

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A relevant literature review revealed that scaphoid fractures account for over 60% of carpal bone fractures and 11% of all hand fractures.1) Historically, casting with thumb immobilization has been the primary method of treatment.2) However, orthopedic practice has evolved dramatically over the years and recently, treating nondisplaced or minimally-displaced scaphoid fractures with early open reduction and internal fixation instead of cast immobilization has been trending.2) Orthopedic surgeons subspecializing in upper extremity/hand surgery are more likely to intervene surgically than generalists (34.6% vs. 6.0%, p = 0.0002).3) It has also been noted that young surgeons, 45-years-old and younger, prefer the modern method for treating scaphoid fractures.3) Regardless, there is insufficient evidence of its greater benefits over its traditional counterpart.2)
One study reported that with prolonged casting, joint stiffness may arise, which could be avoided by surgical intervention.4) On the other hand, another study claimed that non- and minimally-displaced scaphoid fractures are best treated conservatively citing that while surgical treatment may provide improved functional outcomes in the short term, it comes with a possible increase in the risk of osteoarthritis in the long run.5) These study discrepancies lead to debates on whether one therapeutic procedure is better than the other. Throughout the years, a handful of randomized clinical trials comparing surgical and conservative treatments have been done across countries in the hope of finding the best evidence for a better treatment but unfortunately were left with insufficient evidence for a stronger claim.4567891011)
The management of undisplaced and minimally-displaced scaphoid fractures remains a matter of discussion. Considering patients' uniqueness, for each individual case, one option is allegedly better than the other. However, when faced with two good options, direct patient care is balanced against the level of risk when deciding the course of action based on the evidence available. This results in decisions influenced by the hospital to which the patient is admitted and the level of supervision provided by the most responsible physician.
Hence, the main objectives of this systematic review are to identify and evaluate the highest level of evidence available to determine whether undisplaced and minimally-displaced scaphoid fractures should be managed surgically or conservatively. Further, this paper aims to summarize the complications of these two therapeutic procedures from the selected studies to weigh their advantages in terms of long-term benefits.
METHODS
This present study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Search Strategy
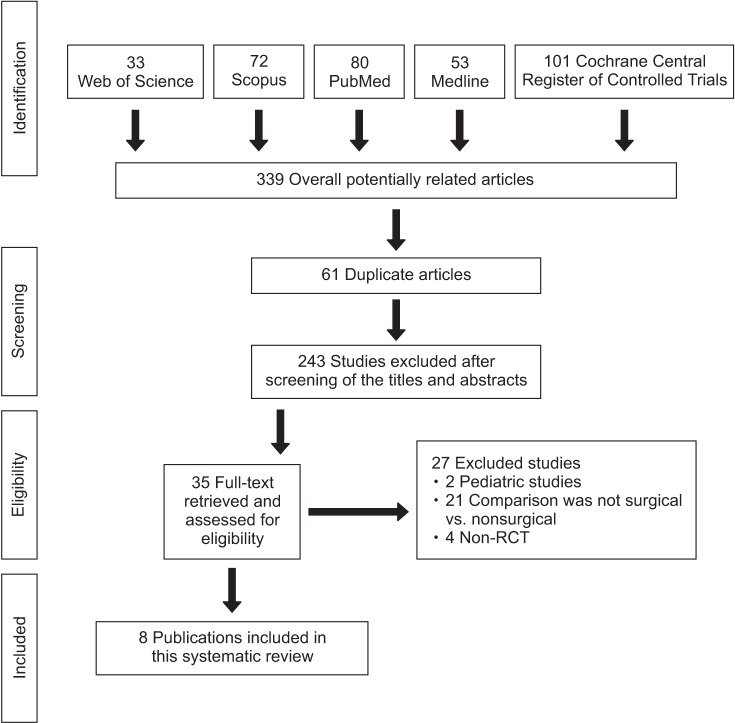
The search in five databases including PubMed, Medline, Cochrane Central Register of Controlled Trials, Scopus, and Web of Science found 339 potentially related articles using the keywords “fracture,” “scaphoid,” “surgical,” “nonsurgical,” “operative,” “non-operative,” “conservative,” “management,” and “treatment.” The search was limited to clinical trials without any language restrictions from the earliest date until January 2017. Two independent authors identified randomized controlled trials (RCTs) and screened the studies based on the established inclusion criteria. The quality of the included RCTs was evaluated further using the PEDro scale. The risk of bias of each eligible study was assessed in accordance with the Cochrane risk of bias tool.12)
Inclusion and Exclusion Criteria
The included studies were original articles that compared surgical and conservative therapeutic treatments of undisplaced and minimally-displaced scaphoid fractures. Criteria for eligibility are outlined as follows: (1) studies: RCT, comparative study; (2) patients: undisplaced and minimally-displaced scaphoid fractures; (3) intervention: surgical procedures (open reduction and internal fixation or percutaneous fixation); (4) comparison: conservative treatment (Colles cast, short-scaphoid cast, and long-arm scaphoid cast); (5) outcomes: functional outcomes including range of motion (ROM), grip strength, pinch strength, and return to work.
