

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bullous pemphigoid (BP) is the most common subepidermal blistering disease, characterized by blisters mainly on the skin in the elderly1. The clinical features of BP include pruritic generalized tense bullae and urticarial plaques2. BP has been reported to be significantly associated with mortality; the first-year mortality rate varies between 6% and 44%, depending on the country, while the 1-year standardized mortality ratio (SMR) ranges from 2 to 15345678910111213141516171819202122232425262728293031. The reason for this large difference in mortality rates among countries is unclear.
BP has also been associated with several comorbidities. It is associated with an autoantibody response to BP180 (BPAg2) and BP230 (BPAg1), two components of adhesion complexes promoting dermo-epidermal cohesion. BPAG1, encoded by DST, has specific isoforms: BPAG1-e is mainly expressed in epithelial tissue, anchoring keratin-containing intermediate filaments to hemidesmosomes, while BPAG1-a and BPAG1-b are expressed in neural and muscle tissues323334. Although the pathogenesis of BP remains unknown, previous studies suggest that the cross-reactivity between these isoforms could be pathogenic in BP34. Furthermore, recent studies have shown that patients with BP are more likely to have neurological and psychiatric diseases than general population3536373839.
Nevertheless, only few studies regarding the mortality, prognostic factors, and comorbidity profiles of BP have been reported in Korea. The main objective of this study was to evaluate the mortality, comorbidity profiles, and risk factors of patients with BP who visited our clinic, compared to those of an age-matched general population of Korea.
Go to : 
MATERIALS AND METHODS
Study population
We retrospectively evaluated patients who were diagnosed with BP at Chonnam National University Hospital (CNUH) in Gwangju, Korea, between 2006 and 2013. The diagnosis of BP was based on the following criteria: (1) consistent clinical features, (2) histopathological evidence of subepidermal blister formation, (3) deposits of immunoglobulin G (IgG) and/or C3 along the basement membrane zone, as assessed by direct immunofluorescence (IF) microscopy, (4) presence of circulating autoantibodies bound to the epidermal side of salt-split skin, detected by indirect IF studies, and (5) presence of IgG autoantibodies against BP180 and BP230 antigens, detected by enzyme-linked immunosorbent assay or Western blot analysis. The diagnosis was based on the presence of the clinical (1), histological (2) and immunological (3) criteria, and at least 1 of the serological (4 and 5) criteria. In total, 103 patients with BP who satisfied the diagnostic criteria were enrolled in this study. After an initial workup, patients are usually treated with corticosteroids with or without corticosteroid-sparing agents, such as dapsone, tetracycline, azathioprine, and mycophenolate mofetil. Patients who are refractory to corticosteroid therapy were treated with intravenous immunoglobulin. The demographic data collected include sex, age at the time of diagnosis, date of death, treatment modalities, and comorbidities. Patients lost to follow-up were contacted via the telephone to determine whether they were alive or dead, and in the case of the latter, the date of death.
For statistical analysis, comorbidities were grouped as follows: cardiac disease (e.g., coronary artery disease, cardiac arrhythmia, and congestive heart failure), hypertension, diabetes mellitus, dementia, stroke, other neurological diseases (e.g., Parkinson's disease, psychosis, epilepsy, and multiple sclerosis), malignancy, renal disease (e.g., chronic kidney disease, lupus nephritis, and nephrotic syndrome), and pulmonary disease (e.g., chronic obstructive pulmonary disease, restrictive lung disease, and pneumonia). Only comorbid diseases diagnosed prior to the diagnosis of BP were included in the present study. This study was approved by the Chonnam National University Hospital Institutional Review Board (IRB no. CNUH-2017-252).
Statistical analysis
The primary aim of this study was to investigate the survival of patients with BP during the 5 years following their diagnosis. Mortality rates at 1 year, 2 years, and 5 years following the diagnosis of BP were calculated using the Kaplan-Meier product limit estimator. To evaluate whether there was significant difference in the 5-year mortality rate among patients with BP based on baseline characteristics and morbidities, the Cox proportional hazard model was used to calculate the hazard ratio (HR) and 95% confidence interval (CI). The ratio of the observed deaths of our group to expected deaths from 2007 to 2015, or the SMR, was calculated for patients in 10-year age intervals. The expected age- and sex-adjusted mortality in a general Korean population was calculated using the mortality rate for year at initial diagnosis from life tables of the Korean Statistical Information Service. An SMR of 1 means that observed and expected age- and sex-adjusted mortality rates are equal.
