

 PDF
PDF ePub
ePub Citation
Citation Print
Print


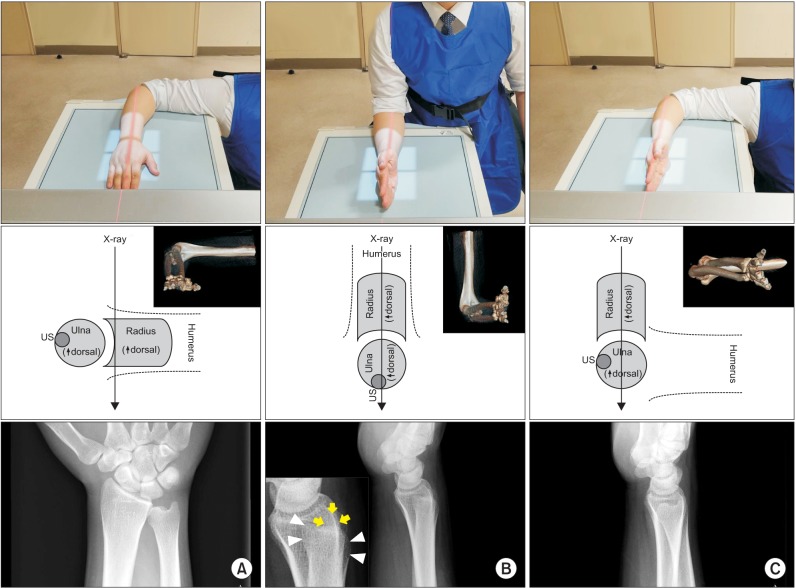
The location of the ulnar styloid process can be confusing because the radius rotates around the ulna. Anatomical structures of the wrist are usually perceived in relation to the hand, which rotates along with the radius. The ulnar styloid process is easily thought to be in a certain position in the wrist, but in fact this can only be applied when the forearm is fixed in a certain rotational position. In other words, the ulnar styloid process may be located either volar or dorsal to the hand when the forearm is pronated or supinated.
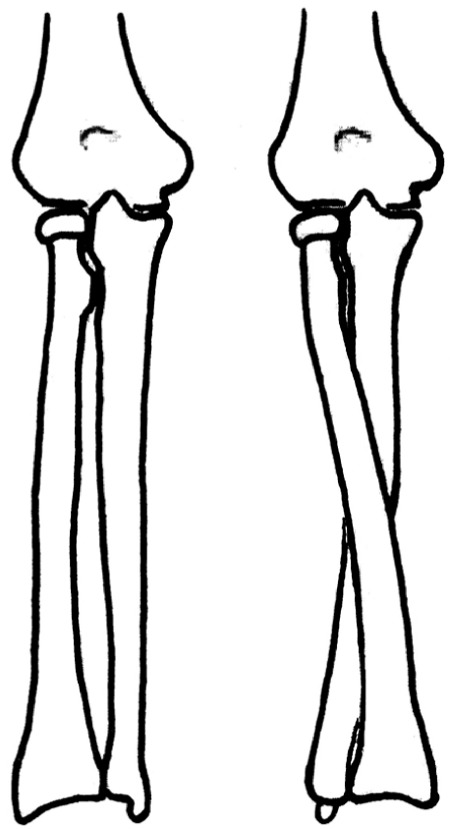
The evidence that the location of the ulnar styloid is confusing is that we often see illustrations of forearm pronation and supination (Fig. 1) where the ulnar styloid is drawn in different locations in the distal ulna despite the same position of the proximal ulna. Certainly, this is impossible unless the ulna can be twisted like a rubber rod. The location of the ulnar styloid tends to be thought in relation to the hand; however, in fact it is fixed in a certain location of the ulna, which is independent of the position of the hand. There will be no more of such misleading illustrations if we establish the absolute location of the ulnar styloid process and take into consideration that the radius and the hand move around the ulna.
