

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Labial melanotic macules (LMMs) are benign pigmented lesions that are commonly encountered in daily practice. LMMs are asymptomatic, discrete, tan-brown to black lesions, which usually less than 1 cm in maximum dimension12. Histopathologically, LMM represent increased levels of melanin pigments in the basal epidermal layer with normal or slightly more than normal melanocyte numbers12.
The diagnostic accuracy of dermoscopy for pigmented skin lesions has been widely demonstrated, but despite this, its merits for the diagnosis of LMM have not been well investigated3456. Furthermore, these reports did not well characterize the unique dermoscopic features of LMM, because it had encompassed entire pigmented lesions on mucocutaneous junction and mucous membrane356. The aim of this retrospective study was to describe and characterize the dermoscopic patterns exhibited by LMM.
MATERIALS AND METHODS
The medical records, clinicodermoscopic photographs, and histopathologic slides of 60 patients (80 lesions) treated at the outpatient clinics of two Korean tertiary teaching hospitals (Pusan National University Hospital and Pusan National University Yangsan Hospital) from 2007 to 2015 were retrospectively reviewed. All 80 patients were diagnosed as having LMM based on clinicopathologic findings. Patient genders, ages, and lesion dermoscopic pattern types were retrieved. The following exclusion criteria were applied: 1) Laugier-Hunziker syndrome, neurofibromatosis, McCune-Albright syndrome, Peutz-Jeghers syndrome, LAMB (lentigines, atrial myxomas, mucocutaneous myxomas, and blue nevi) syndrome, and the associated Carney syndrome; 2) Addison diseases; 3) postinflammatory conditions, such as, lichen planus or smoker's melanosis125. Digital dermoscopic images of selected lesions were acquired using a dermoscope (Dermlite II Pro HR equipment, 10×magnification; 3Gen, LLC, Dana Point, CA, USA) attached to a digital camera (Sony Cybershot DSC-W290, 5×optical zoom, 12.1 megapixels; Sony Corporation, Tokyo, Japan). The study was exempted from the requirement for approval by the ethics committee of Pusan National University Hospital (IRB no. H-1703-012-053), and informed consent was obtained from patients included in our study. All the lesions were determined by two independent dermatologists that were experts in dermoscopy and specific patterns were considered present when both observers agreed.
Ten dermoscopic features were described using the terms previously reported for mucocutaneous lesions, but some of these terms were revised; 5 benign features (background brown pigmentation, parallel lines, circular lines, overlapping vessels, and structureless black pigmentation) and 5 malignant features (irregular network, irregular dots and globules, blue-white veil, atypical vessels, and reticular depigmentation)3456.
RESULTS
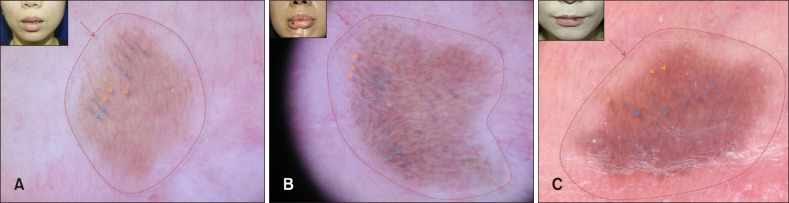
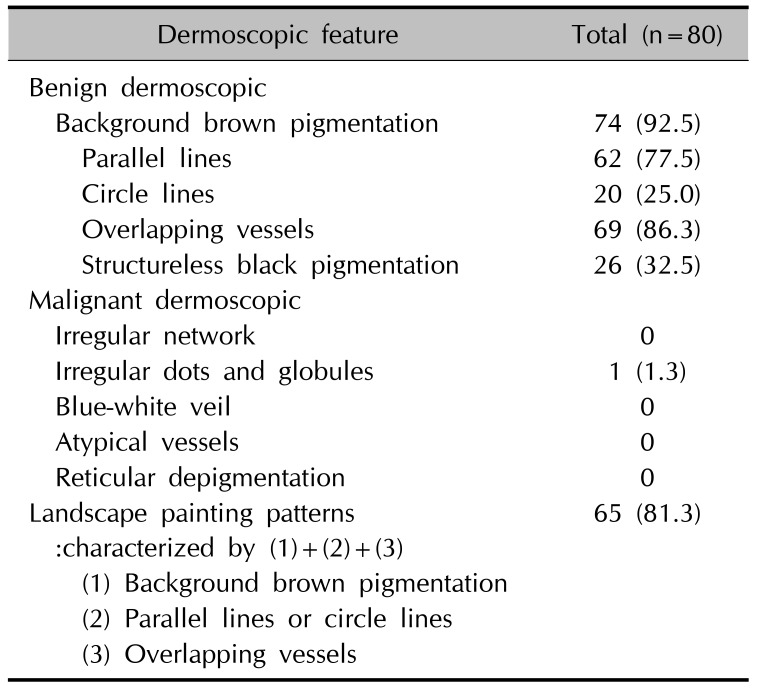
Eighty LMM lesions of 60 patients (13 males and 47 females; mean age, 49.8 years; range, 12 to 81 years) were included in the present study. Background brown pigmentation was observed by dermoscopy in 74 of these lesions (92.5%). Parallel lines, which appeared as linear or curved streaks running parallel to the skin surface, were observed in 62 (77.5%). Circular lines appearing as round to oval structures were also observed in 20 lesions (25.0%). Overlapping vessels characterized by duplicating erythematous vessels to parallel or circle lines were observed in 69 (86.3%). Structureless black pigmentations appeared as diffuse homogenous black pigmentation or variegated dark brown to black pigmentation (without dots, globules, a pigment network, or streaks) were observed in 26 (32.5%) (Fig. 1, Table 1).
