

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transverse dimensions of the dentofacial structures have been emphasized as an important factor in establishing and maintaining long-term stable occlusion.12345 Unfortunately, abnormalities of transverse dimensions are clinically masked and difficult to diagnose when they occur in combination with sagittal and vertical disharmonies. Therefore, clinical inspection of posterior crossbites or the use of study casts alone is inadequate for accurate assessment of malocclusion involving transverse discrepancy. It follows that a comprehensive orthodontic diagnosis should include transverse skeletal evaluation using posteroanterior cephalograms, which would aid in preventing potential relapse of treatment results.
However, most orthodontic records are still focused on the sagittal profile, and a majority of growth studies have focused on sagittal and vertical changes in facial dimensions using lateral cephalograms. Out of the few studies that have assessed transverse growth, subjects were followed longitudinally according to chronological age.678 However, chronological age alone is insufficient to identify the stages of developmental progression through adolescence to adulthood.91011 Evaluation of skeletal maturation can better incorporate individual variations associated with the timing and magnitude of growth.12 In a clinical setting, hand–wrist radiographs can be easily obtained along with other diagnostic radiographs and have been used as a reliable and efficient means of developmental assessment.1213
In orthodontic practice, norms of transverse dentofacial dimensions according to skeletal maturation stage would be beneficial in diagnosis and delivery of appropriate orthopedic treatment for growing patients with transverse discrepancies. Therefore, the purpose of this study was to establish the norms of dentofacial transverse dimensions according to the skeletal maturation stage in growing Korean individuals with skeletal Class I occlusion, assess gender difference and recognize correlations between the transverse variables.
MATERIALS AND METHODS
Patients who visited the Department of Orthodontics at Gangnam Severance Dental Hospital during years 2006 through 2016 for orthodontic consultations that had taken posteroanterior cephalograms and hand-wrist radiographs for diagnostic purposes were considered for this study. From these subjects, further cases were selected based on the following inclusion criteria; skeletal Class I occlusion cases with A point-Nasion-B point (ANB) angle ranging from 0° to 4°, minimal dental crowding of less than 3 mm, absence of dental spacing, absence of skeletal asymmetry and dental crossbites, and no history of previous orthodontic treatment. All the patients were of Korean descent and were aged between 7 and 19 years. This retrospective study was approved by the institutional review board of the Gangnam Severance Dental Hospital (No. 3-2016-0045).
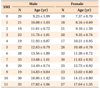
The subjects were categorized into 12 skeletal developmental stages (stage 0 to 11) according to Fishman's skeletal maturation index (SMI) by evaluating the hand–wrist radiographs.12 In this study, SMI stage 0 was defined as within 2 years of age before the subjects were screened as SMI stage 1. A total of 577 subjects (287 males, 290 females) were categorized into SMI stages and dentofacial transverse dimensions were evaluated. The mean age and number of subjects for each SMI stage are shown in Table 1.
All posteroanterior cephalograms were acquired using Planmeca ProMax (Planmeca, Helsinki, Finland). During radiologic exposure, the distance between the film to the porionic axis and the source of radiation was fixed to standardize magnification. All radiographs were taken by the same operator during the entire study period. The posteroanterior cephalograms were imported into V-ceph software (version 3.5; CyberMed Inc, Seoul, Korea). The magnification was adjusted and the ratio for all the posteroanterior cephalograms was maintained at 1.13. All landmarks were identified and transverse measurements were performed by this imaging program. The transverse measurements are shown in Figure 1. A total of seven linear measurements were obtained and one difference value and one ratio value were calculated (Table 2).
The hand–wrist radiographs were evaluated by a single orthodontist (K.H.K) with over 20 years of clinical experience in treating adolescent patients. The transverse skeletal measurements were measured by one investigator (Y.J.N), and intraexaminer reliability was determined by selecting 10 random subjects for each SMI stage (total, 120 radiographs) for a second measurement. The intraexaminer correlation coefficient indicated high reliability between the two measurements (r = 0.95 to 0.99). In addition, 10 subjects were randomly chosen per each SMI stage (total, 120 radiographs) and their posteroanterior radiographs were traced and measured by another examiner for the assessment of interexaminer reliability which showed high correlations as well (r = 0.90 to 0.96).