In addition, we have found discrepant locations of the ulnar styloid process on lateral radiographs of the wrist in practice, suggesting that wrist radiographs are obtained in different positions of forearm rotation. Also, we commonly see wrist radiographs where the ulnar styloid process is in the same location on posteroanterior (PA) and lateral views (Fig. 2) taken from the same neutrally-rotated wrist with X-ray beams angled at 90°. This indicates that the PA and lateral views are not taken with the same forearm rotation, and thus they should not be compared directly for parameters influenced by forearm rotation. However, such radiographs are commonly seen even in scientific articles, including papers on ulnar variance that varies according to forearm rotation.123)
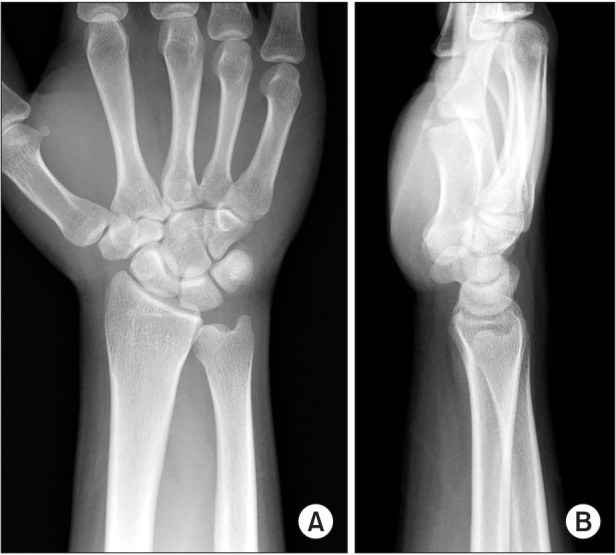 | Fig. 2Posteroanterior and lateral radiographs of the wrist commonly seen in practice. Note the ulnar styloid process is in the same location on the posteroanterior (A) and lateral (B) views. This is not realistic assuming that the two radiographs are taken from the same neutrally-rotated wrist with X-ray beams angled at 90°.
|
A standard lateral radiograph of the wrist should be obtained with the forearm in neutral rotation. There have been reports that the relative positions of the carpal bones can be the reference of pronation and supination on lateral radiographs of the wrist.45) However, such hand-based parameters can reflect only whether the hand is pronated or supinated to the X-ray beam and does not reflect forearm rotation. In other words, they can be controlled in wrist lateral views as with forearm pronation or supination. On the other hand, an ulnar structure such as the ulnar styloid process can be used as a reference of forearm rotation on lateral radiographs of the wrist because the radius rotates around the ulna. However, a scientific method for verification of neutral forearm rotation on lateral radiographs using the ulnar styloid process has not been reported yet because there have been no reports on the absolute location of the ulnar styloid process.
The establishment of the absolute location of the ulnar styloid process, which is independent of forearm rotation, will not only add to our knowledge on anatomy but also be applied in practice and scientific research. Determining whether a wrist lateral radiograph is taken with neutral forearm rotation is one of such applications. The purpose of this study was to identify the absolute location of the ulnar styloid process to use it as a reference for neutral forearm rotation on lateral radiographs of the wrist.
METHODS
We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea (IRB No. KC17RISI0042). The need for informed consent was waived. Three-dimensional computed tomography (3D CT) images of 23 forearms in 23 patients aged 18 years or older were analyzed. The mean age of the patients was 46 years (range, 18 to 82 years). Fifteen of the patients were male and eight were female. Twelve were right-handed and 11 were left-handed. Patients' characteristics are summarized in Table 1.
