

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epilepsy is a chronic debilitating condition that affects about 2.9 million people in the United States.1 The disorder represents a tremendous burden on both individuals and society, with estimates of a direct cost of USD 4.3 billion and a total cost of USD 9.6–15.5 billion annually.23 Although the disease is characterized by episodic attacks, unpredictable recurrent seizures in people with epilepsy (PWE) cause significant disability and negatively impact their health, productivity, and activities of daily living.45 Further, the disease has substantial psychosocial, behavioral, and cognitive sequelae, with frequent seizures, stigma, and seizure worry associated with reduced quality of life (QOL).678 Requirements for chronic medication, barriers to care, employment limitations, and inability to drive a motor vehicle represent longterm hindrances for PWE.
Numerous studies have addressed the impact of demographic and socioeconomic variables, seizure frequency, and comorbid depression on health-related QOL in PWE,91011121314 but there has been less research into how these factors may differ among PWE who have varying clinically relevant degrees of seizure control (i.e., completely controlled, occasional seizures, or poorly controlled). Reports on factors affecting seizure frequency in PWE have typically focused on pharmacological treatments15 or outcomes of epilepsy surgery.16 Since PWE are a heterogeneous population in which the frequency of seizures may vary significantly between individuals and seizure control is a major therapeutic objective, there is value in identifying differences in demographic and clinical variables between PWE with varying seizure frequencies.
The primary purpose of this study was to elucidate differences in demographic variables, depression, and QOL between PWE stratified by seizure frequency in a non-surgical sample of adult PWE using aggregate, de-identified data obtained in studies conducted at multiple United States institutions coordinated by the Managing Epilepsy Well (MEW) Network of the Centers for Disease Control and Prevention (https://www.cdc.gov/epilepsy/research/MEW-network.htm and http://www.managingepilepsywell.org). The present study additionally aimed to demonstrate the validity of using the MEW Network Database (MEW-DB) to conduct research on epilepsy. The MEW-DB is a harmonized database that includes de-identified data obtained in studies of self-management in PWE. The MEW-DB was used to compare the variables of interest between PWE in the following three clinically relevant groups categorized based on the seizure frequency during the past 30 days: completely seizure-free (SZF); fair seizure control, with one to four seizures (FC); and poor seizure control, with at least five seizures (PC).
METHODS
This cross-sectional analysis used data from 481 PWE enrolled in 6 MEW Network epilepsy self-management studies. A detailed description of the MEW Network is available elsewhere.17 The MEW-DB was developed to facilitate aggregate secondary analyses of data collected at individual MEW Network sites,18 with approval received from the Institutional Review Board of University Hospitals Cleveland Medical Center (Principal Investigator, Martha Sajatovic; Reference no. 068620). The de-identified data reported here were collected across four U.S. institutions using studies performed from 2007 to 2016 and reports on baseline data only. The aggregate data used in the analysis comprised participant data from the HOBSCOTCH (HOme-Based Self-management and Cognitive Training CHanges lives) clinical trial performed at Dartmouth-Hitchcock Medical Center,19 the WebEase (Web Epilepsy Awareness Support and Education) clinical trial performed at Emory University,20 the FOCUS (Figure out the problem or the issue, Observe your routine, Connect your observations and choose a change goal, Undertake a change strategy, and Study the results) on Epilepsy pilot study and randomized controlled trial performed at the University of Michigan, and the TIME (Targeted Self-Management for Epilepsy and serious mental illness) and SMART (Self-management for people with epilepsy and a history of negative health events) clinical trials performed at Case Western Reserve University. All of the included individuals were at least 18 years old and had a self-reported diagnosis of epilepsy. They provided informed consent for participating in the respective studies and the values of demographic variables including age, gender, race, ethnicity, education, income, and relationship status. The study participants also provided information on seizure frequency and were assessed for QOL and depression severity. Seizure frequency was standardized across studies to a consistent time frame of 30 days prior to presentation for the baseline study assessment. Data on seizure type and epilepsy type were not consistently available across the included studies. The patients were classified based on the 30-day seizure count into SZF, FC, and PC groups.