Meanwhile, trials involving pediatric, displaced, and chronic fractures were excluded in this analysis due to the following reasons: acute displaced pediatric scaphoid fractures are treated conservatively with casting and immobilization,13) acute displaced scaphoid fractures are treated surgically by anatomical reduction and fixation,1415) chronic (nonunion) scaphoid fractures are treated surgically by bone grafting, surgical fixation, or other operative methods.1617)
Data Analysis
Review Manager (RevMan) ver. 5.3 (The Cochrane Collaboration, Copenhagen, Denmark) was used for data processing and data analysis. Standardized mean differences with 95% confidence intervals (CIs) were calculated for continuous outcomes and risk ratios (i.e., relative risk). For dichotomous outcomes, 95% CIs were calculated in both treatment groups. A sensitivity analysis was performed by investigating the effect of each individual study on the pooled effect size. Funnel plots were used to assess possible publication bias. Because of the limited data available from each RCT for the pooled analysis, treatment effect was defined as significant if p < 0.05.
Go to : 
RESULTS
Fig. 1 shows the process of identifying the included studies with a total of eight articles eligible for analysis.4567891011) The PEDro scale was also used to determine which study is likely to be internally valid (criteria 2–9) and could have sufficient statistical information to make their results interpretable (criteria 10–11) with authors' judgment ranging from 5 to 9.
Moreover, Table 1 summarizes the studies' characteristics. The sample size of the included studies ranges from 25 to 88 with ages ranging from 15 to 75 years. The total fractures were 378 (182 and 196 for surgical group and conservative group, respectively). The duration of follow-up was 10 weeks to 12 years, and most of the studies reported ROM, grip strength, and time to return to work as outcome variables.45678910)

Table 1
Main Characteristics of All Studies Included in the Analysis
| Study | No. of surgical/conservative treatment | Age (yr) | Method | Outcome measured | Follow-up duration | PEDro scale | |||
|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | Conservative treatment | Surgical treatment | |||||
| Clementson et al. (2015)5) | 14/24 | 11/20 | 3/4 | 18–62 | Below-elbow thumb spica cast | Wrist arthroscopy and antegrade screw | · Range of motion (ROM) | 1–6 yr | 9 |
| · Grip and pinch strength | |||||||||
| · Radiographic signs of arthritis | |||||||||
| · Patient Satisfaction | |||||||||
| McQueen et al. (2008)6) | 30/30 | 26/24 | 4/6 | 17–65 | Immobilization in a cast | Acutrak screw | · ROM | 8–52 wk | 9 |
| · Grip and pinch strength | |||||||||
| · The modified Green/O'Brien functional score | |||||||||
| · Return to work (RTW) and sports | |||||||||
| · Radiological evidence of union | |||||||||
| Vinnars et al. (2008)7) | 26/26 | 19/17 | 7/9 | 18–61 | Below-elbow scaphoid cast with the thumb in volar abduction | Herbert screw | · ROM | Median 10 yr | 8 |
| · Grip strength | |||||||||
| · RTW | |||||||||
| · Limb specific outcome scores | |||||||||
| · Osteoarthritis prevalence | |||||||||
| Dias et al. (2005, 2008)810) | 44/44 | 31/31 | 13/13 | 16–61 | Below-elbow plaster cast immobilization | Herbert screw | · ROM | 6.1–9.2 yr | 9 |
| · Grip and pinch strength | |||||||||
| · RTW | |||||||||
| · Patient-rated wrist evaluation | |||||||||
| Adolfsson et al. (2001)9) | 25/28 | 20/19 | 5/9 | 15–75 | Below-elbow plaster cast immobilization | Acutrak screw | · ROM | From 10 wk | 5 |
| · Grip strength | |||||||||
| · Rate of union/time to union | |||||||||
| · Complications | |||||||||
| Bond et al. (2001)4) | 11/14 | 8/13 | 3/1 | 18–34 | Long-arm cast immobilization | Acutrak screw | · ROM | 2 yr | 6 |
| · Grip strength | |||||||||
| · RTW | |||||||||
| · Rate of union | |||||||||
| · Overall patient satisfaction | |||||||||
