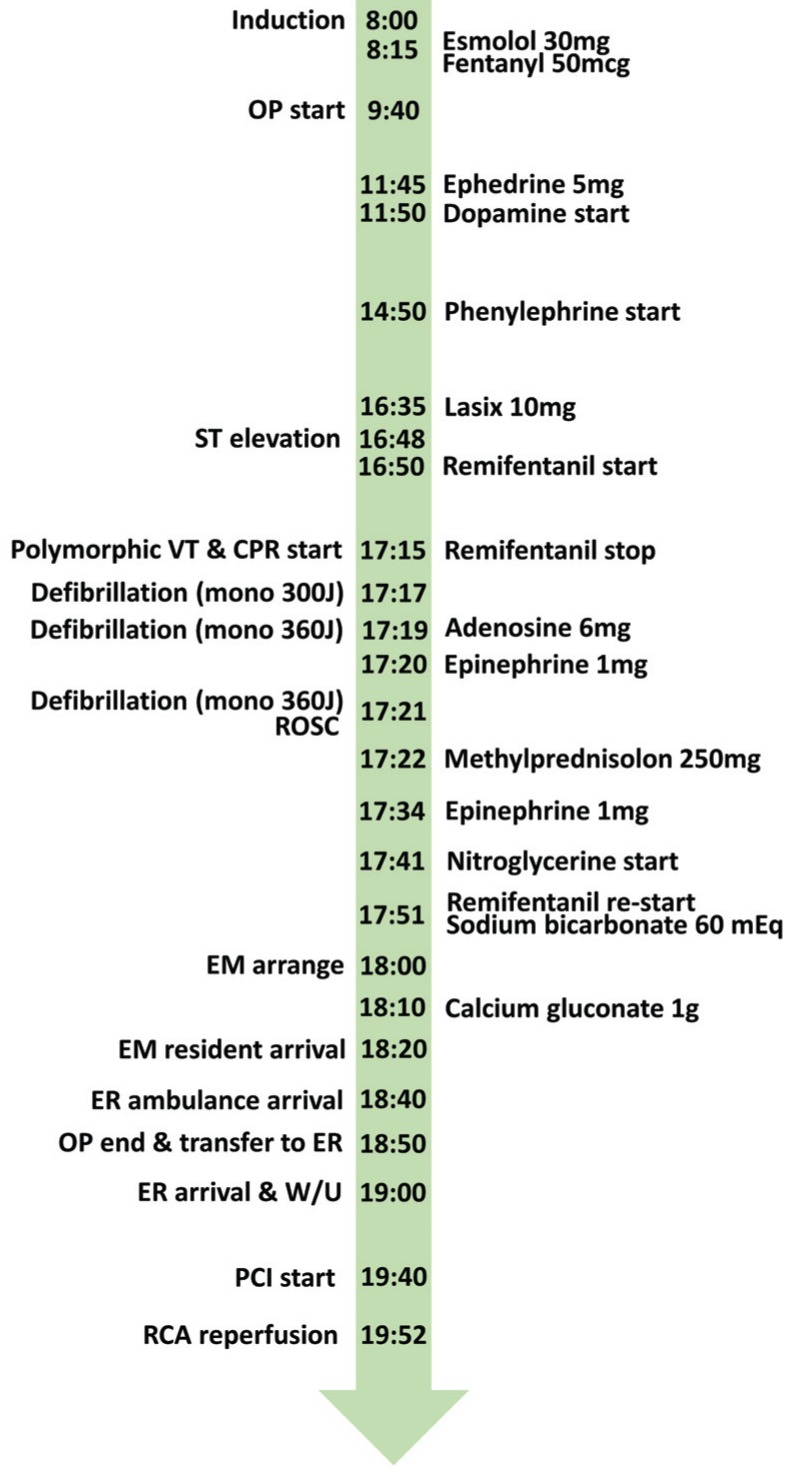
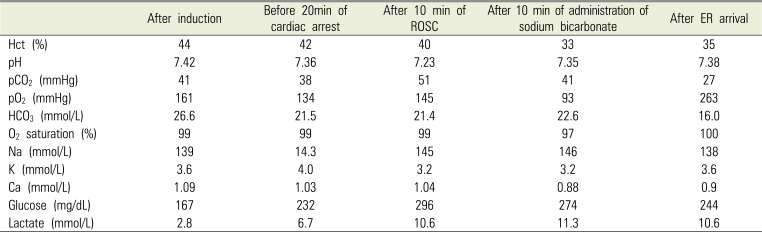
Surgery was uneventful. We started dopamine (3–6 µg/kg/min) injection 4 h after anesthesia induction to maintain BP. At 7 h after anesthesia induction, the HR was above 100 and BP was unstable, even after 4 L of crystalloid saline infusion (urine output 500 ml, blood loss 300 ml), and we started phenylephrine (0.5 µg/kg/min). When mass excision was completed and anterolateral thigh harvesting of a free flap was started, the ST segment was elevated by 4 mm and then decreased to 2 mm. BP was 132/72 mmHg and HR was above 100. We started remifentanil 1 ng/ml using a target-controlled infusion system (Orchestra Base Primea, Fresinius Kabi, Bad Homburg, Germay) and HR decreased to 60 without change in BP (Figure 3). Body temperature was 37.4℃. ABGA results at 20 min before cardiopulmonary resuscitation (CPR) are shown in Table 1. After about 30 min of ST segment elevation, the ECG changed from sinus rhythm to ventricular fibrillation, and a pulse was not palpable (Figure 4A). Saturation prior to cardiac arrest was above 98%. We commenced CPR and stopped remifentanil. After defibrillation (monophasic 300 J) we injected adenosine 6 mg, followed by 2nd defibrillation (360 J) and epinephrine 1 mg. After 3rd defibrillation (360 J), we observed return of spontaneous circulation (ROSC) (Figure 3). After ROSC, we injected methylprednisolone 250 mg. However, BP was reduced and we repeated epinephrine 1 mg and increased dopamine dosage to 15 µg/kg/min. Tachycardia persisted with elevated ST segment (Figure 4B). With suspected ST elevation MI, we started nitroglycerine at 1 µg/kg/min and remifentanil 1 ng/ml using a target-controlled infusion system. We discontinued the operation and started primary wound closure. ABGA results after ROSC showed acidosis, and sodium bicarbonate 60 mEq