Quality-of-life assessment
QOL in this study was measured with the 10-item Quality of Life in Epilepsy for Adults scale (QOLIE-10). The QOLIE-10 is an extensively validated survey of health-related QOL that covers both general and epilepsy-specific domains.21 It is used by clinicians and researchers in various settings and languages, and is a screening version derived from 2 longer instruments: the 89-item QOLIE-89 and the 31-item QOLIE-31. The QOLIE-10 assessment includes questions on health, daily activities, and distress related to epilepsy. Total scores on the QOLIE-10 range from 1 to 50, with lower scores indicating better QOL. To accommodate missing data in the pooled MEW-DB sample, the total score for QOLIE-10 was calculated as the sum of scores for all questions divided by the number of questions answered and a score range of 1–5 with lower scores indicating better QOL. Previous studies have investigated the correlations between QOLIE-10 scores and health-care utilization,22 satisfaction with care,23 anxiety,8 and depression.8
Mental health assessment
Depression in this study was quantified with the nine-item Patient Health Questionnaire (PHQ-9), which is a self-administered multipurpose instrument for screening, measuring, and monitoring the severity of depression in patients. The PHQ-9 has been validated in several patient populations,24 including adult PWE,25 and it incorporates the Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria for major depressive disorder in patients with medical comorbidities. In PWE, the PHQ-9 has been validated against the Neurological Disorders Depression Inventory for Epilepsy25 and has been used in several studies.2627 Scores on the PHQ-9 of 5, 10, 15, and 20 correspond to mild, moderate, moderately severe, and severe depression, respectively.
Statistical analysis
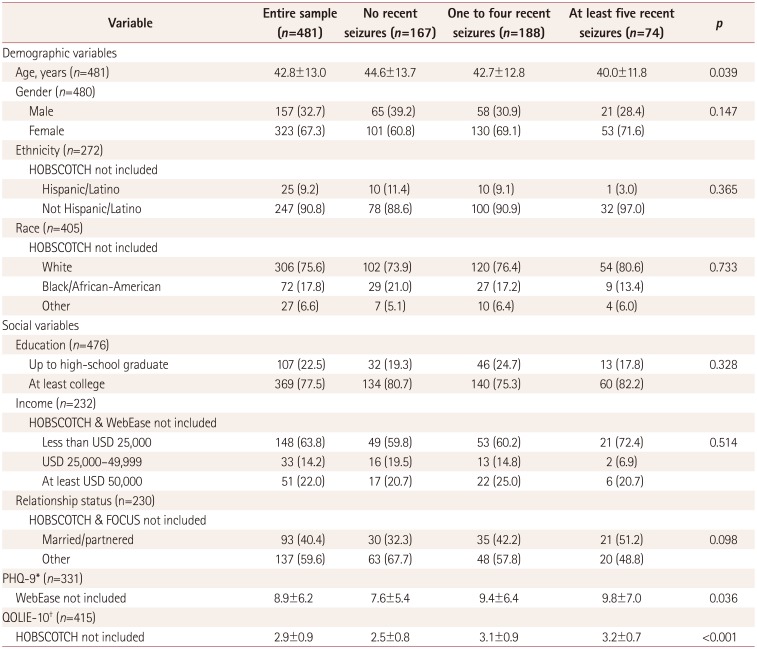
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) program (version 22, IBM SPSS Statistics for Windows, IBM Corporation, Armonk, NY, USA). Due to heterogeneity in variable definitions and data collection between the 4 study sites contributing data, the sample sizes used when comparing the demographic variables and health status measures between the 3 clinically relevant seizure-frequency groups (SZF, FC, and PC) differed between variables, ranging from 481 for age to 230 for relationship status (Table 1). Chi-square tests were used to compare the categorical variables of gender, race, ethnicity, education, income, and relationship status. One-way ANOVA was applied to identify significant intergroup differences in the continuous variables of age, PHQ-9 score, and QOLIE-10 score. A post-hoc analysis of differences between groups was conducted using Tukey's honest-significant-difference test. In addition to evaluating the three clinically relevant seizure-frequency subgroups, demographic variables and clinical correlates of the 30-day seizure frequency as a continuous measure were evaluated using Spearman's or Pearson's correlation for continuous clinical measures (i.e., age, PHQ-9, QOLIE-10), and t-tests, Kruskal-Wallis tests, or Mann-Whitney tests for categorical clinical measures. The cutoff for statistical significance in this study was set at p≤0.05.
