

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Orthodontic microimplants (OMIs) have become popular anchorage tools in the field of orthodontics. Therefore, information on factors that determine their success and failure is useful for clinicians. Many studies have considered the factors affecting the success rate of OMIs using cone-beam computed tomography (CBCT)12345678 and standard two-dimensional (2D) radiography,6910 although we believe that panoramic radiographs (PRs) are superior to these modalities for several reasons.
Compared with PRs, CBCT images can provide more accurate information regarding features such as root resorption, tooth position, and pathology111213; however, PRs exhibit an acceptable reliability with lesser radiation exposure and a lower cost compared with CBCT.1415 Furthermore, PRs are readily available because they are commonly and consistently used for assessment of the oral cavity with regard to normal anatomical structures and oral pathologies.161718
The reliability of PRs with regard to accurate depiction of the angularity and position of teeth remains controversial. Studies have shown that distortion can influence these parameters on PRs.192021 However, Bennemann et al.14 demonstrated that PRs allowed for a rough evaluation of OMIs in relation to the surrounding structures, while Schnelle et al.10 found that the positioning error was negligible and that comparisons could be made between PRs.
Many studies19222324 have suggested that the unreliability of their results could be attributed to inaccurate head positioning at the time of exposure. Therefore, if the head position is carefully adjusted, structures can be accurately measured on PRs, and it could be possible to identify the accurate location and angulation of OMIs on these 2D radiographs. In the present study, we investigated factors influencing the success rate of OMIs, including the OMI position and angulation, using PRs.
MATERIALS AND METHODS
We performed a power analysis using G*Power (version 3.1.9.2: Franz Faul, Christian-Albrechts-Universitat, Kiel, Germany) to determine the sample size required for this study. A two-fold increase in the success rate (odds ratio [OR], 2) was considered to be clinically meaningful. We found that, to detect OR of 2, 104 radiographs would provide a power of 0.87 and a two-tailed alpha value of 0.05.
Our final sample comprised PRs of 80 consecutive orthodontic patients with a good periodontal status (29 men, 51 women; mean age, 17.95 years; standard deviation, 6.13 years; age range, 11–41 years) who underwent bilateral OMI insertion (n = 160) in the maxillary buccal alveolar bone at the Department of Orthodontics, Wonkwang University Daejeon Hospital between March 2007 and December 2010. The institutional review board of Wonkwang University Daejeon Dental Hospital (No. WKD IRB W1603/001-001) approved the study.
A total of 160 OMIs (diameter, 1.2–1.3 mm; length, 8 mm; implant type, AbsoAnchor SH1312-08 [self-drilling and tapered]; material, titanium alloy; surface characteristic, untreated; Dentos, Daegu, Korea) were implanted in the maxillary buccal bone between the second premolars and first molars as anchorage devices for retraction of the anterior teeth. Before implantation, all patients provided informed consent after receiving explanations regarding the advantages and disadvantages of this procedure. OMIs were inserted into the attached gingiva just adjacent to the mucogingival junction, at the midpoint between the roots of the adjacent teeth, and immediately loaded with orthodontic forces of approximately 50 to 200 g using elastic chains.25 All OMIs were directly placed by two right-handed operators (K.I.M. and J.M.C.) using a hand driver with the self-drilling method under local anesthesia. The patients agreed to the acquisition of PRs after OMI placement.
PRs were acquired using an X-ray imaging machine (Planmeca Promax; Planmeca OY, Helsinki, Finland), with the same distance between the film and the X-ray tube, beam angulation, film size, and exposure time for all patients. The head position of patients was maintained by positioning the chin rest and bite guide. Images were acquired by the same radiologist for all patients to increase reproducibility. The optimal image density and contrast were achieved at exposure settings of 84 kVp, 16 mA, and 16 seconds. The magnification factor was 1.20. PR data were saved in Digital Imaging and Communications in Medicine (DICOM) files, and imaging software (V-Ceph, version 6.0; Osstem, Seoul, Korea) was used to analyze the DICOM data to establish reference lines and generate quantitative measurements (Figure 1).
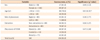
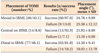
Treatment success was defined by the retention of OMIs as appropriate anchors in the alveolar bone for at least 1 year during the orthodontic treatment.123 The relationship of the OMI success rate with age, sex, side of placement (right or left), extraction or nonextraction treatment, and position of the tip of OMI (TOMI) was analyzed. To assess the effects of age on the success rate, the patients were divided into two age groups (Table 1)123: < 20 years (11–19 years; n = 56; 112 OMIs) and ≥ 20 years (20–41 years; n = 24; 48 OMIs).
For the measurements recorded by one investigator (J.M.C.), the horizontal occlusal plane of the posterior teeth was established through the cusps of the second premolar and first molar. Figure 2 shows the reference lines and points (left) and the linear and angular measurements (right). To test the repeatability of measurements, 20 patients were randomly re-evaluated 2 weeks after the initial measurements. Intraclass correlation coefficients for these analyses ranged from 0.77 to 0.99, indicating excellent reliability.
