

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dementia, of which Alzheimer's disease (AD) is the most prevalent type, is the most frequent reason for institutionalization of the elderly.12 Approximately 20% of patients are institutionalized within 1 year following a dementia diagnosis, and this proportion increases to 50% after 5 years and approaches 90% after 8 years.3 Many studies have identified predictors of institutionalization in patients with AD.3456789101112 The severities of cognitive impairment, functional impairment, and behavioral symptoms such as depression or hallucinations at baseline have been found to be reliable and consistent predictors of institutionalization.3469 The use of antipsychotics was also found to be associated with earlier institutionalization,4 as were the caregiver being a child or another relative rather than the spouse,3 and the patient not being married.36 However, other sociodemographic variables such as age, gender, and whether or not the patient lived alone were considered inconclusive.3469
Most of the above-mentioned studies were conducted in western countries, with analogous studies evaluating Asian populations being relatively rare.7 The social, cultural, and economic situations in certain Asian populations may affect the decisions both to put a patient on a waiting list for a nursing home and then to actually accept an offered space. One previous Korean study7 that included 79 cases identified 6 predictors of the institutionalization of patients with dementia: 3 patient-related factors [higher scores on the Clinical Dementia Rating (CDR) and Brief Psychiatric Rating Scale, and shorter duration of dementia] and 3 caregiver-related factors (younger age, longer formal education, and higher cost of home care). To the best of our knowledge, no previous studies have investigated the predictors of institutionalization in a large Asian population.
This study evaluated baseline factors at a diagnosis of AD that may predict institutionalization in a large Korean sample (n=2,470). We also applied the same interview and neuropsychological tests as in the baseline evaluation before institutionalization to 816 patients who completed at least one follow-up visit, with the aim of identifying predictors of institutionalization among the variables that reflected longitudinal changes in clinical variables after the diagnosis of AD.
Go to : 
METHODS
Participants were drawn from the Clinical Research Center for Dementia of South Korea (CREDOS) study. The CREDOS study is a nationwide multicenter registry cohort study of dementia that began in November 2005.13 Thirty-one university and general hospitals in South Korea have participated in this study to construct a hospital-based registry of dementia patients. The CREDOS cohort is dynamic, with participants being continually added following diagnoses of subjective memory impairment, mild cognitive impairment, mild cognitive impairment of subcortical vascular type, AD, and subcortical vascular dementia. The included participants must agree to be registered in the cohort, and they are removed from the cohort after being lost to follow-up or due to death.14 In addition, the participants can withdraw voluntarily from the cohort.
Patients
From November 2005 to December 2013 we recruited 3,752 patients from the CREDOS study who had very recently been diagnosed with AD. Because the current study utilized nationwide data from the public Long-Term-Care Insurance (LTCI) program to decide whether the patient is qualified for admission to a nursing home, 1,105 patients who were enrolled in the CREDOS study before July 1, 2008 (when the LTCI program started in South Korea) were excluded. Among the remaining 2,647 patients, 134 patients who had already been institutionalized at the time they were enrolled in the CREDOS study were also excluded. Another 43 patients for whom there was insufficient information were disqualified, finally resulting in the inclusion of 2,470 patients.
In evaluating the apolipoprotein E (APOE) genotype as a predictor of institutionalization, 1,456 patients who had agreed to undergo genetic tests were studied. The diagnostic evaluation of patients and inclusion and exclusion criteria are described in detail elsewhere.1315 AD was formally diagnosed in accordance with the criteria of probable AD of the NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association).16
This study was approved by the Institutional Review Boards of all participating hospitals (AJIRB-CRO-07-95 and AJIRB-MED-SUR-12-27), and written informed consent was obtained from patients and their caregivers after they had received a complete description of the study.