The secondary aim was to investigate the comorbidity profiles of patients with BP. Hypertension, diabetes, chronic kidney disease, stroke, Parkinson's disease, and dementia were included. We compared between the prevalence of comorbidities of patients with BP and that of a general population in Korea. Conditional logistic regressions were performed to calculate the odds ratio (OR) and 95% CI to estimate the associations between individual diseases and BP. A p-value <0.05 was considered statistically significant. Tables from the Korean Health Insurance Review and Assessment Service in 2012 were used to determine the expected prevalence in a general population of Koreans. IMB SPSS ver. 21.0 (IBM Co., Armonk, NY, USA) and R 3.2.2 were used for statistical analysis.
Go to :
RESULTS
Demographic data
In total, 103 patients with BP were included in this study. Of these patients, 53 (51.5%) were male and 50 (48.5%) were female (Table 1). The mean age±standard deviation (SD) at which BP was diagnosed was 74.4±10.6 years, and the median age was 76 years (range, 41~96 years). The majority of patients (89.3%) were aged ≥60 years. The mean duration of follow-up for those alive at the end of the analysis was 66.4 months, and for all patients, the mean duration of follow-up was 47.1 months.
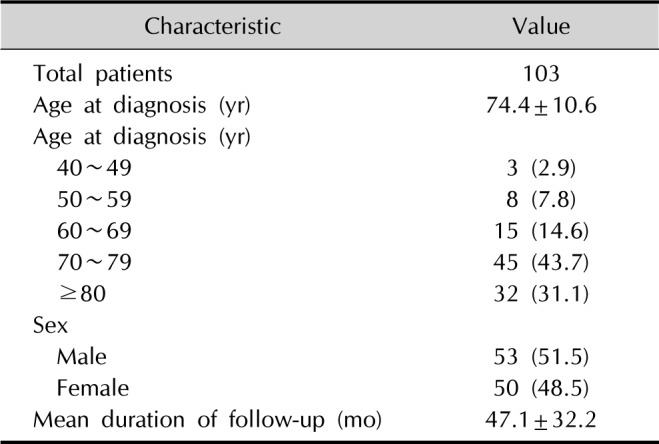
Table 1
Demographic characteristics of patients with BP
![]()
In this study population, systemic corticosteroids were the most frequently prescribed medications; in fact, all of the study participants received corticosteroids. Other therapeutic agents include dapsone, colchicine, mycophenolate mofetil, and azathioprine, among others.
Mortality and standardized mortality ratio
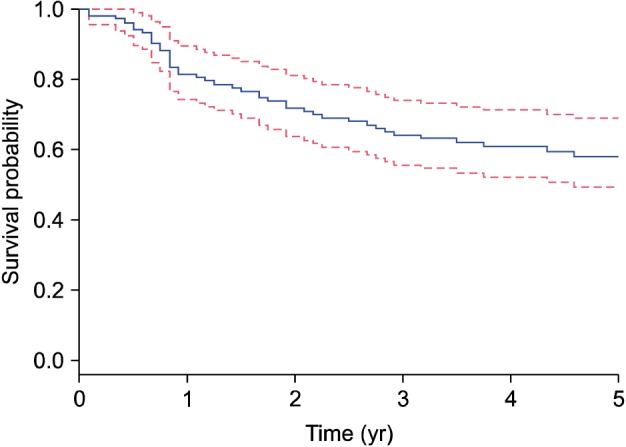
Of the 103 patients included in this study, 61 (59.22%) were still alive at the time of the final analysis. The 1-year, 2-year, and 5-year mortality rates for our BP cohort were 18.44% (95% CI, 10.62~25.63), 28.16% (95% CI, 18.88~36.30), and 42% (95% CI, 31.33~51.00), respectively. A survival curve of BP patients is shown in Fig. 1.
The results of the SMR analysis are shown in Table 2. The SMR ranged from 0 to 2.35, depending on the age. The mortality of patients in our BP cohort was higher than the expected mortality of age- and sex-matched individuals in the general population for aged ≥70 years. The SMR was significantly elevated, particularly in patients aged 70~79 years.