RESULTS
The demographic and clinical variables of the entire sample and the three seizure-frequency categories are summarized and compared in Table 1. The participants were aged 42.8±13.0 years (mean±standard deviation, n=481). Of the 480 participants who reported gender, 157 (32.7%) of them were male and 323 (67.3%) were female. Of the 272 participants who reported ethnicity, 25 (9.2%) identified as Hispanic. Of the 405 participants who reported their race, 72 (17.8%) were African-American. The sample of PWE for whom data on education were available comprised 476 individuals, 369 (77.5%) of whom were college educated. As for income, out of 232 included PWE, 148 (63.8%) reported annual earnings of less than USD 25,000, 33 (14.2%) earned USD 25,000–49,999, and 51 (22.0%) had incomes of at least USD 50,000. In terms of marital or relationship status, 93 out of 230 (40.4%) PWE reported being married or partnered. The PHQ-9 score in 331 PWE was 8.9±6.2, and the QOLIE-10 score in 415 PWE was 2.9±0.9.
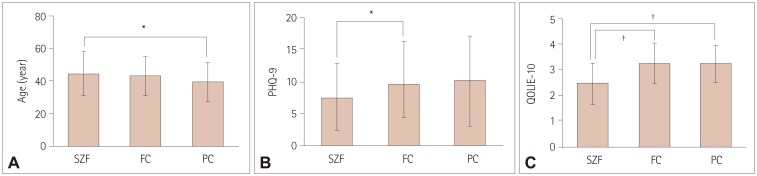
Gender, ethnicity, race, education, income, and relationship status did not differ significantly between PWE in the SZF, FC, and PC groups. Patients with worse seizure control were younger (p<0.039), significantly more depressed (p=0.036), and had a lower QOL (p<0.001). Those in the SZF, FC, and PC groups were aged 44.6±13.7, 42.7±12.8, and 40.0±11.8 years, respectively (p=0.039); their PHQ-9 scores were 7.6±5.4, 9.4±6.4, and 9.8±7.0 (p=0.036), and their QOLIE-10 scores were 2.5±0.8, 3.1±0.9, and 3.2±0.7 (p<0.001) (Fig. 1).
Our evaluation of the relationship between the past 30-day seizure frequency as a continuous measure (irrespective of the clinically relevant degree of seizure control) revealed that PHQ-9 and QOLIE-10 scores remained significantly correlated (rho=0.19 and p=0.001, and rho=0.381 and p<0.001, respectively). Greater number of seizures was associated with worse depression severity and lower QOL. Age was not significantly correlated with 30-day seizure frequency (rho=−0.02, p=0.67). With respect to categorical demographic variables, we found that 30-day seizure frequency as a continuous variable was significantly correlated with gender (p=0.047) but not with the other demographic variables.
DISCUSSION
This study found that PWE with different clinically relevant degrees of seizure control generally have similar demographic characteristics. However, evidence was found of significant differences in depression and QOL in PWE, with frequent seizures associated with an increased severity of depression and lower QOL. Notably, the PHQ-9 and QOLIE-10 scores did not differ significantly between the FC and PC groups, but they were significantly different in the SZF group, suggesting that experiencing a seizure over a 30-day period is associated with worse QOL in PWE. This underscores the importance of achieving complete seizure freedom for ameliorating depression and improving the QOL in this patient population.
