

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various cutaneous tumors are known to become larger or worse during pregnancy. Eccrine poroma is a benign adnexal tumor originating from the epidermal sweat duct unit. Herein, we introduce an interesting case of eccrine poroma on the left palm of a pregnant woman which increased in size rapidly during pregnancy.
CASE REPORT
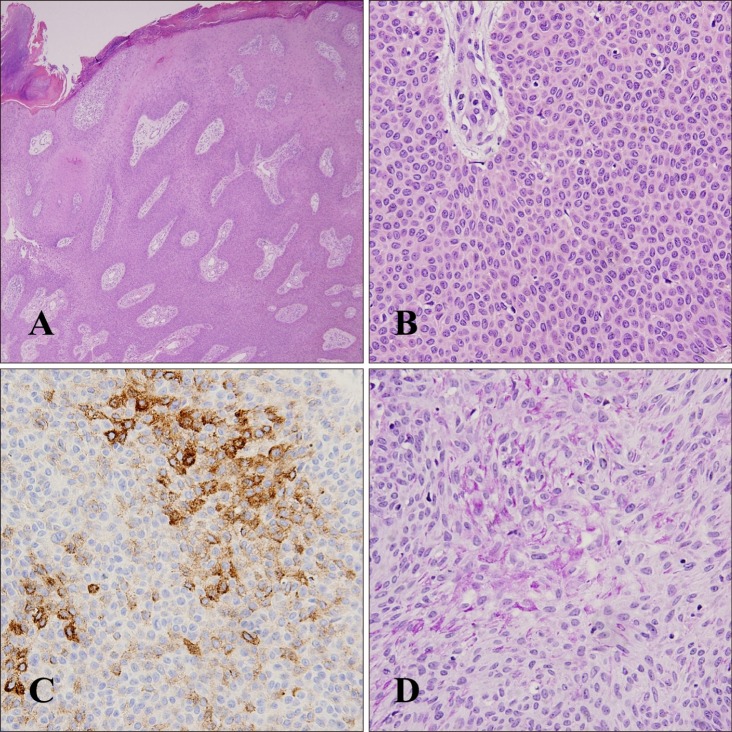
A 37-year-old, 9-month pregnant woman presented with a dark red colored, bean-sized, pedunculated mass on her left palm (Fig. 1). It was first noticed 10 years previously as a tiny papule, which remained unchanged without any discomfort for a long time, but it suddenly increased in size after she conceived. As it enlarged, she began to feel pruritus and tenderness in the lesion. There was no history of trauma or infection, and palpable regional lymph nodes were not detected. A shave biopsy with complete removal was performed, and the specimen revealed that a large aggregation of neoplastic cells replacing epidermis extended into the dermis in broad anastomosing bands (Fig. 2A). The tumor was predominantly composed of uniform, dark basophilic, cuboidal poroid cells which were united by intercellular bridges (Fig. 2B). There was some mitosis, but no cellular atypia was found. Peripheral palisading, which is a characteristic feature of basal cell carcinoma, was not seen. The tumor cells were focally positive for epithelial membrane antigen (Fig. 2C). The structures staining with periodic acid-Schiff stain were also observed (Fig. 2D). Based on the above findings, the tumor was finally diagnosed as eccrine poroma. She has been under observation with no evidence of recurrence for 5 months.
DISCUSSION
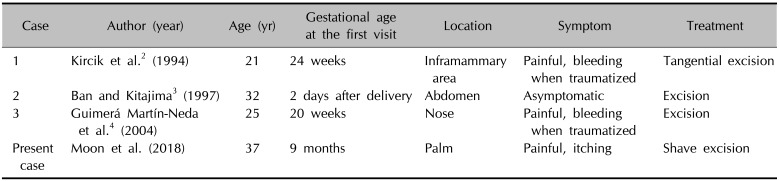
Eccrine poroma is a benign sweat gland tumor arising from the cells differentiating towards the intraepidermal ductal portion of eccrine sweat duct1. It is a common skin disorder predominantly found on the sole, but only three reports demonstrating enlargement during pregnancy have been documented (Table 1). Unlike the prevalent sites where eccrine poroma usually appears, the worsened cases during pregnancy described their lesions in unusual sites such as inframammary skin, abdomen, and nose234. This is the first report of eccrine poroma on the palm which was exacerbated during pregnancy.
The pathogenesis of this unique event is unclear, but like other dermatoses modified by pregnancy it is accepted that the altered physiologic status of skin appendages due to pregnancy may act as a key factor. Generally increased activity of eccrine glands is suggested to contribute to the sudden growth of eccrine poroma4. This hypothesis seems reasonable, but it cannot totally explain our case because the palm is known to be the only area where the activity of eccrine glands decreases during pregnancy45. Therefore, other intrinsic or extrinsic causes may have been involved in our patient although she denied an antecedent traumatic episode. We suggest that the elevated level of angiotensin II during normal pregnancy may play a causative role, because some of tumor cells in eccrine poroma can express angiotensin type 1 receptors which bind to angiotensin II67. The stimulation of angiotensin type 1 receptors by angiotensin II activates phosphokinase C and induces intracellular calcium influx, subsequently promoting the expression of c-Fos and c-Jun which are major transcription factors related in the stimulation of mitogenesis7. To demonstrate this new hypothesis, we tried to measure the expression of angiotensin type I receptors in our case, but unfortunately failed to perform the test because the patient refused to consent. Additional research is needed to prove our hypothesis. Likewise, some cases of malignant transformation from benign poroma to eccrine porocarcinoma during pregnancy have been published89. In this situation, the declined immune function during pregnancy is presumed to be highly associated9.
Rapidly growing eccrine poroma during pregnancy accompanies morphologic variability. Kircik et al.2 found an enlarged, erythematous, lobular, sessile, and painless nodule below the left breast. Ban and Kitajima3 demonstrated a black colored, pedunculated, and soft abdominal tumor, which had similar appearance to our case except color. Guimerá Martín-Neda et al.4 described the lesion on the nasal tip as an exophytic and sessile dark red nodule with bleeding surrounded by shallow cuplike invagination of skin. Thus, histologic confirmation is necessary to differentiate it from other clinically similar tumors such as pyogenic granuloma, dermatofibroma, neurofibroma, seborrheic keratosis, bowenoid papulosis, leiomyoma, and some vascular tumors which can develop, erupt, or proliferate during pregnancy110. Histologic features indicate that the extending tumor downward into dermis which arises from lower portion of epidermis communicates with epidermis by broad bands of epithelial cells. It consists of solid masses of basaloid cells with deeply basophilic nucleus, having a cuboidal shape and a smaller size than that of normal keratinocytes. Significant amount of glycogen contained in the tumor cells is responsible for cytoplasmic clearing11. Also, dermoscopic patterns of eccrine poroma exhibit substantial discrepancy among cases, guaranteeing the necessity of histopathologic examination as a feasible diagnostic tool12.
The definite treatment of eccrine poroma is surgical excision13. Because of the possibility of recurrence, it is important to eliminate it completely, especially when the lesion is actively growing during pregnancy. In the present case a shave removal was possible because the lesion was pedunculated. In case of more superficial lesions, electrosurgical destruction can be tried to avoid an excessive invasive process14.
Herein, we experienced the fourth case of eccrine poroma which grew rapidly during pregnancy. The mechanism has not been elucidated yet, but this is considered to be an extremely rare phenomenon related to pregnancy.

 XML Download
XML Download