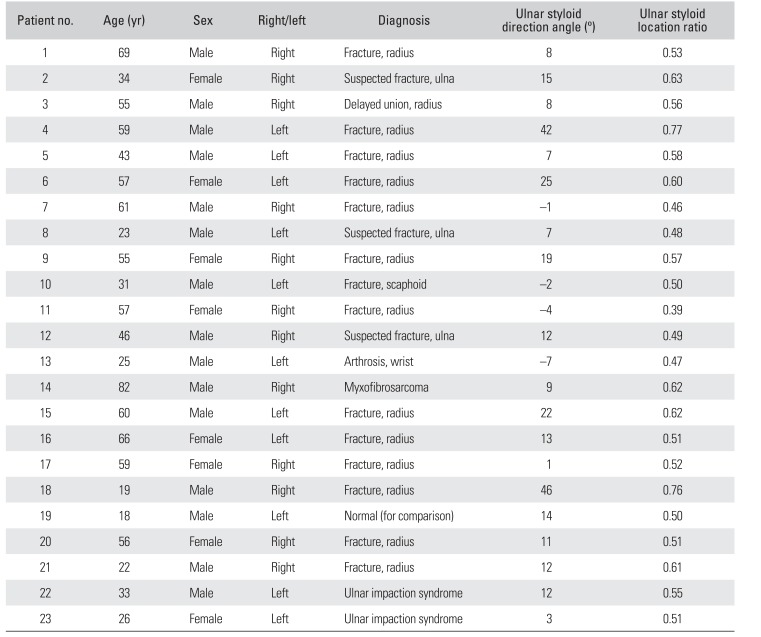
Table 1
Clinical Characteristics and Measurement Values (Ulnar Styloid Direction Angle and Ulnar Styloid Location Ratio) of the 23 Patients
![]()
The absolute location in this study was defined as the location of the ulnar styloid process on the axial plane of the ulnar head relative to the long axis of the humeral shaft, with the elbow set in the position for standard lateral radiographs of the wrist. Because our study was not performed with normal wrists, inclusion and exclusion criteria were set to ensure a normal articulation and relationship between the ulnar styloid process and the humeral shaft. Inclusion criteria were intact medial and lateral ligamentous complexes of the elbow and CT images that had been taken with the elbow flexed between 70° and 90°. Exclusion criteria were patients with ulnar fracture, deformity of the forearm bone, or unstable humeroulnar joint. The axial images of the forearm CT were reconstructed to be perpendicular to the distal ulnar shaft.
The standard true lateral view of the wrist is obtained with the elbow flexed to 90°, the arm adducted against the trunk, and the forearm placed on the film plate in neutral rotation.6) The X-ray beam is aligned vertically over the radial styloid, 100 cm from the film. In this position, the central beam is almost parallel to the long axis of the humerus (Fig. 3). Therefore, we assumed that the true lateral view of the wrist is the orthogonal projection of the wrist by the X-ray beam parallel to the humerus on the axial plane of the distal ulna.
 | Fig. 3Positioning for standard lateral radiographs of the wrist. The elbow is flexed to 90°, the arm is adducted against the trunk, and the forearm is on the film plate in neutral rotation. The X-ray beam is aligned vertically over the radial styloid 100 cm from the film. In this position, the central beam is almost parallel to the long axis of the humerus.
|
Based on the assumption that such an orthogonal projection is to be obtained, a straight line passing through the center of the ulnar head and parallel to the long axis of the humerus (line UH) was drawn on the axial images of the wrist CT obtained with the elbow flexed (Fig. 4). This line would be in the same direction as the X-ray beam for a standard lateral view. Then a straight line was drawn from the center of the ulnar head to the center of the ulnar styloid process (line C). To identify in which direction the ulnar styloid process is located on the axial plane of the ulnar head, the angle between line C and line UH was measured as the “ulnar styloid direction angle.”
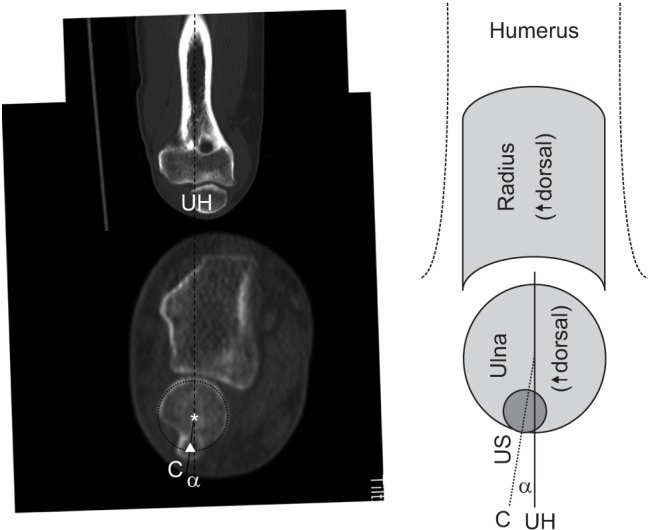 | Fig. 4Measurement of ulnar styloid (US) direction angle. A straight line passing through the center of the ulnar head and parallel to the long axis of the humerus (line UH) was drawn on the axial image of the wrist computed tomography obtained with the elbow flexed (arrowhead: center of the ulnar styloid process, asterisk: center of the ulnar head). Then a straight line was drawn from the center of the ulnar head to the center of the ulnar styloid process (line C). To identify in which direction the ulnar styloid process was located on the axial plane of the ulnar head, the angle between line C and line UH (US direction angle = angle α) was measured.