The cross-sectional design of this study means that causal inferences cannot be made, but the elucidated relationship between seizure frequency and QOL is congruous with the results of numerous published multivariate analyses of QOL correlates in PWE. Other studies have shown that both depression1112 and seizure frequency10121314 are correlated with reduced QOL in PWE. Poor seizure control might precipitate stress and depression, leading to reduced QOL. The consistency of the present findings with those in other populations of PWE underscores the validity of using the MEW-DB to advance original clinical research into epilepsy.
The significant inverse relationship found between age and seizure frequency in the three frequency categories of PWE might reflect how chronic illness is managed. Learning to manage epilepsy takes time and practice, as supported by a recent prospective study of seizure recurrence in PWE treated with antiepileptic monotherapy finding older age to be associated with a lower likelihood of seizure at follow-up.28 Additionally, Escoffery et al.29 found that safety, wellness, and treatment behaviors were performed less by younger PWE (<30 years) compared to those in older age groups. However, our analysis of the 30-day seizure frequency as a continuous measure in relation to demographic variables did not show a significant relationship with age. These discrepancies might have been due to our sample being relatively small, with limited numbers of individuals at the upper and lower extremes of age.
The lack of significant differences in other demographic variables such as education and income between the SZF group and the FC and PC groups suggests that these factors may be more affected by the affective and cognitive sequelae of epilepsy than by the frequency of seizures.30 Since the mortality, morbidity, and long-term prognosis in chronic disease are negatively impacted by the presence of affective disorders, depression can be conceptualized as a modifiable factor in seizure frequency and QOL outcomes in epilepsy. Comorbid depression has been shown to cause poor medication adherence,31 which in PWE can increase the frequency and severity seizures and decrease QOL. A significant association has been shown between seizure frequency and QOL across all subscale domains of the QOLIE-31 assessment: seizure worry, overall QOL, emotional well-being, energy/fatigue, cognitive functioning, medication effect, and social functioning.9 The rate of psychiatric illness is higher in PWE than in the general population and those affected by other forms of chronic illness.3233
Our findings underscore the importance of the timely identification of comorbid depression by applying screening tools such as the PHQ-9, with subsequent behavioral therapy and/or pharmacological management being applied where required. The benefit of early depression screening, detection, and treatment in PWE has been demonstrated by other investigators. In a randomized controlled trial of systemic family therapy in younger PWE and comorbid depression and anxiety, Li et al.34 found that therapy significantly reduced the 30-day seizure frequency as well as the depression and anxiety symptoms.
Several MEW Network interventions specifically target the reduction of depression as a modifiable and important outcome in epilepsy self-management.35 The UPLIFT (Using Practice and Learning to Increase Favorable Thoughts) for Prevention program tested a remotely delivered self-management intervention for PWE with mild symptoms of depression. The trial demonstrated that the incidence of new or relapsing depressive episodes was significantly lower in the intervention group than in the controls.36 These results supplemented those from a previous single-site trial of UPLIFT for Treatment.37 In another MEW Network study, Ciechanowski et al.38 implemented the Program to Encourage Active, Rewarding Lives for Seniors (PEARLS), an evidence-based treatment program for depression in older adults and PWE.39 Adults participating in the PEARLS program exhibited significantly lower severities of depression and suicidal ideation.3839 The recently published TIME study targeting PWE with comorbid severe mental illnesses including severe depression, schizophrenia, and bipolar disorder found that TIME was associated with improved depression severity compared to the standard treatment.40
Limitations of the present study include its cross-sectional design and the self-reporting of data from heterogeneous sources, which led to inconsistencies in the sample sizes and in the various demographic and clinical variables analyzed between the included studies. Additionally, the education level of the included participants was on average higher than the typical level in large studies of PWE. However, at least half of the study participants were from lower income households. The higher level of education might reflect selection bias in PWE who enroll in self-management research. The high prevalence of moderate depression also reflects selection bias for study participation.
The continuing expansion and refinement of the MEW-DB will led to future analyses aimed at characterizing the longitudinal outcomes for variations in seizure frequency, mood, and other health outcomes among individuals with a chronic neurological condition.
 XML Download
XML Download