| Saeden et al. (2001)11) | 32/30 | 27/22 | 5/8 | 15–50 | Short-arm cast | Herbert screw | · ROM | 12 yr | 7 |
| · Radiological evidence of union | |||||||||
| · RTW | |||||||||
| · Arthritis | |||||||||
| · Rating of pain and discomfort | |||||||||
![]()
Clementson et al.5) reported that the conservative group with a below-elbow thumb spica cast had a significantly better ROM and had reached almost normal values at 26 weeks compared with those who underwent the wrist arthroscopy and percutaneous antegrade screw fixation.
McQueen et al.6) randomly allocated 60 consecutive patients with undisplaced or minimally-displaced scaphoid fractures to percutaneous screw fixation or immobilization in a cast. The conservative group and surgical group consisted of 30 patients each. Minimal initial fracture displacement was present in association with two fractures in the conservative group and five fractures in the surgical group. There were 10 female patients and 50 male patients with a mean age of 29.4 years ranging from 17 to 65 years. Patients had at least 52 weeks of follow-up.
Vinnars et al.7) studied the data of a subgroup of 52 patients from a randomized trial consisting of 26 patients per treatment group. They included acute nondisplaced fractures of the scaphoid (Herbert type A2, B1, B2, and B3 fractures). There were 16 female patients and 36 male patients with a median age of 32 years for the casting group and 29 years for the surgical group. Only additional data from this report (i.e., data not reported by Vinnars et al. in 2008) were used for analysis. The mean duration of follow-up was 10 years, and no patient was lost to follow-up.
In 2008, Dias et al.8) reported on 88 patients with an age range of 16–61 years (9 females and 79 males) who had a clear bicortical nondisplaced or minimally-displaced fracture of the scaphoid. Forty-four patients were allocated to each treatment group, consisting of internal fixation with a Herbert screw or cast immobilization. Minimal initial fracture displacement was present in association with three fractures in the conservative treatment group and eight fractures in the surgical treatment group. Patients were followed for a minimum of 52 weeks.
Adolfsson et al.9) reported on 53 patients (14 women and 39 men) with an age range of 15–75 years with nondisplaced fracture of the scaphoid. The authors randomly allocated 25 patients to surgical treatment (percutaneous screw fixation) and 28 patients to conservative treatment (cast immobilization). Patients were followed for a minimum of 16 weeks.
Bond et al.4) reported on 25 patients with an age range of 18–34 years who had sustained an acute nondisplaced fracture of the scaphoid (Herbert type A2 or B2 fracture). Eleven patients were randomized to percutaneous screw fixation while 14 were randomized to cast immobilization. The mean follow-up range for both groups was 25 months.
Saeden et al.11) randomized 61 patients with 62 acute fractures of the scaphoid to surgical treatment with use of a Herbert screw (32 fractures) and conservative treatment with use of a cast (33 fractures). The age range at the time of injury was 15–50 years. Patients were followed for a minimum of 12 years.
Comparison of the Effect of Surgical and Conservative Treatments on Functional Scores, ROM, Grip Strength, Pinch Strength, RTW Time, and Complications
Table 2 depicts that there are statistically significant differences in the mean functional scores of the surgical group when compared to those of the conservative group after 2 and 4 months of the procedure (p < 0.05). Significant differences are noted in the grip strength of the compared groups at 2, 4, and 6 months, 1 year, and > 1 year after the procedure (p < 0.05). All significant differences favor the surgical group over the conservative group, which may mean that the surgical group improved better and faster
than the conservative group.

