

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Subungual melanoma (SUM) is a malignant neoplasm of melanocytes that arises from the nail matrix. In the early phase of SUM, it usually presents as longitudinal brown or black band on nail plate (melanonychia), and can be misdiagnosed as benign nail pigmentation disorders such as nail matrix nevi or subungual lentigo123. Although SUM is rarely diagnosed in Caucasian, the prevalence in Asian population is relatively high. In a retrospective study in Japanese population, SUM accounted for approximately 10% of cutaneous melanoma3. According to our data in a single tertiary institute, SUM constitutes about 18% of cutaneous melanoma in Korea4. Prognosis of SUM was generally poor in the past, because the diagnosis was frequently delayed. One of the most common causes of delay in SUM diagnosis is lack of early recognition5. Although an “ABCDEF rule” for early clinical detection of SUM had been proposed6 and it seems to be useful, the 6 features of this criterion, particularly the “family history of melanoma or dysplastic nevus syndrome,” are not always observed in cases of SUM in situ.
The aim of our study is to suggest simple clinical strategy for SUM in situ for early clinical detection by analyzing clinical features of 8 cases of SUM in situ.
Go to : 
MATERIALS AND METHODS
After receiving approval from the institutional review board of Samsung Medical Center (IRB no. 2016-08-187-001), 8 cases of SUM in situ diagnosed at the Samsung Medical Center from January 2015 to September 2016 were identified and retrospectively reviewed. Histopathology slides, clinical records, and clinical photographs of the cases were included. Data gathered from the electronic medical record included gender, age, age of onset, location of the lesion, clinical features including pattern of melanonychia, presence of periungual pigmentation (Hutchinson's sign) and nail deformity, biopsy and surgical method, and pathological information.
All patients underwent nail matrix biopsy. After local anesthesia with 2% lidocaine, nail plate was extracted and about 5 mm longitudinal incisions were made at both ends of the proximal nail fold to expose nail matrix. Nail matrix specimens were obtained at nail matrix with the darkest pigmentation or nail matrix corresponding to the darkest band on nail plate by 3 different methods: 3 mm punch biopsy; longitudinal incision from nail matrix to hyponychium; or transverse shave biopsy (similar to the tangential excision of nail matrix described in literatures78, but matrix was shaved after nail plate extraction). Wide excision of nail unit was performed in all cases. Pathological diagnosis of SUM in situ was based on our previous investigation of histological findings of SUM in situ: diagnosis of SUM in situ was made if increased number of scattered atypical melanocytes with large hyperchromatic nuclei were observed in nail matrix without evidence of dermal invasion in the excision specimen.
Go to :
RESULTS
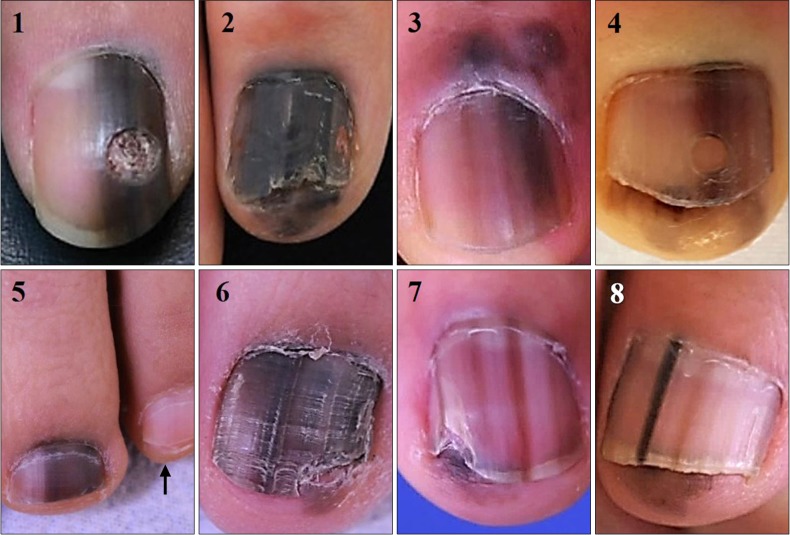
Of the 8 cases of SUM in situ, 3 (37.5%) cases were male and 5 (62.5%) were female. The age at diagnosis ranged from 30 to 70 years (mean age, 56.3 years). The duration of pigmentation ranged from 6 months to 16 years (mean duration, 6.3 years). The thumb (25%) and big toe (12.5%) were most commonly affected. All cases were presented as longitudinal melanonychia in a single digit (Fig. 1). Colors of melanonychia striata were black, dark brown, or tan. Besides, entire nail plate was faintly or darkly pigmented (i.e., total melanonychia) in all cases, exhibiting homogeneously black (1 case) or variegated shades of tan or brown (7 cases). Periungual pigmentations on hyponychium or proximal nail fold were found in 7 (87.5%). In short, all patients were older than 18 and had solitary melanonychia with brown background pigmentation or periungual pigmentation. Nail