Table 2
SMRs of observed deaths in patients with bullous pemphigoid versus expected deaths among the general Korean population
![]()
Risk factors
Factors related to 5-year mortality were evaluated and shown in Table 3. Age at the time of diagnosis of over 70 was significantly associated with higher mortality (HR, 9.32; 95% CI, 2.25~38.60). Among the comorbidities, cardiac disease (HR, 2.50; 95% CI, 1.15~5.40) and renal disease (HR, 2.99; 95% CI, 1.38~6.48) were significantly associated with elevated mortality in the univariate analysis. However, age at the time of diagnosis and renal disease remained significantly associated with elevated mortality in the multivariate analysis. Patients with BP having hypertension, stroke, neurological disease, pulmonary disease, dementia and malignancies generally showed increased mortality; however, there was no significant difference in the mortality rate.
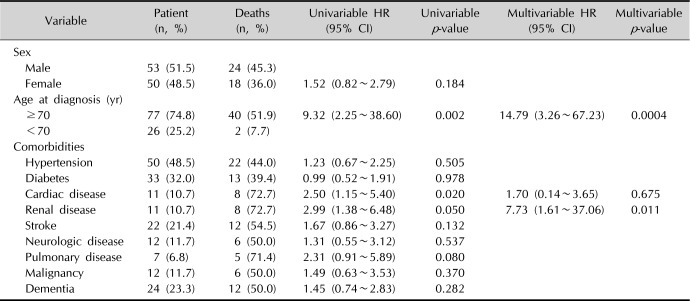
Table 3
Results of the univariate and multivariate analyses for 5-year mortality in patients with bullous pemphigoid
![]()
Comorbidity profiles
Comorbidities of patients with BP compared with general population are shown in Table 4. Our results showed that the presence of diabetes (OR, 1.64; 95% CI, 1.06~2.55), stroke (OR, 3.55; 95% CI, 2.09~6.03), Parkinson's disease (OR, 3.45; 95% CI, 1.49~7.98), and dementia (OR, 2.76; 95% CI, 1.67~4.56) were significantly associated with BP compared to the general population. Although hypertension was the most common comorbidity, it was not significant.

Table 4
Prevalence of comorbid diseases in patients with bullous pemphigoid compared with the general population
![]()
Go to :
DISCUSSION
In this study of 103 Korean patients with BP, we observed 1-year, 2-year, and 5-year mortality rates of 18.44%, 28.16% and 42.00%, respectively; these results were lower or similar to those reported in European studies19202130. However, the mean age of the patients in our study was 74.4±10.6 (SD) years, which is approximately 5 years younger than that of previous European studies202128. Considering the younger age, our results are consistent with those of the European studies. A recent study from Finland showed a 1-year mortality 16.7%, which is lower than our results30. Some US-based studies reported lower mortality rates than European studies, although a recent US-based cohort study demonstrated a higher mortality rate that was closer to those seen in our results and previous European data1116. Recently, several studies regarding the mortality rates of patients with BP have been conducted in Asian countries. The mortality rates and SMR analyses of patients with BP from Asian studies are shown in Table 522232627. One study from China23 showed a slightly higher 1-year mortality rate compared to our study (23.4%), while another study from China reported lower 1-, 2-, and 5-year mortality rates at 12.9%, 20.1% and 33.5%, respectively22. Considering that the mean age of the patients from the latter Chinese study was 67 years, this disparity in mortality rate is justifiable. One Singaporean study reported a higher 1-year mortality rate (26.7%) than that of our study. The mean age of their study patients was slightly older (75.7 years) compared to ours (74.4 years)26. A recent retrospective study from Korea with a total of 168 BP patients reported 1-, 2-, and 5-year mortality rates of 19.46%, 29.13% and 58.03%, respectively27. These values are slightly higher than ours, despite the lower mean age of the study population (69.2 years) compared to ours27.