Table 2
The Effect of Surgical and Conservative Treatments on ROM, RTW, Grip Strength, and Functional Score with a Significant p-value Only (p < 0.05)
![]()
It is remarkable to note, however, that there are no statistically significant differences in the mean ROM across all months of comparison and in the mean functional scores at 6 months, 1 year and > 1 year, and in the pinch strength at > 1 year (p > 0.05) between the surgical and conservative groups, which may mean that in these tested outcomes, the two therapeutic treatments are equally effective.
Fig. 2 presents that four of the eight studies included in this systematic review reported the time needed to return to work.461011) On the return to work outcome, there is a statistically significant difference (p < 0.05) between the compared groups. The meta-analysis revealed that the return to work time is significantly lower among those who underwent surgical treatment than those who received conservative treatment (weighted mean difference, −6.01; 95% CI, −9.16 to −2.87; p < 0.001).
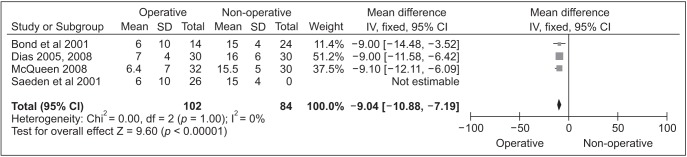 | Fig. 2Forest plot for the weighted mean difference estimate for the time to return to work weighting given to the trial in the overall pooled estimate, taking into account the number of participants and the amount of interstudy variation (heterogeneity) rhombus, and combined effect size. SD: standard deviation, CI: confidence interval.
|
The eight reviewed studies reported the occurrence of complications among patients in both treatment groups variying from malunion, nonunion, osteoarthristis, symptomatic osteoarthritis to further surgical treatment. One study revealed that patients whose radiographic findings showed nonunion with the cast in place for 3 months were treated surgically with Herbert screws.7)
Table 3 and Fig. 3 show that there are no statistically significant differences in the overall complication rate between surgical and conservative treatments (p > 0.05). This may mean that regardless of the treatment, complications are likely to happen.

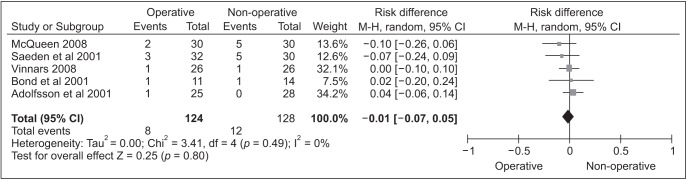 | Fig. 3Forest plot for the risk ratio estimate for the assessment of overall complication rate. CI: confidence interval.
|
Table 3
The Effect of Surgical vs. Conservative Treatments on the Occurrence of Complications
![]()
Of the six studies that reported the incidence of complications in both surgical and conservative treatment groups, only one study reported significant difference in the complication rate (p = 0.036).6) However, combining all the data reported by the five studies,567911) the meta-analysis revealed that there are no statistically significant differences in the incidence of complication rate between the surgical and conservative treatments (p = 0.754), which may mean that complications are likely to occur in both treatments.
Sensitivity Analysis and Publication Bias Analysis
Table 4 and Fig. 4 present the Cochrane risk of bias tool (modified) for quality assessment of randomized controlled trials using RevMan ver. 5.3. Based on the authors' judgments and understating of the eight included studies, blinding of the participants and personnel was not implemented, which may have influenced the outcomes of the included studies (Fig. 5). However, 87% of the studies met the allocation concealment (selection bias) and selective reporting (reporting bias) criteria, which contributed to the overall rating of low-risk of bias (Fig. 6).