was injected. ABGA results after 10 min showed improvement in acidosis but reduced ionized calcium, and we injected calcium gluconate 1 g (Table 1). We arranged transfer to a hospital where percutaneous coronary intervention (PCI) was available. While being transported, the patient was intubated but had spontaneous respiration, was fully conscious, and had no neurological symptoms. BP was 111/52 mmHg, HR was 55 beats/min, body temperature was 37.3℃, and SpO2 was 97%. Laboratory tests in the ER showed creatine kinase MB (CKMB) 34.5 ng/mL (reference: < 6.6 ng/mL), troponin I 0.35 ng/mL (reference: < 0.028 ng/mL), Hb 11.9 g/dL, and Hct 35%. The ECG showed ST elevation in II, III, aVF, V4, 5, and 6 and ST depression in I, aVL, and V3 leads (Figure 5). Cardiac catheterization revealed single-vessel disease. The left coronary artery (LCA) was intact but the middle portion of the right coronary artery (RCA) was totally occluded with thrombus (Figure 6A, 6B). Red thrombus was removed with suction and wiring to the distal RCA was successfully performed (Figure 6C). After reperfusion, balloon dilatation and stent insertion were performed (Figure 6C, 6D). The patient was admitted to intensive care and aspirin 100 mg and clopidogrel 75 mg was started. After PCI, an echocardiogram showed “normal left ventricle cavity size and systolic function; calculated ejection fraction 56%; RCA territory ischemic insult; akinesia of basal, mid, apical inferior wall; trivial tricuspid regurgitation; dilated left atrium cavity; no other pathological changes”. The patient showed clinical improvement with progressive normalization of cardiac enzymes and after 7 days was transferred to the Maxillofacial Surgery ward of our dental hospital without complications. However, he still required anticoagulation and conservative treatment pending further reconstructive surgery in 6 months.