All data were analyzed using the SPSS software program, version 22.0 (IBM SPSS Statistics for Windows; IBM Co., Armonk, NY, USA). Descriptive statistics including means and standard deviations of the transverse measurements were calculated for each SMI stage in both sexes. Independent two-sample t-tests were used to evaluate statistical differences between males and females. Transverse changes with sequential increases in the SMI stage were analyzed using one-way ANOVA followed by post hoc Bonferroni correction. Pearson's correlation coefficients were used to determine correlations between the transverse measurements. A p-value of 0.05 or less was considered statistically significant.
RESULTS
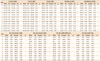
All seven transverse measurements were significantly affected by sex for most SMI stages. Males had significantly larger values than that of females in all SMI stages for facial, maxillary and mandibular width. Furthermore, males had significantly larger values for all seven transverse measurements at growth completion compared to that of females. The average maxillary and mandibular widths at growth completion were 73.58 mm and 95.75 mm, respectively, for males and 67.43 and 91.14 mm, respectively, for females (Table 2).
The maxillomandibular width difference at growth completion was 22.16 mm for males and 23.70 mm for females. This width difference was significantly larger in males at SMI 0 and 5. The maxillomandibular width ratio at growth completion was 77.01% for males and 74.06% for females. This width ratio was significantly larger in males at SMI 9 and 11 (Table 2).
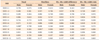
The subjects were evaluated for significant changes in the transverse maxillomandibular dimensions for every sequential increase in the SMI stage. The nasal and maxillary widths in males showed significant changes when the SMI stage progressed from 6 to 7. With regard to the maxillomandibular width difference and ratio, there were significant changes from stage 7 to stage 8 in males. No significant changes associated with SMI stage progression were observed in females (Table 3).
Cumulative growth percentages were calculated for all seven transverse measurements (Table 4). Cumulative growth of over 95% towards growth completion started in SMI stages 7 and 5 for facial width; stages 7 and 6 for nasal width; stages 4 and 1 for maxillary width; stages 5 and 6 for mandibular width in males and females, respectively.
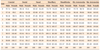
The maxillary and mandibular intermolar widths showed the strongest correlation for both sexes (r = 0.826 for males, r = 0.725 for females). The maxillary width and the maxillary intermolar width were also strongly correlated for both sexes (r = 0.671 for males and r = 0.724 for females). In males, there was also a strong correlation between the nasal and maxillary molar width (r = 0.663) as well as the facial and maxillary width (r = 0.642) (Table 5).
DISCUSSION
Diagnosis of transverse discrepancies by a combination of clinical and skeletal evaluations using posteroanterior cephalograms would be beneficial in preserving periodontal health during orthodontic treatment, which would eventually lead to favorable long-term stability.13 In adolescent patients, the timing of treatment is crucial with regard to the remaining growth of the craniofacial region. As there are variations of growth when patients are evaluated by chronological age, transverse skeletal norms according to the skeletal maturation stage will be useful for delivering timely and appropriate treatment.
In this study, dentofacial transverse development was evaluated according to Fishman's skeletal maturation stages. The mean age of subjects with each skeletal maturation stage closely matched the average chronological data presented by Fishman,13 with a difference within 1 year of age for males in every SMI stage and for females in SMI stages 5 to 11. Females in SMI stages 1 to 4 showed an age difference of less than 2 years compared to Fishman's data (Table 1).
The average cranial width at prepubertal stage (SMI 0–3) was more than 97% of the width at growth completion for both genders (Table 4). This was consistent with the findings of Scammon14 in that the cranial width followed the neural growth curve and reached near adult size by 6 years of age.
Facial width was greater for this study compared to previous growth studies.261516 Ricketts15 found facial widths to have an average value of 115.7 mm at age 9 years. Woods16 found facial widths to increase from 110.5 mm to 124.7 mm in males and 107.8 mm to 120.6 mm in females between 7 to 15 years of age. The facial width for this study were 131.78 mm for males and 125.28 mm for females at SMI 0 which increased to 147.80 mm and 136.77 mm at growth completion, respectively. The mean facial width for Korean subjects was greater than that reported for Chinese or Japanese subjects, who have been compared with American Caucasian subjects for their wide zygomatic widths, by approximately 15 to 19 mm.1718 Nevertheless, the average facial width for Korean subjects was within the range reported of Japanese subjects by Enoki et al.17 The results of this study can reasonably imply that Korean subjects have relatively pronounced zygomatic widths compared with American Caucasian subjects.