Institutionalization
Institutionalization was defined as admission to long-term-care facilities. In South Korea there are two kinds of long-term-care facilities where elderly people in need of nursing care are traditionally and most commonly admitted: long-term-care hospitals and nursing homes. Nursing homes are licensed nursing facilities that provide 24-hour care and benefit directly from the public LTCI program. Direct medical services are not available in nursing homes, but these facilities maintain connections with community hospitals. On the other hand, long-term-care hospitals are community hospitals where long-term admission is available. Elderly people with a chronic illness such as dementia or stroke are mostly admitted to these hospitals, and usually for several years. Long-term-care hospitals receive funding from National Health Insurance rather than from the public LTCI program.
The date of placement in the nursing home was derived from LTCI program data as at January 1, 2014. For those admitted to long-term-care hospitals, we utilized data from National Health Insurance as at January 1, 2014. Because the data from National Health Insurance does not differentiate between acute-care hospitals and long-term-care hospitals, we regarded the patient as institutionalized when he or she was admitted to and remained in the same hospital for at least 6 months.
Public LTCI for the elderly in South Korea
LTCI has been in effect in South Korea since July 2008. The LTCI program covers the entire population aged 65 years and older regardless of income, and the population younger than 65 years selected based on relatively high levels of severity in the standardized evaluation of senile functional disorders that include dementia, cerebrovascular diseases, and Parkinson's disease. The Korean LTCI recognizes in-kind benefits in principle, which consist of home-care and residential-care benefits. Home-care benefits include home help, home bathing, home nursing, day/night care, and short-term care, while residential-care benefits consist of elderly care facilities and group homes. There is flexibility in selecting between residential-care and home-care benefits.17181920 Institutionalized patients with AD must be qualified in LTCI to receive residential-care benefits. When a patient is admitted, long-term-care facilities report data for that patient to the National Health Insurance Service in order to obtain financial support. Thus, since July 2008 when the LTCI program was introduced, lists of dementia patients admitted to long-term-care facilities could be compiled using data from the National Health Insurance Service.
Baseline demographic and clinical variables
The following variables were included as baseline factors: age, gender, length of formal education, Clinical Dementia Rating Sum of Boxes (CDR-SB) score, Mini Mental State Examination (MMSE) score, Geriatric Depression Scale (GDS) score, total score for the NeuroPsychiatric Inventory (NPI), comorbidities such as hypertension, diabetes mellitus, cardiovascular disease, and stroke, alcohol consumption, and smoking. Other included variables were the relationship with the main caregiver (categorized into spouse, son/daughter-in-law, daughter/son-in-law, or others), APOE genotypes, and medication types [cholinesterase inhibitors (ChEI)/memantine, antipsychotics, and benzodiazepines].
Variables for measuring longitudinal changes
The following variables were obtained for patients who completed at least one follow-up visit using the same interview and neuropsychological tests as applied in the baseline evaluation: annual change in MMSE score, annual change in CDR-SB score, annual change in total NPI score, and medication possession ratio (MPR) of antipsychotics and ChEI or memantine. For participants in whom the MMSE, CDR-SB, or NPI score was evaluated several times, the annual score change was obtained by (score at the last visit minus score at the baseline evaluation/time interval in years between the last visit and the baseline visit). Only the tests performed before institutionalization were included for institutionalized patients, while tests performed up to December 2013 were included for not-institutionalized patients. MPR is calculated by dividing the total number of days of prescription use by the total number of follow-up days for the patient. When calculating the MPR, only the number of days before institutionalization was included for institutionalized patients, while the number of days up to December 2013 was included for not-institutionalized patients. We used MPR to evaluate the medication effect on institutionalization since the medication time can vary between patients. Data for variables related to longitudinal changes during the defined period were available for 816 patients.