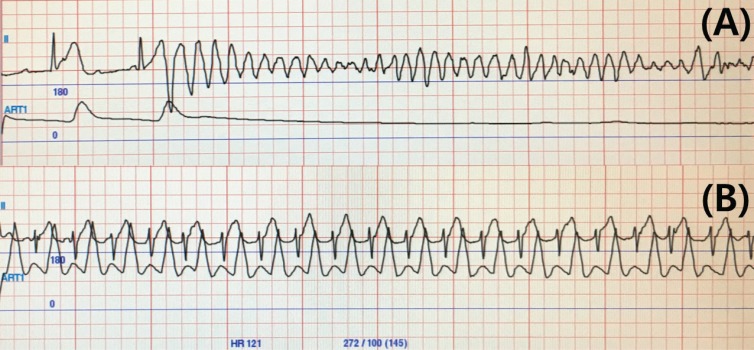 | Fig. 4Changes in lead II on electrocardiogram and arterial blood pressure during anesthesia. (A) Cardiac arrest; ventricular fibrillation, (B) Sinus tachycardia with ST segment elevation.
|
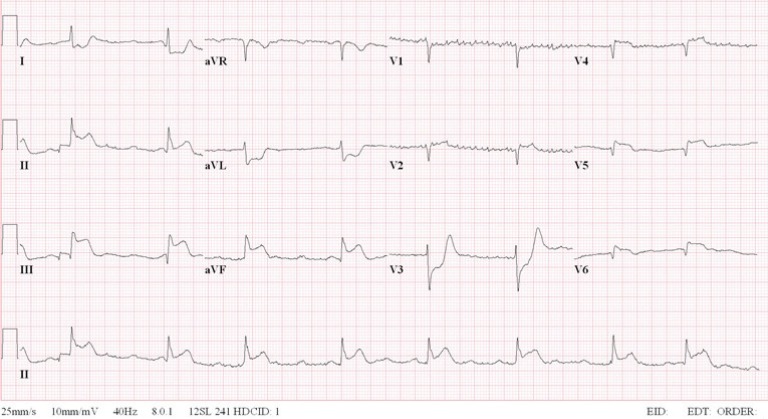 | Fig. 5Postoperative electrocardiogram in the emergency room (heart rate 51, QRS 88 ms, QT/QTc 418/385 ms).
|
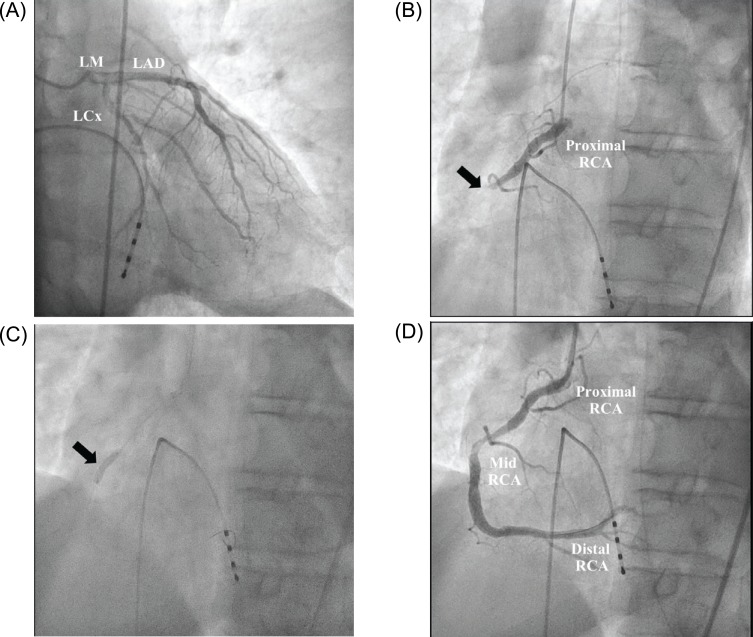 | Fig. 6Coronary angiography and percutaneous coronary intervention. (A) Normal left coronary angiography (RAO 7.1 CAU 28.9), (B) Angiography showing complete luminal occlusion of the mid RCA (arrow) (LAO 29.4, CAU 0.6), (C) Successful wiring to distal RCA and ballooning (arrow) (LAO 32.1, CAU 0.5), (D) After percutaneous coronary intervention, the stent placed at mid RCA showing good final result (LAO 32.1, CAU 0.5). CAU = caudal; LAO = left anterior oblique; LCA = left coronary artery; RAO = right anterior oblique; RCA = right coronary artery.