|
To identify how volarly or dorsally the ulnar styloid process should be located on the lateral view of the wrist, lines being parallel to the line UH and passing the most volar/dorsal point of the ulnar head (line V/line D) and the center of the ulnar styloid process (line US) were drawn on the same axial images (Fig. 5). The ratio of the distance between line V and line D (DUH, diameter of the ulnar head) and the distance between line V and line US (DUS, distance of the center of the ulnar styloid from the volar-most aspect of the ulnar head) was calculated as the “ulnar styloid location ratio.” Values are presented as mean and standard deviation.
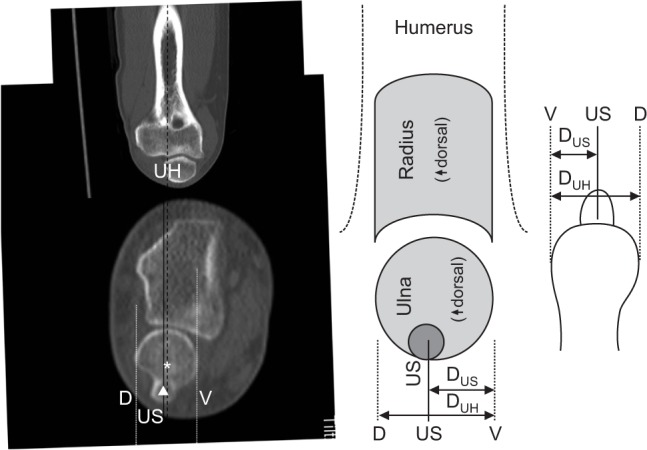 | Fig. 5Calculation of ulnar styloid (US) location ratio. Straight lines passing through the most volar and dorsal points of the ulnar head (line V and line D) and the center of the ulnar styloid process (line US) parallel to the long axis of the humerus (line UH) were drawn on the axial image of the wrist computed tomography obtained with the elbow flexed (arrowhead: center of the ulnar styloid process, asterisk: center of the ulnar head). To identify how volarly or dorsally the ulnar styloid process should be located on the lateral view, the ratio of the distance between line V and line D (DUH, diameter of the ulnar head) and the distance between line V and line US (DUS, distance of the US) was calculated (US location ratio = DUS/DUH).
|
Go to : 
RESULTS
The mean ulnar styloid direction angle was 12° ± 13° dorsally (Fig. 6). The mean ulnar styloid location ratio was 1 : 0.55 ± 0.09. Clinical characteristics and measurement values are presented in Table 1.
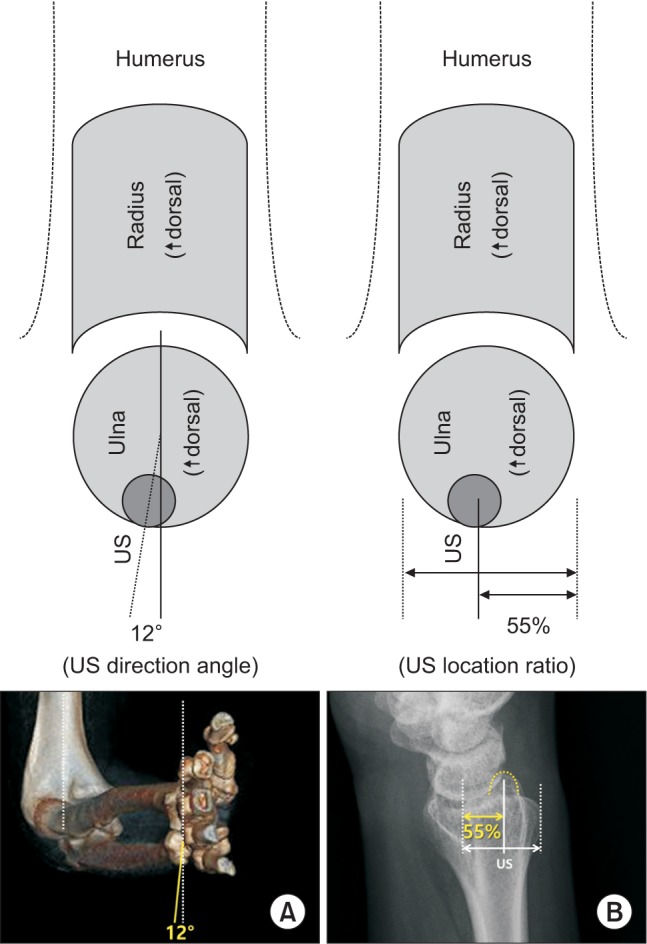 | Fig. 6The absolute location of the ulnar styloid process on the axial plane of the ulnar head relative to the long axis of the humeral shaft with the elbow set in the position for standard wrist lateral radiographs. (A) The mean ulnar styloid (US) direction angle is 12° ± 13° dorsally. (B) The mean US location ratio is 1 : 0.55 ± 0.09.