Statistical analysis
Descriptive statistics are reported as means (standard deviations) or numbers (percentages), where appropriate. Logistic regression analysis was performed to evaluate the association between PR measurements and OMI success. Univariate logistic analyses were performed and crude ORs calculated for the association between each predictor variable and OMI success. Then, predictors that were significantly associated with OMI success (p ≤ 0.10) were included in simultaneous logistic regression analysis to evaluate their unique (adjusted) association with OMI success. Pearson's correlation coefficients were also calculated for the relationship between the placement angle and other predictors. IBM SPSS Statistics software (version 22.0; IBM, Armonk, NY, USA) was used for all statistical analyses. A two-tailed p-value of < 0.05 was considered statistically significant.
RESULTS
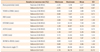
The overall OMI success rate was 85.0% (136 of 160 OMIs). The success rate was higher for the ≥ 20-year group than for the < 20-year group, for OMIs placed on the left than for those placed on the right, for women than for men, for extraction group than for nonextraction group, and for OMIs with tips placed on interradicular midline (IRML; central) than for those with tips placed mesial or distal to IRML. However, these differences were statistically significant only in association with age (Table 1). The highest success rate was observed with the central position of TOMI (92.9%), followed by the mesial (87.0%) and distal (81.8%) positions. Table 2 shows the mean values and standard deviations for root proximity and other measurements according to the success or failure of OMIs.
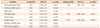
Logistic regression analyses were performed to evaluate the association between the PR measurements and OMI success. Univariate analysis (Table 3, crude ORs) revealed that the placement height of OMI (HTOMI; OR, 1.53; 95% confidence interval [CI], 1.18 to 1.97) and the length of OMI (LOMI; OR, 1.81; 95% CI, 1.29 to 2.54) were significantly associated with OMI success (p = 0.001). Root proximity was not significantly associated with success (p = 0.073), although it fulfilled the criterion for entry into the simultaneous analyses (p ≤ 0.10). The coefficients for both HTOMI and LOMI indicated that the probability of success would increase with an increase in their values. A 1.0-mm increase in HTOMI increased the odds of success by 1.53, while a 1.0-mm increase in LOMI increased the odds of success by 1.81. When the three predictors that met the criteria for inclusion in the simultaneous regression analyses were evaluated (Table 3, adjusted ORs), only LOMI was found to be statistically significant (OR, 1.57; 95% CI, 1.05 to 2.35; p = 0.027). The fact that HTOMI was no longer significant when analyzed with LOMI suggested that, although LOMI and HTOMI were both predictive of OMI success, LOMI was the stronger predictor.
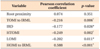
Pearson's correlation analysis revealed that the distance between the head of OMI (HOMI) and IRML (HOMI to IRML) increased with an increase in the placement angle, with highly significant (positive) correlations between the two parameters (p < 0.001). On the other hand, the distance between TOMI and IRML, the interradicular distance (IRD), HTOMI, and LOMI showed significant negative correlations with the placement angle (p < 0.05). The correlation between the placement angle and root proximity showed no statistical significance (p > 0.05; Table 4).
DISCUSSION
In the present study, we investigated factors influencing the success rate of OMIs, including the OMI position and angulation, using PRs. The results indicated that LOMI and HTOMI were significant predictors of OMI success. Moreover, the OMI success rate was significantly higher for patients aged ≥ 20 years than for those aged < 20 years.
Although absolute anchorage devices such as OMIs have been widely used to enhance the quality of orthodontic treatment for several decades, their clinical performance and the crucial factors affecting their success rate are not well known. Therefore, many orthodontists have tried to identify factors that affect the success rate of OMIs. Various studies have attempted to determine the influence of various factors, including sex, age, side of placement, clinical proficiency, cortical bone thickness, placement angle, root proximity, bone density, bone stress, sinus pneumatization, skeletal pattern, extraction or nonextraction treatment, surgical procedure, thread surface treatment, mechanical properties, patient care, placement torque, placement site, position, smoking, systemic disease, and orthodontic force, on the success rate of OMIs using radiography and clinical examinations.123456789102627 However, there are few studies using PRs.
PRs are frequently used to visualize root parallelism and mesiodistal tooth angulation for orthodontic treatment.282930 However, methodological errors typical of 2D evaluations cannot be ruled out, which is a limitation of the present study. Vertical and horizontal magnifications and distortion of angulation are inherent disadvantages of PRs.192021 Nevertheless, several authors have suggested that accurate linear and angular measurements can be obtained if the head position is accurately adjusted during exposure.1015222324 Bennemann et al.14 also reported that PRs enabled a rough evaluation of the miniscrew position in relation to the surrounding structures without the higher levels of radiation exposure associated with CBCT.