Data analysis and statistics
Categorical variables are reported as frequencies and percentages, while continuous variables are reported as mean±standard-deviation values. Discrete variables were compared using chi-square tests. Independent Student's t-tests were used to compare characteristics between not-institutionalized and institutionalized groups. We implemented three Cox proportional-hazards models. The first Cox proportional-hazards model was used to identify predictors of future institutionalization among characteristics at the time of diagnosis in 2,470 AD patients. We also performed a sensitivity analysis using a similar model that included the CDR instead of CDR-SB as a variable with the same number of subjects. The second Cox proportional-hazards model was applied to 1,456 patients for whom data were available on the APOE genotype and baseline characteristics at the diagnosis of AD. The final Cox proportional-hazards model was used to investigate predictors among variables that reflected longitudinal changes in clinical characteristics prior to institutionalization in 816 patients who underwent follow-up testing.
Cox proportional-hazards models were created to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for incident institutionalization among AD. The time to an event was defined as the time from study entry to the first-time institutionalization. Participants who had not been institutionalized were treated as censored observations on January 1, 2014. All statistical analyses were performed using the Statistical Analysis System (SAS) (version 9.3, SAS Institute, Cary, NC, USA).
Go to :
RESULTS
Characteristics of the patients
Among the entire cohort of 2,470 patients, 421 patients (17.0%) had been institutionalized in a nursing home (49.2%), long-term-care hospital (44.7%), or both (6.2%) for 38.3±16.5 months. The baseline demographic and clinical variables are presented in Table 1. Patients who were institutionalized were significantly older (75.4 vs. 74.3 years, p=0.005) at baseline and had less education (5.7 vs. 6.4 years, p=0.027) than those who were not institutionalized. Institutionalized patients had more-severe dementia according to CDR and MMSE and more-severe neuropsychiatric symptoms (higher NPI score) at baseline than did the patients who were not institutionalized. These two groups did not differ with regard to pathological comorbidities at baseline such as hypertension, diabetes mellitus, and stroke. Regarding medications, those who were institutionalized were taking more antipsychotics at baseline, but the usage of ChEI, memantine, and benzodiazepine did not differ between the two groups.
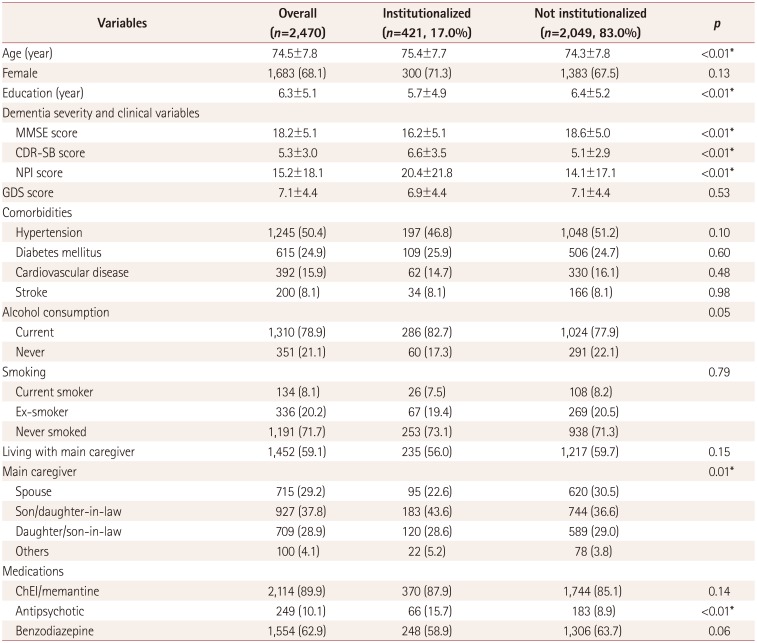
Table 1
Patient characteristics at baseline
Data are mean±standard-deviation or n (%) values.
*p<0.05 between institutionalized and not-institutionalized patients.
CDR-SB: Clinical Dementia Rating Sum of Boxes, ChEI: cholinesterase inhibitors, GDS: Geriatric Depression Scale, MMSE: Mini Mental State Examination, NPI: NeuroPsychiatric Inventory.