|
Go to :
DISCUSSION
The ulnar styloid direction angle of 12° means that the ulnar styloid is located at nearly the ulnar-most and slightly dorsal aspects of the ulnar head on the axial plane. It also indicates that the ulnar styloid is located almost on the opposite side of the humerus when the elbow is flexed. In addition, the ulnar styloid location ratio of 0.55 shows that the ulnar styloid should appear almost in the middle (55% dorsally) of the ulnar head on standard lateral views of the wrist taken in neutral forearm rotation. Hagert and Hagert7) also reported that the ulnar styloid was shown at the center of the ulnar head on a true lateral view of the distal radioulnar joint (DRUJ). However, it was not based on scientific measurements, whereas our study revealed that the true position is not exactly the center of the ulnar head through scientific investigation although the difference is small. If the ulnar styloid is shown exactly at the center of the ulnar head on a lateral radiograph of the wrist, now we may think that the lateral view was probably taken with the forearm slightly pronated.
The location of the ulnar styloid process can be confusing because the radius (and the hand) rotates around the ulna. The ulnar styloid process can be located either volar or dorsal to the hand when the forearm is pronated or supinated (Figs. 7 and 8). The volar/dorsal direction of the ulna relative to the radius is the same only when the forearm is in neutral rotation. In fact, the “lateral view of the wrist” in practice is the lateral view of the radius, which rotates along with the hand. Therefore, the ulnar styloid process is located dorsal to the radius on lateral views of the wrist when the forearm is supinated (Fig. 9). Lateral views of the wrist taken with the forearm supinated have been presented in a number of previous publications including studies on the radiographic evaluation of the wrist or the ulnar variance that varies with forearm rotation.389) In these papers, the distal ulna looks the same in PA and lateral views, with the ulnar styloid located dorsally in lateral views. If someone thinks that the ulnar styloid is located dorsally, he or she may be familiar with lateral radiographs taken with the forearm supinated.
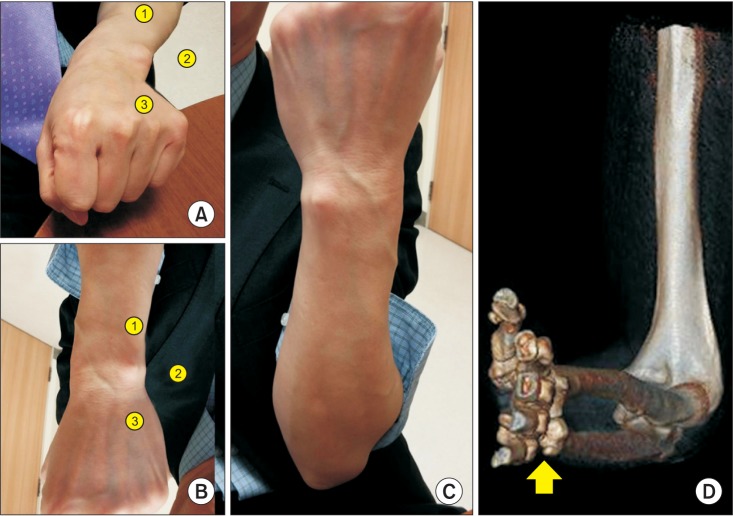 | Fig. 7The location of the ulnar styloid process relative to the hand. Where is the ulnar styloid in (A) and (B)? Although its position may be thought to be similar in (A) and (B), the actual location of it is different. In fact, (A) shows a pronated wrist and (B) shows a supinated wrist. (B) is a 180°-rotated image of the original photo (C). Therefore, the closest answer is number ③ in (A) and number ① in (B). (D) The ulnar styloid process is located on the opposite side of the humerus when the elbow is flexed regardless of the forearm rotation (arrow: ulnar styloid process).