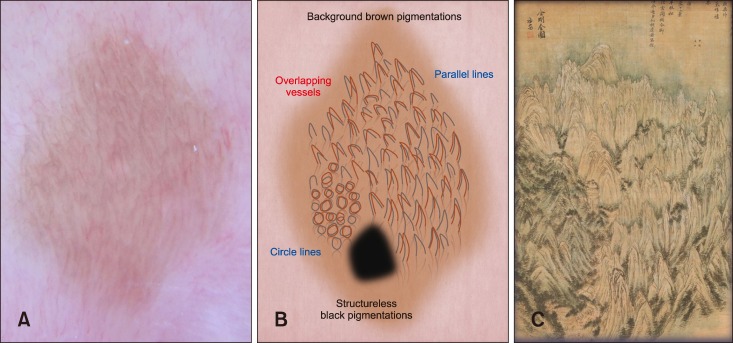
We described the co-presence of three features, that is, background brown pigmentation, parallel lines or circular lines, and overlapping vessels (Fig. 2) were described as ‘landscape painting patterns’ (derived from the Korean landscape masterpiece called ‘A General view of Mt. Geumgangsan’ painted by Jeong Seon in the 18th century). This unique pattern was identified in 65 of the 80 lesions (81.3%). However, only 1 of the 80 lesions exhibited irregular dots and globules suggestive of malignancy. No lesion presented as an irregular network, blue-white veil, atypical vessels, or reticular depigmentation (Table 1).
DISCUSSION
LMM is a benign pigmented lesions of the mucosa characterized by hyperpigmented basal keratinocytes1. Despite its benign behavior, on clinical grounds the differentiation of LMM may be frequently required from malignant melanoma possibly being characterized by asymmetry, variegated pigmentation from light to dark brown, irregular borders, and large size56. Dermosocpy is an emgerging technique that allows for noninvasive imaging of the skin and mucosa.
However, as far as we know, most of the literature on dermoscopy related to LMM has primarily been focused on integrated analysis of the mucocutaneous lesions including lips, oral cavity, and vulva (not confined to only lips)356. Mannone et al.3 identified three major dermoscopic patterns in benign mucosal melanotic macule, known as parallel pattern, structureless pattern and reticular-like pattern3. Lin et al.5 reported ring-like pattern and its variant (fish scale-like pattern and hyphal pattern) in 20 labial and 4 penile lesions of mucosal melanotic macules. In addition, the previous largest scale study was done by Blum et al.6, which included 60 lesions of LMM. In a total of 140 pigmented mucosal lesions, they found 5 patterns including 67 structureless, 64 lines, 26 circles, 8 globules/clods, and 10 dots. Remarkably, they had presented very simple descriptions that can cause diagnostic confusion6.
Therefore, we performed this study to confirm dermoscopic accuracy in the diagnosis of LMM, and so to obviate the need for biopsies in the lip which is a sensitive part of the body. In comparison with the findings of previous reports356, the unique aspects of our study are larger sample size than before and confined to one disease entity as LMM to achieve detailed observation. In addition, we investigated more diverse dermoscopic features of the pigmentations and vasculature using uniform terminology for delineating these features3456.
In our study, the peculiar dermoscopic features of LMM, that is, landscape painting patterns was presented, and need to be considered as the key diagnostic criteria for LMM. This important feature is supposed to enable correct diagnosis of benign labial lesions and help to allow earlier diagnosis of malignant changes (Fig. 2). In addition, our results indicate a close correlation between dermoscopic patterns and underlying histologic features. The parallel or circle lines represent the melanin pigmentation within basal layer, and the characteristic histologic features of LMM. The overlapping vessels indicated markedly dilated capillaries in rete ridges and the background brown pigmentations can be explained by melanins and melanophages at all levels of the epidermis or the dermis12.
Our study had several limitations. It was an uncontrolled, non-double-blind study. The study did not reflect the variables of age, sex, and the locations and activity of the lesions. In particular, we did not compare the features between LMM and melanoma.
In conclusion, this study clearly shows that dermoscopy can be useful tool for diagnosing LMM, and landscape painting patterns may represent a new dermoscopic clue for the diagnosis of the lesions.
 XML Download
XML Download