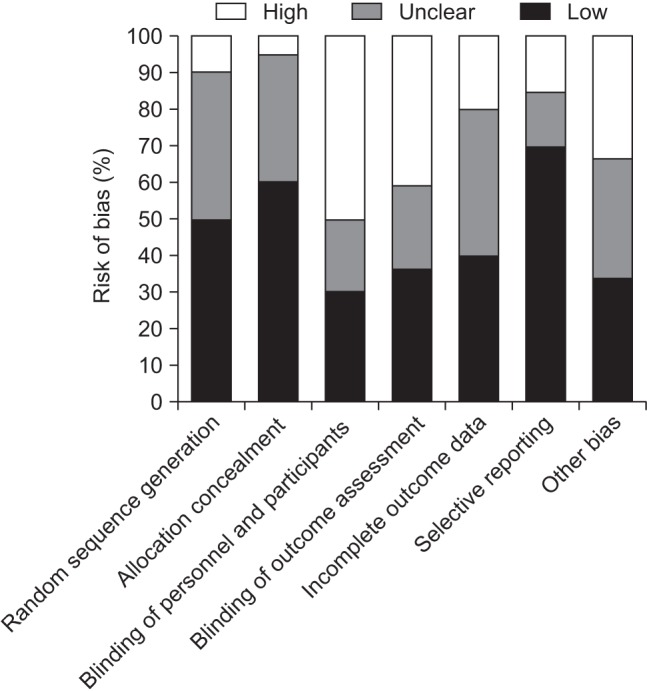 | Fig. 4Risk of bias graph: authors' judgements about each risk of bias item presented as percentages across all included studies.
|
 | Fig. 5Sensitivity analysis and publication bias analysis of the meta-analysis. The figure shows the influence of individual study on summary risk ratio (RR) computed by omitting each study in turn. The vertical axis indicates the overall RR and the two vertical axes indicate the 95% confidence interval (CI). Every circle indicates the pooled RR when the study is omitted in this meta-analysis. The two ends of the dotted lines represent the 95% CI.
|
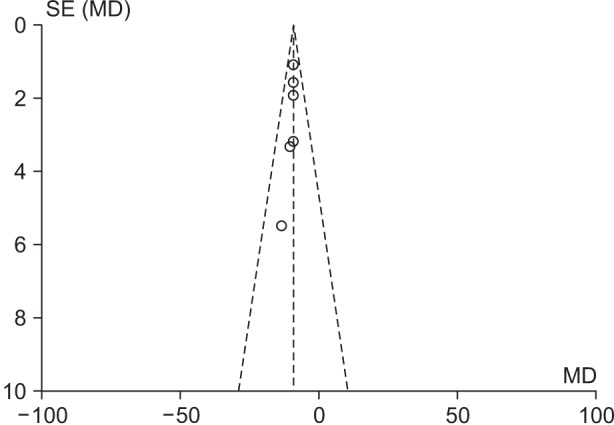 | Fig. 6Begg's funnel plot for publication bias in the selection of studies. The horizontal axis represents the log risk ratio (RR) and the vertical axis indicates the standard error (SE) of the log RR. The vertical line and the sloping lines represent the effects summary RR and the expected 95% confidence interval for a given SE. Each circle represents the eight studies. The symmetrical appearance of the funnel means that there is no publication bias in the selection of the studies included in this metaanalysis. MD: mean difference.
|
Table 4
Risk of Bias Summary: Authors' Judgements about Each Risk of Bias Item for Each Included Study
| Study | Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective reporting | Other bias |
|---|---|---|---|---|---|---|---|
| Clementson et al. (2015)5) | Yes | Yes | No | No | Unclear | Yes | Yes |
| McQueen et al. (2008)6) | No | Yes | No | Yes | Yes | Yes | Yes |
| Vinnars et al. (2008)7) | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Dias et al. (2005, 2008)810) | Yes | Yes | No | No | Yes | Yes | Yes |
| Adolfsson et al. (2001)9) | Unclear | Unclear | No | Unclear | Yes | Unclear | Yes |
| Bond et al. (2001)4) | Yes | Yes | No | No | Unclear | Yes | Yes |
| Saeden et al. (2001)11) | Unclear | Unclear | No | No | Unclear | Yes | Yes |
![]()
Go to :
DISCUSSION
Several studies were documented in the literature comparing the therapeutic advantages of surgical and conservative treatments for acute undisplaced or minimally-displaced scaphoid fractures to determine which method is superior to the other; however, seemingly none of the studies has settled on a definitive conclusion. This systematic review and meta-analysis is a sequel to a study of Shen et al.18) that was published in 2015 to reach a conclusion. Eight studies, including the six studies mentioned in the study by Shen et al.,18) were analyzed with 399 eligible patients randomized to undergo two therapeutic treatments, surgical or conservative. Based on the results presented by each study, this paper suggests that surgical treatment is significantly better in terms of patient-reported functional outcome and grip strength, shorter time for bone union, and earlier return to work while it proposes that there are no statistically significant differences between the two treatments in regard to ROM and complications (malunion, nonunion, osteoarthritis, and symptomatic osteoarthritis), the need for further surgical treatment, avascular necrosis, infection, and procedure failure.