|
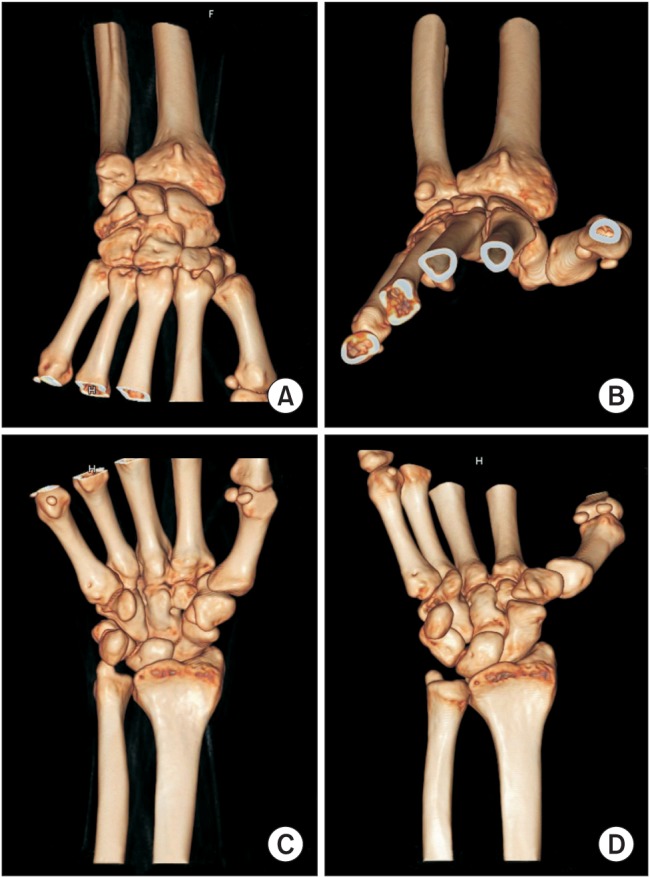 | Fig. 8Locations of the ulnar styloid process in the wrist with the forearm pronated (A, C) and supinated (B, D). The ulnar styloid process may be located either volar (A, C) or dorsal (B, D) to the hand when the forearm is pronated or supinated.
|
 | Fig. 9Forearm rotation and relevant wrist radiographs. (A) Standard posteroanterior view with neutral forearm rotation. (B) Standard lateral view with neutral forearm rotation (arrows: ulnar styloid process, arrowheads: ulnar head). Note the ulnar styloid process is located almost midway from the ulnar head. (C) Lateral view taken with the forearm supinated. Note the distal ulna looks almost the same as that on the posteroanterior view. US: ulnar styloid.
|
The probable cause that the lateral radiographs of the wrist are taken commonly with the forearm supinated is that lateral views are usually taken immediately after PA views. After positioning the patient for the PA view (Fig. 9A), it is easier to supinate the forearm (Fig. 9C) for the lateral view than to reposition the patient for the true lateral view (Fig. 9B). In this case, the ulna is fixed to the humerus and maintains its position, whereas the radius and the hand rotate around the ulna. Consequently, the radius and the hand look different in PA and lateral views, but the ulna looks the same in PA and lateral views (Fig. 9A and C). However, the distal ulna in the lateral view taken with the patient in the correct position for the lateral radiograph of the wrist (Fig. 9B) looks different from that in the PA view (Fig. 9A), and the ulnar styloid is located almost midway from the ulnar head in the lateral view, in contrast to the ulnar-most location in the PA view.