![]()
The 1,456 patients for whom APOE genotyping data were available were younger (73.7 vs. 75.6 years, p<0.001) and had more education (6.6 vs. 5.9 years, p<0.001), less hypertension [n=699 (48.0%) vs. n=546 (53.9%), p=0.004], less diabetes mellitus [n=335 (23.0%) vs. n=280 (27.5%), p=0.009], a less-significant history of stroke [n=84 (5.8%) vs. n=116 (11.4%), p<0.001], lower CDR-SB score (5.1 vs. 5.7, p<0.001), and higher MMSE score (18.5 vs. 17.8, p=0.002) than the 1,014 patients without APOE genotyping. The prevalence of the APOE e4 allele did not differ significantly between the institutionalized group (n=87, 37.5%) and the not-institutionalized group (n=499, 40.8%; p=0.352) in the analyses including only the 1,456 patients with APOE genotyping.
The 816 patients who underwent follow-up testing were younger (73.3 vs. 75.1 years, p<0.001) and had a longer total follow-up duration (45.3 vs. 34.9 months, p<0.001), more education (6.7 vs. 6.1 years, p<0.001), lower CDR-SB score at baseline (5.0 vs. 5.5, p<0.001), lower NPI score (13.6 vs. 15.9, p=0.001), lower GDS score (6.7 vs. 7.2, p=0.009), and higher MMSE score (18.5 vs. 18.0, p=0.020) than the 1,654 patients for whom longitudinal changes were not measured. These subjects had a higher usage of ChEI or memantine [n=720 (88.2%) vs. n=1,394 (84.3%), p=0.008] but a lower usage of benzodiazepines [n=478 (58.6%) vs. n=1,076 (65.1%), p=0.001] than did those without variables of longitudinal changes. Of the 816 patients who underwent follow-up testing, 130 (16.0%) had been institutionalized for 45.3±13.0 months. Patients who were institutionalized had a significantly larger annual change in CDR-SB score (3.5 vs. 1.6, p<0.001), larger annual change in MMSE score (−2.9 vs. −1.6, p=0.002), and higher usage of antipsychotics (MPR=0.4 vs. 0.2, p=0.001). Sociodemographic variables such as age, gender, length of formal education, and comorbidities (diabetes mellitus, hypertension, cardiovascular disease, and stroke) did not differ between the groups. The NPI score also did not change significantly from baseline to benzodiazepine use (Table 2).
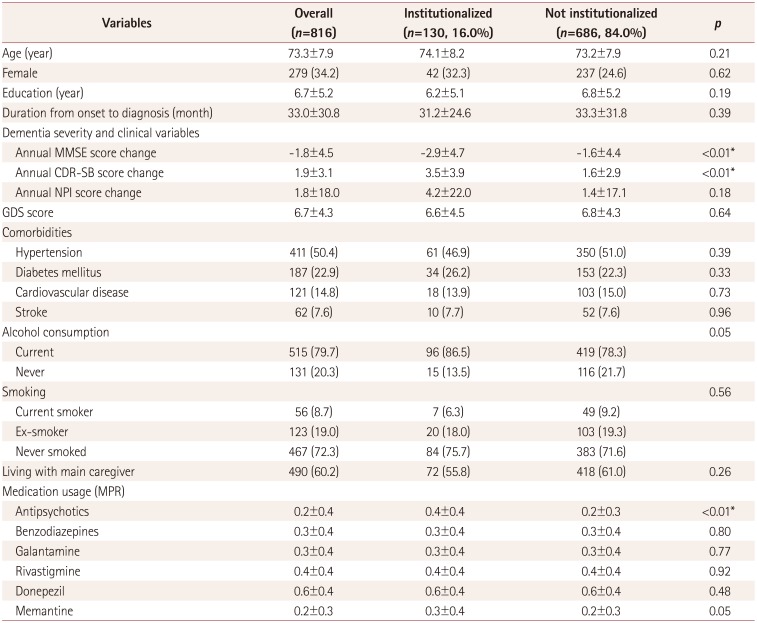
Table 2
Patient characteristics for variables that were measured longitudinally
Data are mean±standard-deviation or n (%) values.