The average nasal width of this study at SMI 0 was greater by more than 3 mm compared to studies that report a mean nasal width of about 23 mm at age 6 years and 25 mm at age 9 years.215 As a result of an approximate growth of 0.5 mm per year, the average nasal width at SMI 11 was 33.10 mm for males and 31.28 mm for females; these values were also greater than those reported in previously mentioned studies. However, the final nasal widths were comparable to those in a study of Chinese subjects by Wei,18 which reported a width of 32.8 mm for males and 30.4 mm for females.
The maxillary width at SMI stage 7 for boys and SMI stage 3 for girls reached over 99% of the width at growth completion (Table 4). This result coincided with a previous study in that males reached growth completion about 3 years later than females.19 However, the absolute time of growth completion was earlier than that in previous studies, which reported that the maxillary width increased up to 13 to 15 years of age in females and beyond 18 years of age in males.27192021 The difference in time of growth completion can be attributed to individual growth variation which was inevitably included in this cross sectional study. According to the findings of our study, growth of the maxillary width was about 95% to 96% complete at SMI stages 4 to 6 (age 12 to 14 years) in males and SMI stages 1 to 2 (age 8 to 10 years) in females which may be used as a timeline for including maxillary expansion earlier than this time (Table 4). The average maxillary widths at growth completion were also greater than previous growth studies carried out in the North American regions.2722
For evaluation of the mandibular width, the bilateral antegonial notches were used because they reportedly remain unchanged by muscle attachments.815 The mandibular width showed continuous growth close to SMI stage 11 in both sexes; this was in accordance with the findings in previous studies showing that the mandible continued to increase in transverse dimensions at 18 years of age.2719 Ricketts15 reported a mean antegonial width of 76.1 mm at 9 years, with an incremental increase of 1.4 mm per year. Athanasiou et al.23 found an increase of 12.1 mm in the antegonial width from 7 to 15 years of age, while Lux et al.8 showed a 11.2 mm increase in males and a 9.9 mm increase in females. In this study, the mean mandibular width at SMI stage 0 was 86.90 mm for males and 80.68 mm for females; both values were larger than those reported in previous studies.81523 Even though the amount of increase in width until growth completion was 8.85 mm in males and 10.46 mm in females, which was comparable to that in previous studies, the final mandibular width was greater than that in the aforementioned reports. This is in accordance with the findings of studies that included Chinese and Japanese subjects, whose bigonial widths considerably exceeded those of American Caucasian subjects.18 It is reasonable to infer that Korean subjects, in addition to Chinese and Japanese subjects, have wider faces compared with American Caucasian subjects.