A commonly preferred site for OMI placement is the bone between the maxillary second premolar and first molar because of the lower root proximity, easy accessibility for various orthodontic mechanics, and easy placement surgery.12369 In the present study, we examined only OMIs placed in the maxillary buccal alveolar bone between the second premolar and first molar, although further studies are planned to investigate OMIs placed in the mandibular buccal alveolar bone between the first and second molars.
We obtained PRs after simultaneous placement of OMIs in the maxillary buccal alveolar bone between the maxillary second premolar and first molar on the right and left sides. To obtain high reliability, PRs were acquired by the same radiologist under the same conditions. Linear and angular measurements as well as the position of OMIs were evaluated using imaging software.
The OMI success rate was significantly higher for patients aged ≥ 20 years than for those aged < 20 years in the present study; this finding was similar to that in a previous study.31 This difference can be attributed to the thin cortical bone and poor bone quality in the younger patients. Moreover, in agreement with previous studies, we found that the success rate was higher for women than for men, for OMIs placed on the left than on the right, and for patients with extraction treatment than for those with nonextraction treatment, although the differences were not statistically significant.1235 Lim et al.5 concluded that the clinician's experience did not generally affect the success of OMI stability; therefore, we disregarded the clinical proficiency of the two operators as a factor for evaluating the success rate.
Joo6 used the interlamina dura distance to measure the IRD, whereas Kim et al.7 used the root surface as the standard for improving consistency, because the root surface can be observed more clearly on PRs. Therefore, for improved accuracy and reproducibility, we used the root surface for the measurement of root proximity to OMIs. In the present study, root proximity was not significantly associated with the OMI success rate, which is inconsistent with the findings of CBCT studies.129 This inconsistency may be attributed to differences in methods for measuring root proximity.
Some authors have used the tooth axis for measuring the angle.430 In the present study, the horizontal placement angle was measured with IRML as the standard. We believe that IRML is a more accurate standard compared with the tooth axis because it is generally used as a guideline during OMI insertion.
The OMI success rate in our study was the highest when TOMI was centrally positioned, i.e., on IRML, and it was higher with the mesial position for TOMI (mesial to IRML) than with the distal position for TOMI (distal to IRML; Table 5).2 This difference probably occurred because of root proximity and stronger masticatory forces on distally placed tips than on mesially placed tips.
In the present study, univariate analyses indicated that the OMI success rate would increase with an increase in LOMI and HTOMI on PRs, although simultaneous analyses did not find HTOMI to be a significant factor for success (Table 3). This could be a result of the difference in the alveolar crest height according to periodontal status. Further studies should investigate HTOMI using the occlusal plane or cementoenamel junction (CEJ) as a reference instead of the alveolar crest.67
Nevertheless, some of our cases did not exhibit an association between OMI success and LOMI. Therefore, to maximize the success of OMIs, clinicians should consider all potential factors that could affect the probability of success. We also found a significant correlation between the placement angle and LOMI and HTOMI (Table 4), although we could not evaluate the correlation between the vertical placement angle and LOMI because of limitations inherent to PRs. Sinus invasion by OMIs, distal angulation of TOMI, and a sloping alveolar crest were not included as factors influencing OMI success because of their rarity.
Root proximity has been considered the most significant factor affecting the success rate of OMIs in studies using dental radiographs and CBCT.1289 The authors found that titanium screws appearing close to the root on CT images also appeared close to the root on dental radiographs; accordingly, they suggested that 2D dental radiographs should suffice for the evaluation of root proximity.9 However, in the present study, root proximity was not a significant predictor of OMI success, although the success rate increased as the distance between OMI and the root surface increased. This could be due to the difference in linear accuracy between 2D radiographs and CBCT.914192021222324
In the present study, PRs were used to evaluate linear and angular measurements for OMIs. PRs offer the inherent disadvantage of methodological errors.192021 Although evaluations using CBCT may be more accurate, PRs can be easily and rapidly acquired, are economic and convenient, provide a good overview of the entire dentition along with its surrounding structures, and result in lesser radiation exposure compared with CBCT. In addition, the validity of PRs with regard to the accuracy of linear and angular measurements has been reported.2223 Therefore, PRs can be considered useful tools for the assessment of OMI positioning and success.
Periapical radiographs are also commonly used to investigate hard tissues in the dentoalveolar region, with advantages and limitations similar to those of PRs. However, they exhibit less inherent magnification compared with PRs.32 In the present study, OMIs were simultaneously placed on both sides of the maxillary buccal alveolar bone. Therefore, we consider that PRs were a better option than periapical radiographs because they permitted the comparison of both sides in a single frame.
This study was limited to the maxillary posterior region, and further studies should evaluate OMI placement in all suitable areas, such as the palatal slope and mandible, using PRs and periapical radiographs.
CONCLUSION
We recorded two principal findings in the present study based on PRs. First, the OMI success rate increased with an increase in LOMI and HTOMI and exhibited a statistically significant association with these two parameters. The findings suggested that the OMI success rate increased when the microimplants were positioned more apically and with a lesser angulation. Second, the OMI success rate was significantly higher for adults than for adolescents.


 XML Download
XML Download