*p<0.05 between institutionalized and not-institutionalized patients.
CDR-SB: Clinical Dementia Rating Sum of Boxes, GDS: Geriatric Depression Scale, MMSE: Mini Mental State Examination, MPR: medication possession ratio, NPI: NeuroPsychiatric Inventory.
![]()
Predictors of institutionalization
The multivariate Cox proportional-hazards model with baseline characteristics among all 2,470 patients revealed that lower MMSE and higher NPI scores at baseline were independent risk factors for institutionalization. Other baseline variables such as age, length of formal education, CDR-SB score, comorbidities, alcohol consumption, smoking, and the relationship with the main caregiver were not significantly related to patient institutionalization. Whether the patient was taking a medication at baseline such as ChEI, memantine, antipsychotic, or benzodiazepine also did not significantly influence institutionalization (Table 3). However, in the sensitivity analysis, a higher CDR score was an independent risk factor for institutionalization (relative to CDR score=0.5: HR=1.79, 95% CI=1.335–2.332, and p<0.001 for CDR score=1; and HR=1.68, 95% CI=1.120–2.533, and p=0.0123 for CDR score=2). In the multivariate Cox proportional-hazards model with baseline characteristics among the 1,456 patients with APOE genotyping, the presence of the APOE e4 allele did not predict earlier institutionalization (p=0.723) (Table 3). In the multivariate Cox proportional-hazards model with variables that were measured longitudinally (816 patients), larger annual change in CDR-SB score (HR=1.15, p< 0.001) and higher MPR of antipsychotics (HR=1.89, p=0.005) predicted a shorter time to when institutionalization would be necessary (Table 4).
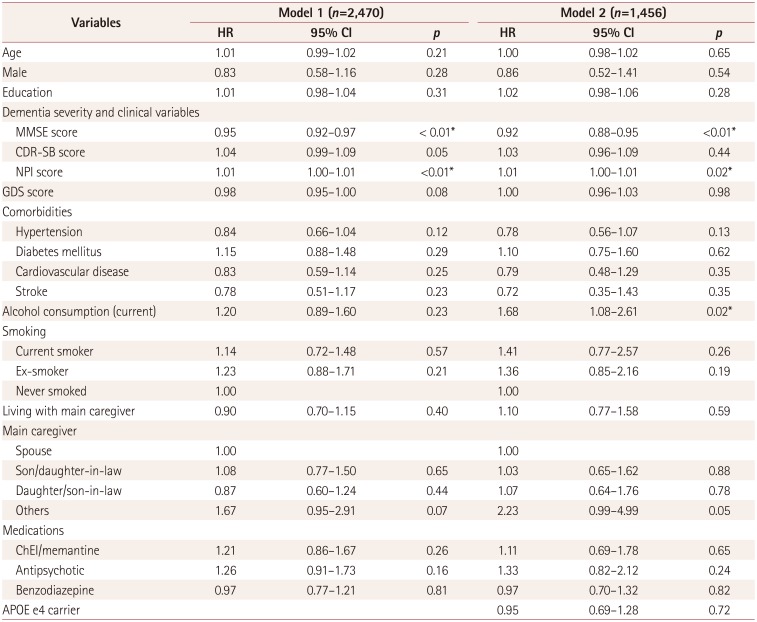
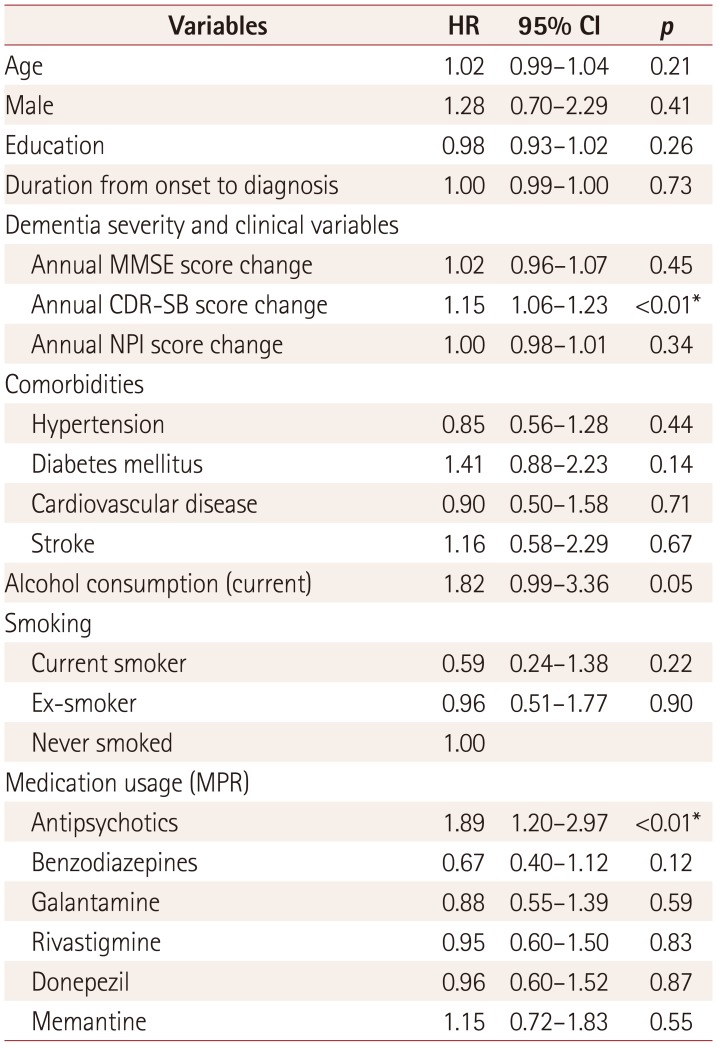
Table 3
Predictors of institutionalization among baseline characteristics at the diagnosis obtained using multivariate Cox proportional-hazards models
![]()
Table 4
Predictors of institutionalization including variables that were measured longitudinally obtained using a multivariate Cox proportional-hazards model with 816 patients
![]()
Go to :
DISCUSSION
This study found that lower MMSE score, higher CDR score, and higher NPI score at baseline, larger annual change in CDR-SB score, and more-frequent usage of antipsychotic drugs were independent predictors of earlier institutionalization. Factors such as APOE genotype and the relationship with the main caregiver did not predict institutionalization.