The findings of this study should be judiciously interpreted due to the existence of substantial limitations. Significant heterogeneity is seen in the measured outcomes. The pooled grip strength in five studies456710) was of the dominant-hand injury in 34% to 64% of the cases; however, a relevant literature search revealed that variability exists in the relative strength of the dominant and non-dominant sides in a healthy population and grip strength has shown to be typically greater on the dominant side.192021) Also, the different duration of follow-up of the eight included studies ranging from at least 8 weeks to 12 years is a general source of heterogeneity. Two studies reported that the primary outcome measurement, functional outcome, mainly improved over time between 8 and 52 weeks of follow-up.68) Post-immobilization and active functional use of the hand and wrist play a key role in functional improvement.68) The fact that conservatively managed patients have a relatively shorter mobilization time at the time of the latest follow-up evaluation, due to the method of treatment, produces bias in the assessment of functional outcome in favor of the surgical treatment group.
Another area of concern is the duration of fracture union. It has been noted that surgical fixation for undisplaced scaphoid fractures yields higher union rates and rapid union time.22) As for casting, it typically takes around 9 to 12 weeks for union, which is the reason for many surgeons to avoid the conservative method.22) A recent study, however, revealed that computed tomography (CT) determined scaphoid union could be obtained in approximately 7 weeks with use of a short arm thumb spica.22) Two of the included studies46) used radiographs to determine fracture union, which happens to have poor reliability.23) The validity of fracture union would have been exceptional if CT was used because it is considered to be the most reliable imaging technique for predicting scaphoid fracture union which is used as a standard reference for healing.24)
The measurement of time to return to work was yielded from five studies.4671011) The study of Bond et al.4) consisted solely of full-time military personnel, which happens to be a major source of heterogeneity considering their nature of work as full-duty status. In addition, there is a great possibility that in other studies, time to return to work was shorter than the time of cast immobilization.671011) Thus, many patients, especially nonmanual laborers, may have returned to work prior to cast removal.
The superiority of one therapeutic technique to the other should be considered in an individualized approach. For example, young patients and athletes may not tolerate long durations of immobilization in cast; therefore, surgical intervention is the better choice for them, which also has been reported to provide better range of movement and grip strength than conservative treatment.25) Determination on the best plan of care should be based on the consideration of both the patient and the health care system. Surgical and conservative treatments impose a burden on hospital resources and governmental budgets. Economically speaking, the surgical approach happened to require more than five times the direct cost of conservative treatment although it can be indirectly 60% less costly than casting.3) Indirect costs can be affected by the time required to return to work, for instance.3) Vinnars et al.7) examined direct and nondirect costs concluding that there were long periods of absenteeism in manual than nonmanual workers. Nonmanual workers had less total costs, herein, making the option of surgery for manual workers seem more rational.
The findings of the present review are consistent with those of the systematic review and meta-analysis of Yin et al.26) that included seven articles, which were also included in our study, utilizing stricter inclusion criteria to examine randomized and quasi-randomized trials. Their final conclusion supports our conclusion that surgical management of acute nondisplaced or minimally-displaced fractures has not yet been proven to be superior to conservative management. Although a systematic review was done on some variables, the inconsistency of reported data made pooling of data impossible at times. Moreover, the lack of patient homogeneity and the presence of confounding factors limited the ability to perform a meta-analysis on the entire groups, and such issues were also noted in the study of Shen et al.18) It is indeed critical for future clinical studies to report protocols carefully,18) increase the number of trials when comparing the effects of surgical versus conservative treatments, and take into consideration the effect of demographics, types of fractures, duration of follow-up, and types of surgical and conservative treatments, which have seemingly limited this systematic review. Some of the included studies reported surgical treatment was advantageous over conservative management; however, there is insufficient evidence to make definitive conclusions. Hence, the superiority of one method to the other could not be determined.
Go to :
 XML Download
XML Download