In addition to the standardization of lateral radiographs of the wrist, there are other benefits of establishing the absolute location of the ulnar styloid process. For example, it would be possible to determine whether the forearm is pronated or supinated on axial magnetic resonance imaging (MRI) and CT images of the wrist by referencing the direction of the ulnar styloid in relation to the radius (Fig. 10). This can be particularly useful when those images are obtained to evaluate parameters dependent on the degree of forearm rotation, such as subluxation of the DRUJ or the position of the extensor carpi ulnaris tendon.1011) If forearm rotation is different on two axial images, such parameters cannot be compared directly. However, to our knowledge, no study on DRUJ subluxation has presented verification of forearm rotation on axial images of the wrist. Now, with our results, a retrospective investigation in terms of pronation and supination can be performed, which we think should be useful for future studies focusing on investigations into these areas. Clinically, awareness of the absolute location of the ulnar styloid facilitates greater precision in the examination of the wrist structures, such as the extensor carpi ulnaris tendon that is just beside the ulnar styloid. It may also help make ulnar-sided arthroscopic portals in the wrist.
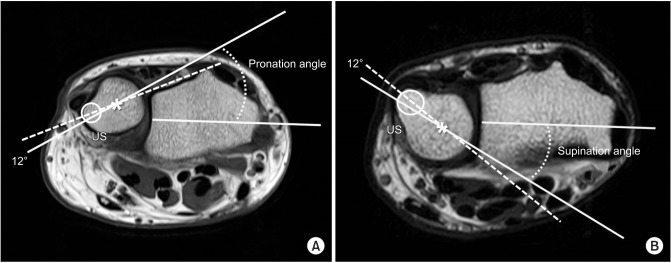 | Fig. 10Measurement of forearm rotation on axial images of wrist magnetic resonance imaging (MRI). It is possible to determine the amount of forearm pronation (A) and supination (B) on existing axial MRI or computed tomography images of the wrist by referencing the direction of the ulnar styloid (US) relative to the radius (asterisks: center of the ulnar head, circle: US).
|
There are several limitations in this study. First, the elbow was not uniformly flexed to 90° in all of the patients. We tried to take the CT scans with the elbow flexion of 90° because in general it is the position in which wrist lateral views are taken; forearm rotation is measured; and ulnar variance is determined.1213) However, the actual elbow flexion was less than we expected probably because of the positioning in the CT gantry. As a result, there may be errors associated with the degree of elbow flexion, which alters the screw displacement axis (SDA) of the elbow (or elbow flexion axis).14) However, as the SDA deviation is less than 5° in 3D space throughout the whole range of elbow flexion,14) such an error may be minimal within our inclusion criteria (elbow flexion 70° to 90° and intact elbow ligament complexes). In addition, there is a report that there is no ulnar axial rotation during elbow flexion-extension motion,15) which additionally justifies our study on the location in the axial plane of the ulnar head. The CT scans in our study were not uniformly taken with a certain forearm rotation either. However, the influence of this is thought to be small since SDA patterns are similar regardless of the forearm rotation in the intact elbow.14) Second, there could be measurement errors due to the asphericity of the ulnar head. Some discrepancy may exist between the direction angle and the location ratio, although its effect on overall tendency may be minimal. Third, our study has not been performed with normal wrists. To overcome this, we excluded cases with structural alteration of the ulna or unstable ulnohumeral joint. We believe that this essentially keeps the spatial relationship between the ulnar styloid and the humerus sound. Fourth, the number of CT image sets included in the analysis is small, and patients enrolled in this study do not represent all races or generations. However, the significance of this study can be found in the fact that this is the first study to scientifically determine the absolute location of the ulnar styloid process in neutral forearm rotation, which used to be thought as “approximately somewhere on the ulnar side.” Future studies including cadaveric ones may reveal differences between races, generations, and genders.
In conclusion, the ulnar styloid process is located at nearly the ulnar-most (the opposite side of the humerus with the elbow flexed) and slightly dorsal aspects of the ulnar head in the axial plane view obtained in neutral forearm rotation. It should appear almost midway (55% dorsally) from the ulnar head on standard lateral views of the wrist with neutral forearm rotation. These standard locations would facilitate more precise examination and evaluation of the wrist and could help clinicians determine whether the forearm is in neutral rotation or pronated/supinated on an axial wrist CT/MRI scan or a lateral radiograph.
Go to :
 XML Download
XML Download