We found that 17.0% of patients were institutionalized in either nursing homes or long-term-care hospitals at a mean of 3.19 years during the follow-up in our study. This is a smaller proportion than in previous reports. In the systematic review by Luppa et al.,3 approximately 20% of patients were institutionalized within the first year following a diagnosis of dementia. This interstudy difference may be due to cultural differences between Asia (and especially South Korea) and western countries. Korean caregivers show a higher level of familism than do white American caregivers.21 Due to the Confucian attitude of having respect for one's elders, a significant proportion of Korean caregivers are likely to feel guilty about institutionalizing their spouse or parents. This makes them more willing to care for a dementia patient even when the patient demonstrates chronic and severe dysfunction in the activities of daily living (ADL).22
Among baseline characteristics at the time of diagnosis, lower MMSE score and higher CDR and NPI scores at baseline were independent predictors of earlier institutionalization. These findings are consistent with those of previous studies.3469 However, unlike previous reports of being female increasing the likelihood of being admitted to a nursing home,9 the current study found that gender was not related to the rate of inpatient institutionalization, which is consistent with the results of recent studies carried out in Australia.4
The presence of the APOE e4 allele did not predict institutionalization in this study, which is consistent with a previous study.9 The APOE e4 allele is a well-known risk factor for the development of AD,23 but its effect on the progression of this disease remains unresolved. A few studies have found seemingly deleterious effects of the APOE e4 genotype on disease progression,242526 but most studies have found no definite correlation between APOE genotype and the progression of the disease.2527282930 One study even found that the progression of the disease was more aggressive in patients who lack the APOE e4 allele.31 The findings of the current study are therefore consistent with previous reports that the APOE e4 allele is associated with earlier development of AD but not with the disease progression.