In a study by Betts et al.,3 age-appropriate-expected maxillomandibular difference values were presented and are used for comparisons with actual maxillomandibular measurements during the evaluation of transverse skeletal discrepancies. A difference of less than 5 mm from this index is recommended for orthodontic/orthopedic expansion, and a difference of more than 5 mm is indicative of surgically assisted expansion to correct transverse skeletal problems. However, the maxillomandibular width difference at all SMI stages in the current study showed greater values compared with the age-appropriate-expected values in the aforementioned report, and some differences even exceeded the 5 mm standard used for surgical intervention. Considering the fact that this study included subjects in normal Skeletal Class I occlusion without skeletal asymmetry or dental crossbites, the age-appropriate-expected maxillomandibular transverse differential index13 should not be applied to Korean subjects during the treatment planning phase, as variations of craniofacial morphology between different populations have been reported.2425
The maxillomandibular width ratio was evaluated in order to minimize radiographic enlargement factors at different ages, which could affect the mandible more than the maxilla due to its larger size.7 A previous study by Cortella et al.7 reported a maxillomandibular width ratio of 78.6% at 6 years of age, which decreased to 74.9% at 18 years of age. Athanasiou et al.23 showed a width ratio of 77.8% at 6 years of age and 74% at 15 years of age. Similar values of 77.77% for males and 78.83% for females at SMI stage 0 were obtained in the present study. At SMI stage 11, the ratio was 77.01% for males and 74.06% for females which also decreased according to growth. A decrease in this ratio, however, was not detrimental to the long-term prognosis of posterior occlusion, as the results of this study showed a tendency of increase in maxillary intermolar width and decrease in mandibular intermolar width in females, similar to the results of previous studies by Woods16 and Snodell et al.2 However, the decrease in the mandibular intermolar width in males was not pronounced which may be due to the individual variations of subjects included. Despite the limitations of this cross-sectional study, the tendency for change in the molar width in females explains the maintenance of proper posterior occlusion even though greater skeletal transverse growth was observed in the mandible relative to the maxilla. A compensatory mechanism had occurred in the mandibular molars to adapt to the width of the maxillary molars which resulted in normal occlusion.726
As for gender differences, males showed significantly greater transverse values for facial, maxillary and mandibular width in all SMI stages compared to females. All seven transverse measurements resulted in significantly greater values at growth completion for males as well. This is in accordance with the findings of previous studies that showed a significant difference of transverse width in most ages between genders.82728 Although the maxillomandibular width ratio was greater in males at SMI stage 11 compared to that of females, the maxillomandibular intermolar width ratio did not show significant difference which suggests posterior occlusion at growth completion should not be affected by gender.
In order to overcome the limitations associated with the cross-sectional study design, the subjects were grouped into prepubertal (SMI stages 0–3), pubertal (SMI stages 4–7), and postpubertal (SMI stage 8–11) groups. The average values for the maxillomandibular width difference, which was the key variable in this study, were assessed for each group. There was a significant difference between pubertal and postpubertal stages for both sexes. This suggests that the maxillomandibular width difference continued to increase substantially during the postpubertal stage. This is in accordance with a study by Gandini and Buschang29 in that the maxillary and mandibular basal structures increased during late adolescence.
The maxillary and mandibular intermolar widths showed the strongest correlation compared with other variables for both sexes (r = 0.826 for males, r = 0.725 for females). The maxillary width and the maxillary intermolar width also showed a strong correlation in both sexes (r = 0.671 for males and 0.724 for females). These correlations were consistent with those reported in a study by Snodell et al.2 However, there was a moderate correlation between the mandibular width and the mandibular intermolar width for males (r = 0.506) and these parameters did not show correlations in females. A lower correlation between mandibular width and mandibular intermolar width could be due to a decrease in mandibular intermolar width that occurred in order to adapt to the width of the maxillary intermolar to obtain good posterior occlusion.
Accurate evaluations with posteroanterior cephalograms have been controversial as 3-dimensional structures are overlapped into a 2-dimensional (2D) image. Current studies are investigating cone-beam computed tomography (CBCT) images for diagnostic superiority over the conventional 2D imaging using posteroanterior radiographs.30 However, the use of CBCT as a standard diagnostic tool for growing patients may face ethical challenges associated with unnecessary radiation exposure. Furthermore, the cross-sectional design of our study and the assessment of subjects in a one-time frame inevitably included individual growth variations that should be considered during interpretation of descriptive data and comparisons between consecutive SMI stages. Even though the subjects were categorized into each skeletal maturation stage to minimize the magnitude of growth variations by chronological age, further studies including longitudinal data would be needed. Nonetheless, the results may serve as a guideline of dentofacial width development in Korean adolescents of good occlusion according to skeletal maturation.
CONCLUSION
Dentofacial transverse norms of Korean adolescent subjects in Class I normal occlusion were established according to skeletal maturation stages. Facial, maxillary and mandibular widths were significantly greater in males during all growth stages and all dentofacial width measurements were significantly greater in males at growth completion. Maxillary and mandibular intermolar widths were strongly correlated for both genders. Maxillomandibular width difference values may be greater for Korean adolescents compared to Caucasians. This study may be useful as a guide for dentofacial transverse growth of Korean adolescents in good occlusion according to skeletal maturation.


 XML Download
XML Download