plates in 2 patients (Fig. 1; cases 2 and 6) had deformity ahead of nail matrix biopsy, presumably due to the effect of melanoma. Nail dystrophy in 3 cases (Fig. 1; cases 1, 4, and 7) were caused by previous nail matrix biopsy before visiting us. Three-millimeter punch biopsy was performed in 5 patients. Longitudinal incision and nail matrix shave biopsy were used in remaining 2 (cases 2 and 3) and 1 (case 5) patients, respectively. All patients received wide excision with distant free flap or full-thickness skin graft; no evidence of dermal invasion was found in all cases. Clinical findings, method of biopsy, and surgical procedures that patients received are summarized in Table 1.
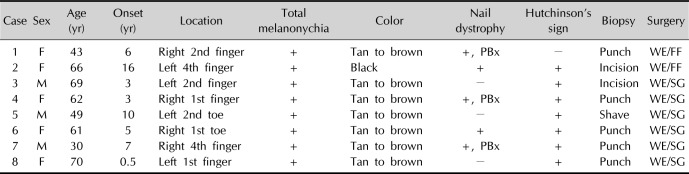
 | Fig 1Clinical photographs of 8 subungual melanoma in situ cases. Note all cases have entirely pigmented nail plate compared to unaffected ones (arrow in case 5). Hutchinson's sign was observed except for case 1. Cases 2 and 6 had nail deformity ahead of nail matrix biopsy.
|
Table 1
Clinical features, method of biopsy, and surgical management in 8 cases
![]()
Go to :
DISCUSSION
Amputation of affected phalanx was performed for the surgical management of SUM in situ in the past, but several recent literatures advocated the phalangeal bone conserving surgery in early stage91011. Therefore, early detection and diagnosis of SUM is important because it can improve quality of life as well as 5-year survival rate. Our study provides a clinical screening tool for SUM in situ. In 1989, Saida and Ohshima3 described 5 clinical features of SUM in situ: noticed after middle age; pigmented band broader than 6 mm; brownish band with shades of tan to black; Hutchinson's sign; and slight degree of nail deformity. Levit et al.6 reviewed this and other literatures to propose the “ABCDEF” mnemonic for SUM: “A” stands for age, ranged from 20 to 90 years in Asian or African-American race; “B” stands for pigmented black-brown band with breadth wider than 3 mm; “C” stands for rapid change in nail band or lack of change in nail dystrophy despite appropriate treatment; “D” stands for digit, namely, most commonly in thumb of dominant hand; “E” stands for extension of pigmentation on periungual skin; “F” stands for family or personal history of dysplastic nevus syndrome or melanoma. Although this mnemonic seems to be useful, items need to be added or corrected for SUM in situ. First, all patients were adults (i.e., older than 18 years). Previous ABCDEF rule specified the range of age, but we simplified “A” as “adult age”. All of 18 cases of SUM in situ in our previous study were adults as well4. In addition, all of our cases had faint to dark background pigmentation in entire nail plate. Cases 1, 3, 4, 5, and 8 might be confused with partial melanonychia, but background pigmentation adjacent to the dark band was identified by comparing with unaffected opposite finger/toe or adjacent fingers/toes (Fig. 1, arrow in case 5). Thus, we suggest that “dark brown bands in brown background” is a characteristic of SUM in situ, adding background pigmentation to “B” of previous ABCDEF rule. We recommend clinical photograph should include all 10 fingers or toes for correct description of lesion. Background pigmentation can differentiate benign nail pigmentation disorder from SUM in situ as well. In our previous study, 18 SUM in situ were included. Fourteen out of 18 (77.8%) SUM in situ had entirely pigmented nail plate4. On the other hand, in our clinicopathological analysis of 28 nail matrix nevus (NMN) cases (not published), all except for 2 total melanonychia cases exhibited sharp band margin and normal colored nail plate adjacent to the lesion. Two total melanonychia cases were children. Moreover, in another study on NMN, there were adult cases with band breadth wider than two thirds of affected nail12. Therefore, background pigmentation is more appropriate clinical