|
Table 1
Arterial blood gas analysis of the patient during anesthesia
![]()
Go to : 
DISCUSSION
The first manifestation of coronary artery disease in 60–70% of patients is sudden death or MI [10]. A retrospective study of 193 patients who underwent head and neck reconstructive surgery showed a 3.6% incidence rate of postoperative MI [11]. We found 4 case reports of patients who received free flap surgery and had cardiac arrest. A breast cancer patient experienced cardiac arrest due to tamponade during reconstructive surgery, but recovered [12]. Another patient experienced cardiac arrest due to hypokalemia during surgery for tongue cancer, and completed reconstructive surgery after recovering from cardiac arrest [13]. Another patient died after an undetected arrhythmogenic right ventricle cardiomyopathy after reconstructive surgery for maxillary SCC [14]. A fourth case had sudden cardiac death after reconstructive surgery for a diabetic foot; postoperative MI caused severe left ventricular dysfunction with ventricular fibrillation [15]. However, no previous case report described cardiac arrest due to an acute MI during free-flap surgery.
MI is defined as an irreversible necrotic state of myocardium. Key causes include coronary artery occlusion or spasm. Occlusion of the RCA may cause infarction of the inferior wall of the left ventricle with or without right ventricular (RV) myocardial infarction (MI), manifested as ST-segment elevations in leads II, III, and aVF. Anterior ST elevation due to occlusion of an RCA branch may be a mirror image of RV ischemia [1617].
Perioperative acute MI is a major cause of morbidity and mortality in non-cardiac surgical patients. Poor preoperative cardiac condition, new intra-operative ST-T changes, intra- and postoperative hypotension, and increased intraoperative blood loss and transfusion are risk factors for perioperative acute MI [18]. Our patient exhibited no other cardiovascular risk factors aside from hypertension and being overweight, and had no preoperative evaluation that could anticipate acute MI.
Surgical interventions can be divided into low, intermediate, and high cardiac risk, and 30-day cardiac event rates are 1%, 1–5%, and 5% respectively [2]. The revised cardiac risk index [1920] is commonly used, and includes high risk surgery, ischemic heart disease, prior heart failure, stroke or transient ischemic attack, preoperative insulin therapy, and creatinine level > 2 mg/dl. Our case had no components of the revised cardiac risk index. The patient had no preoperative abnormalities and was relatively young.
Acute MI during general anesthesia is difficult to diagnose. The patient cannot report chest pain, and changes in vital signs may not be noticeable or easily differentiated from surgical factors. However, ischemia can be detected with ECG changes [21], which were observed in our case prior to cardiac arrest. Unfortunately, the anesthesiologist overlooked ST-segment elevation. Nonetheless, there may be no changes on the ECG. Furthermore, the leads that reflect ECG changes may vary, based on the ischemic location. Since only II and/or V5 are monitored under general anesthesia, diagnosing an MI can be difficult [22].
The diagnosis of acute MI is based on clinical symptoms, myocardial biomarkers (CKMB, troponin), ECG indicators, or changes on an echocardiogram [23]. In suspected acute MI in a patient undergoing surgery under general anesthesia, rapid diagnosis and treatment is crucial. If necessary, immediate discontinuation of surgery, rapid cardiac work-up, and PCI are crucial for survival. We suspected an acute MI after ROSC and arranged transfer to a hospital where PCI was available. Quick decision making and transfer allowed the patient to receive RCA reperfusion through PCI after ROSC within 140 min. The patient recovered without further complications.
Based on advanced cardiovascular life support guidelines (2015), adenosine injection and 1st defibrillation using 300 J during CPR in our case were part that need improvement [24]. Adenosine injection was recently deleted from guidelines, and defibrillation should start with 360 J.
In conclusion, diagnosis of acute MI in patients who cannot report chest pain due to general anesthesia is difficult, more so in patients without risk factors, making careful observation of ECG changes necessary. If an acute MI is suspected, quick decision making is required for rapid diagnosis and treatment to increase the chance of survival.
Go to :
 XML Download
XML Download