

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
MATERIALS AND METHODS
Subjects
Methods
Measurement of cytokine levels
Assessments of therapeutic effects and adverse events
Assessment of changes in cytokine levels
Statistical analysis
RESULTS
Demographic data
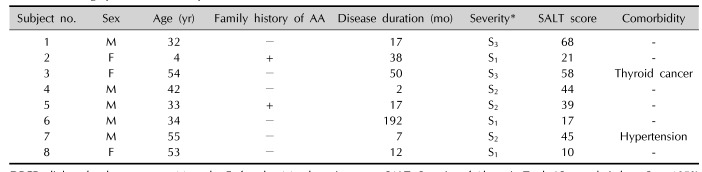
Table 1
Demographic data of the patients treated with DPCP
![]()
Objective assessment
 | Fig. 1Gross photograph of patient no. 3 (responder) and patient no. 7 (non-responder) at before and 4 months after DPCP treatment. Before treatment (A, E: patient no. 3; C, G: patient no. 7). After 4 months of treatment (B, F: patient no. 3; D, H: patient no. 7).
|
Table 2
Summary of clinical results of the patients treated with DPCP
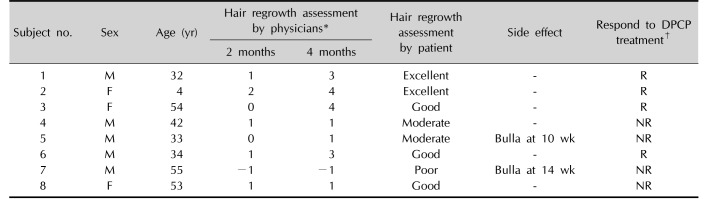
DPCP: diphenylcyclopropenone, M: male, F: female, R: responder, NR: non-responder. *−1=spreading, 0=no hair growth, 1=1%~24% hair growth, 2=25%~49% hair growth, 3=50%~74% hair growth, 4=75%~99% hair growth, 5=100% hair growth. †Responder: hair regrowth assessment score ≥3 (hair regrowth ≥50%) at 4 months after DPCP treatment, non-responder: hair regrowth assessment score <3 (hair regrowth <50%) at 4 months after DPCP treatment.
![]()
Subjective satisfaction assessment
Adverse events assessments
Changes in cytokine levels
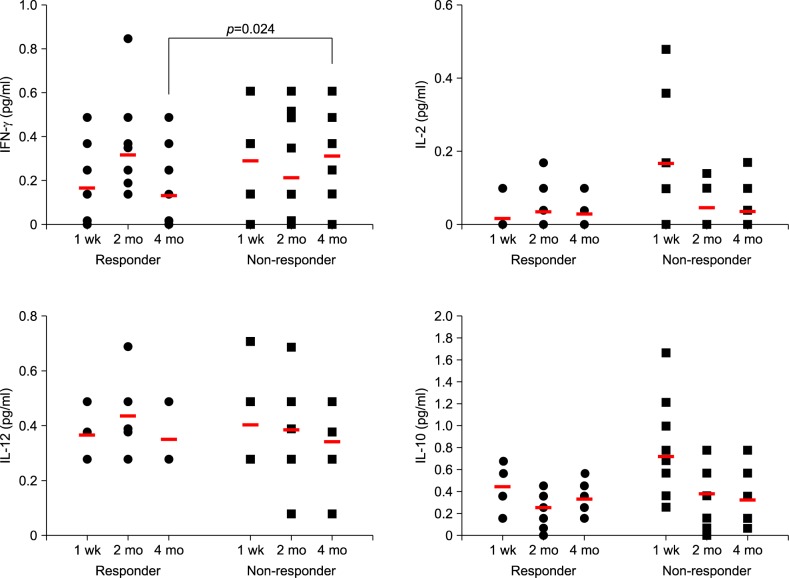 | Fig. 2Dot plot showing each value of cytokines in the patients treated with diphenylcyclopropenone (DPCP). Red bar in the graph indicates mean values. Before significant clinical differences appear (1 week and 2 months after treatment), interferon (IFN)-gamma, interleukin (IL)-12, and IL-10 showed no significant difference between responders and non-responders. IL-2 levels at 1 week showed difference between the two groups, however, it did not showed difference at 4 months after treatment. IFN-gamma levels at 4 months after DPCP treatment showed statistically significant differences between responder and non-responder groups (p=0.024).
|
Table 3
Comparison of the cytokine levels between responder and non-responder groups at 1 week, 2 months, and 4 months
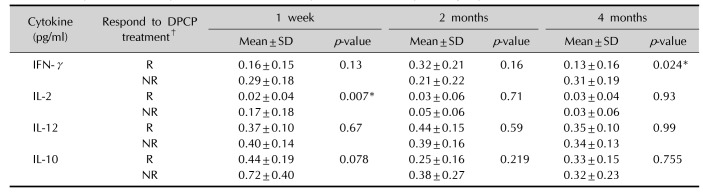
Values are presented as mean±standard deviation (SD) for n=4 of the three independent experiments. DPCP: diphenylcyclopropenone, IFN: interferon, IL: interleukin, R: responder (n=4), NR: non-responder (n=4). *p<0.05 calculated by Mann-Whitney U-test between responder and non-responder groups. †Responder: hair regrowth assessment score ≥3 (hair regrowth ≥50%) at 4 months after DPCP treatment, non-responder: hair regrowth assessment score <3 (hair regrowth <50%) at 4 months after DPCP treatment.
![]()
Table 4
Comparison of the differences of cytokine levels in each group after DPCP treatment
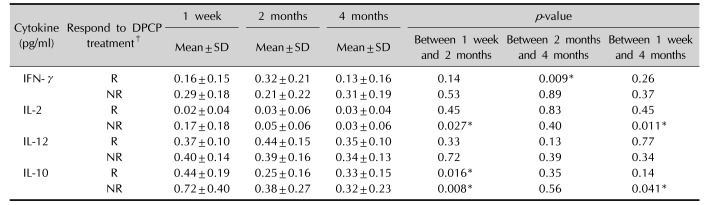
Values are presented as mean±standard deviation (SD) of changes between each time intervals, for n=4 of the three independent experiments. DPCP: diphenylcyclopropenone, IFN: interferon, IL: interleukin, R: responder (n=4), NR: non-responder (n=4). *p<0.05 calculated by Wilcoxon signal rank test in the responder and non-responder group each. †Responder: hair regrowth assessment score ≥3 (hair regrowth ≥50%) at 4 months after DPCP treatment, non-responder: hair regrowth assessment score <3 (hair regrowth <50%) at 4 months after DPCP treatment.
![]()
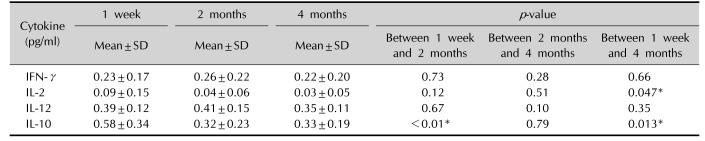
Table 5
Comparison of the differences of cytokine levels in total eight patients after DPCP treatment
![]()
 XML Download
XML Download