Among predictors that measured longitudinal changes, more-rapid decline in the severity of the dementia (CDR-SB) and more-frequent use of antipsychotic drugs were considered independent risk factors leading to earlier institutionalization. In a recent study involving a sample population that included various types of dementia, greater declines in cognitive abilities (MMSE score) and functional abilities [as measured using the SMAF (Functional Autonomy Measurement System)] were associated with earlier institutionalization.4 However, other studies where the sample population was confined to patients with AD found that the rate of change in instrumental ADL decline was probably an independent predictor of earlier institutionalization, although a rapid decrease in MMSE score was also a significant predictor of institutionalization in univariate analysis.9 The current study findings are consider to be essentially in agreement with these findings,9 in that institutionalized patients exhibited a higher decrease in MMSE scores, but a decline in overall dementia severity (CDR-SB) remained the more important predictor. These findings may be due to differences between various types of dementia. A study that employed a functional measure of severity (CDR) in patients with AD and frontotemporal dementia (FTD) who were matched for age and MMSE score found that the total CDR-SB score was significantly worse in those with FTD than in patients with AD.32 This means that when a study population is homogeneous, the MMSE scores may be more strongly correlated with CDR-SB score, resulting in a decrease in the MMSE score not being an independent predictor. Furthermore, to the best of our knowledge, no studies searching for predictors of institutionalization have included CDR-SB in their analyses. In our study the annual change in the CDR-SB score was a significant independent predictor, whereas the CDR-SB score at the diagnosis of AD was not.
This study was subject to some limitations. The dynamic nature of the CREDOS cohort meant that the follow-up periods differed between the patients, making it impossible to know the proportion of institutionalized subjects during a specific time period. Furthermore, APOE genotyping and follow-up tests were performed in only some of the included patients, and we used three data sets with different numbers of subjects. The three models with different numbers of subjects revealed differences in the demographic characteristics, although these differences did not affect the main results. In addition, we regarded a patient as having been formally admitted into a long-term-care hospital when he or she stayed in the same facility for at least 6 months. This 6-month cutoff period was arbitrary, and there might have been some patients who were discharged after staying in the same hospital for more than 6 months. Furthermore, previous studies have found factors such as the caregiver age, caregiving burden, health status, and stress level of the caregivers to be predictors of the earlier institutionalization of patients. However, the lack of sufficient information from caregiver questionnaires meant that various potentially important caregiver factors could not be included or considered in this study. In addition, both the physical and instrumental ADL could be predictors of earlier institutionalization, but ADL scores were not included in the present analyses. Finally, the follow-up tests involved a relatively small proportion of the patient cohort (33.0%, 816 out of 2,470), and so a separate analysis was needed for variables that exhibited longitudinal changes.
This study found that among patients with AD, those with lower cognitive ability, higher dementia severity, and more-severe behavioral symptoms at baseline were more likely to be institutionalized earlier during the course of the disease. More-rapid cognitive decline in the severity of the dementia and more-frequent use of antipsychotic drugs during follow-up were independent indicators of earlier institutionalization. This information will allow clinicians to make more-practical and informed choices regarding treatment options, and assist caregivers in the appropriate management of specific patients.
Go to :
 XML Download
XML Download