criterion than specified band breadth for SUM in situ. The information on change in nail band or treatment response of nail dystrophy at initial visit may be incorrect, because we have to rely on patient's memory. In addition, nail dystrophy is not frequently accompanied with SUM in situ. Only about 25% of our case and 16.7% of our previous cases had nail dystrophy. In tertiary center setting, patients occasionally underwent nail unit biopsy already, and we cannot be sure that the nail dystrophy was occurred by melanoma or biopsy. Therefore, change in nail band or nail deformity may not be an appropriate item for clinical checklist when we initially examine the lesion suspected as SUM in situ. “D” and “F” in the rule are only ancillary items. SUM should be suspected if a patient is adult and has melanonychia striata with background pigmentation whether “D” and “F” are satisfied or not. Moreover, more than half of our cases had lesion on digits other than thumbs or big toes and none of our cases had family or personal history of melanoma or dysplastic nevus syndrome. Levit et al.6 commented that periungual pigmentation is usually late presenting sign of SUM, and not suitable for early detection of SUM although they included Hutchinson's sign in the ABCDEF rule. However, nearly 90% of our case showed Hutchinson's sign in spite of SUM in situ. Eleven of 18 (61.1%) SUM in situ in our previous study had Hutchinson's sign on periungual skin, but only 1 pediatric NMN had hyponychial pigmentation4. Hyponychial pigmentation in 1 NMN case can be one of the atypical features found in pediatric NMNs12. Periungual extension of pigmentation can happen before dermal invasion because radial growth phase usually precedes vertical growth except for nodular melanomas. In a previous case series of 9 acral lentiginous melanoma in situ, mean duration of radial growth phase was 9.4 years13. Three of them were SUM in situ, and Hutchinson's sign was identified in two cases. We suggest “color in periungual skin” or “C” as the third rule. Finally, all 26 cases in this and our previous investigation had solitary lesion, namely, only 1 digit was affected. Multiple melanonychia is usually caused by benign disorders that can manifest as nail pigmentation, such as Laugier-Hunziker syndrome1415 or Peutz-Jeghers syndrome16. Although there was one case report on multiple primary SUM in 3 fingers, it was very exceptional and 3 lesions appeared sequentially, not at the same time17. Therefore, SUM in situ involves only one digit except for very rare cases. We suggest “single digit lesion” or “D” as the last rule.
In summary, based on 8 cases and our previous SUM in situ cases, nail “ABCD” for SUM in situ is as followed: “A” stands for adult age; “B” stands for brown bands with brown background; “C” stands for color in the periungual skin; and “D” stands for single digit lesion. We propose a clinical strategy for screening SUM in situ; suspect SUM in situ if solitary (“D”) longitudinal melanonychia in adult (“A”) was satisfying either “B” and/or “C” in ABCD. Seventeen out of 18 SUM in situ satisfied ABCD rule, whereas none of the benign lesions fulfilled it4. As aforementioned above, none of 28 NMN cases (unpublished cases) satisfied nail ABCD rule. Therefore, sensitivity and specificity of nail ABCD rule were 100% and 96.6%, respectively.
The limitation of our study is small sample size, but all 8 cases satisfied ABCD rule. Furthermore, this strategy can be applied to our previous 18 SUM in situ.
Based on current data, we believe our nail ABCD rule is a simple, sensitive, and specific clinical tool for screening SUM in situ. For accurate documentation of lesion, we recommend clinical photography including whole 10 fingers or toes. Further refinement of this clinical criteria based on larger sample size is necessary to facilitate early recognition of SUM in situ.
Go to :
 XML Download
XML Download