Table 5
Mortality rates and standardized mortality ratios (SMRs) for bullous pemphigoid patients from Asian studies
| Author | Country | Mean age (yr) | 1-year mortality (%) | 2-year mortality (%) | 3-year mortality (%) | 5-year mortality (%) | SMR |
|---|---|---|---|---|---|---|---|
| Li et al.22 (2013) | China | 67 | 12.9 | 20.1 | 33.5 | 3.08~6.14 | |
| Zhang et al.23 (2013) | China | 71 | 23.4 | ||||
| Cai et al.26 (2014) | Singapore | 75.7 | 26.7 | 38.4 | 45.7 | 2.74 | |
| Lee and Kim27 (2014) | Korea | 69.2 | 19.46 | 29.13 | 58.03 | 2.43~9.56 | |
| Our study | Korea | 74.4 | 18.44 | 28.16 | 42.00 | 1.83 |
![]()
We compared the mortality rate of patients with BP with those of an age- and sex-matched general population. From our results, we found that patients with BP had increased rates of mortality compared to the general population. In those aged ≥70 years, the mortality rate of BP patients was higher than the expected rate for the general population, particularly in patients who were 70 to 79 years old. Several cohort studies from Europe have reported that patients with BP have increased mortality compared with age-matched general populations192128. In addition, recent Asian studies reported significantly higher SMR among patients with BP compared to the general population222627. Our data support the results of these reports, in which BP is significantly associated with increased mortality.
BP was associated with a number of antibody-mediated autoimmune, infectious, cardiovascular, neurological, and psychiatric disorders. Our results showed that the prevalence of diabetes, stroke, Parkinson's disease, and dementia were significantly associated with BP compared to that of the general population. The increased prevalence of diabetes is likely to be related to prior treatment with corticosteroids; however, the exact reason for this association is unclear. Studies have shown that patients with BP are most very likely to have neurological diseases as stroke, dementia, and Parkinson's disease3536373839. A recent cohort study from USA showed that patients with BP had numerous neuropsychiatric disorders, including dementia and Parkinson's disease31. The pathomechanism underlying the association between neurological diseases and BP is not fully understood; however, autoimmunity against BP antigens in the brain that cross-react with the skin have been proposed as a possible triggering factor26. Our results are consistent with recent studies and support the hypothesis that a neuronal isoform of BPAG1 may secondarily trigger an autoimmune response against the epithelial isoform of BPAG1343536.
We examined the risk factors associated with the 5-year mortality of patients with BP. Recent studies have evaluated the risk factors related to 1-year or 3-year mortality. In this study, we believed it was necessary to evaluate both the 5-year mortality rate and risk factors as the mortality rate of patients with BP at 5-year follow-up were significantly higher than those at 1-year and 3-year follow-up. Old age at the time of diagnosis (especially over 70 years) was found to be associated with an increased 5-year mortality rate, consistent with previous reports. Previous European reports have shown that an age of over 80 years was a poor prognostic factor for patients with BP. However, recent Korean reports demonstrated that an age of over 70 years at diagnosis is a risk factor for poor prognosis, in keeping with our results91419202728.
Cardiac and renal diseases were also associated with an increased mortality rate in our study. There were 14 patients with cardiac disease and 14 patients with renal disease among our patients with BP; 7 patients belonged to both disease groups. While the pathomechanism is unclear, diuretics, which are commonly used in both cardiac and renal diseases, have been found to be a risk factor for aggravation of BP in the elderly364041. However, it is unclear whether the use of diuretics is associated with a higher mortality rate. A recent study from Singapore showed that cardiac disease, particularly heart failure, significantly increased the mortality of patients with BP26. Further investigation is required to identify the association between these diseases and increased mortality.
Interestingly, dementia, diabetes and stroke, which many studies have reported to be poor prognostic factors, did not demonstrate increased risk of 5-year mortality in our study161920222327. In a recent Korean study, a history of diabetes also showed an increased risk of 1-year mortality, and stroke was shown to be a poor prognostic factor for overall survival27. Neurological disease, which prior studies demonstrated as a poor prognostic factor16192035, was not associated with increased 5-year mortality. Some of these studies have classified dementia and stroke as neurological diseases but we evaluated each disease individually. In other Korean study, a history of dementia and neurological disease didn't showed an increased risk of 1-year and overall mortality27, which is consistent with our result. There are several limitations of this study. First, we retrospectively evaluated patients with BP by using medical records and direct telephone calls. Second, our study was a single-center study, consisted of a relatively small sample size (n=103), and excluded patients who were lost to follow-up; therefore, there might be selection bias. Third, we failed to obtain data regarding the exact cause of death.
In conclusion, the mortality rate of patients with BP is higher than that of the general population. Korean patients with BP are more likely to have dementia, Parkinson's disease, diabetes mellitus, and stroke. Risk factors for increased mortality include old age at the time of diagnosis, medical comorbidities, especially cardiac and renal diseases. Dermatologists should therefore be extra cautious when they encounter and care for patients with BP with these underlying risk factors.
Go to :
 XML Download
XML Download