

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Interferon-beta (IFN-β) is one of the established first-line therapies for multiple sclerosis (MS). However, not all patients with MS experience satisfactory treatment response.1 Some patients appear to be influenced by the presence of neutralizing antibodies (NAbs) against IFN-β, which has been associated with the occurrence of clinical relapse(s) and/or progression of Expanded Disability Status Scale (EDSS) scores in previous studies, and up to 40% of all patients treated with IFN-β become persistently positive for NAbs.123456 In addition, several molecules-including C-X-C motif chemokine ligand 10 (CXCL10) and soluble tumor-necrosis-factor-related apoptosis-inducing ligand (sTRAIL)-have been reported to be induced by IFN-β and exhibit decreased levels when NAbs are present.78
Because diverse therapeutic options are now available for patients with MS, the timely identification of factors that can affect the efficacy of specific first-line agents is vital to optimize personalized therapeutic strategies.91011 Data regarding NAbs against IFN-β and IFN-β biomarkers have not been evaluated previously in Korean MS patients. Accordingly, we aimed to investigate the prevalence of NAbs against IFN-β and the association between treatment response and persistent NAb positivity. We also evaluated the association between NAbs and IFN-β biomarkers in Korean MS patients treated with IFN-β.
METHODS
Patients who fulfilled the 2010 McDonald criteria12 and clinically isolated syndrome (CIS) suggestive of MS were enrolled. They had received regular treatment with IFN-β (subcutaneous IFN-β-1a 44 mcg thrice weekly; IFN-β-1b 250 mcg every other day; or intramuscular IFN-β-1a 30 mcg weekly) for at least 6 months. Serum samples collected from nine referral hospitals in Korea from 2010 to 2016 were stored at -80℃ until analysis. Sera from patients who were treated with corticosteroids within the previous 1 month or with plasma exchange within the previous 3 months were excluded. Serum samples that were available from 75 patients at 2 different time points were analysed for persistent positivity (PP) of NAbs. The medical records of these patients were analysed to verify the association between treatment response and persistent NAb positivity. Demographic and clinical information was collected from the participating centers.
NAbs were measured using a commercially available luciferase reporter gene assay (iLite, Galway, Ireland), while IFN-β biomarkers (CXCL10 and sTRAIL) were assessed using ELISA kits (R&D Systems, Minneapolis, MN, USA) according to the manufacturer's instructions.
Disease activity was defined as the presence of at least one active MRI lesion [new or enlarging lesion(s) on T2-weighted or fluid-attenuation-inversion-recovery imaging, or gadolinium-enhanced lesions on T1-weighted imaging], and/or the occurrence of clinical relapses during a 1-year follow-up from the confirmation of NAb positivity.13
The chi-squared or Fisher's exact test was used to compare patients with and without NAbs. Student's t-test or the Mann-Whitney U test was performed to compare continuous variables of IFN-β biomarkers, with p<0.05 considered to be statistically significant.
The Institutional Review Board of National Cancer Center approved the study protocol (NCC 2015-0032), and written informed consent was obtained from all patients.
RESULTS
Demographics
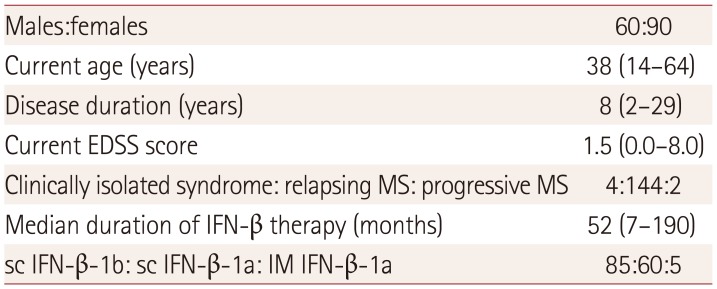
In total, 150 MS patients were recruited from 9 medical centers in Korea; their demographic information is summarized in Table 1. The male-to-female ratio was 2:3, and the median age at sampling was 38 years (range 14–64 years). The median disease duration was 8 years (range 2–29 years), and the median duration of IFN-β treatment was 52 months (range 7–190 months). A total of 146 patients fulfilled the 2010 McDonald criteria, and 2 of them had primary progressive MS. Remained 4 patients had CIS suggestive of MS. The median EDSS score at the last visit was 1.5 (range 0.0–8.0). Of the 150 MS patients in this study, subcutaneous IFN-β-1b, IFN-β-1a, or intramuscular IFN-β-1a was used in 85, 60, and 5 individuals, respectively.
Prevalence of NAbs in Korean patients with MS
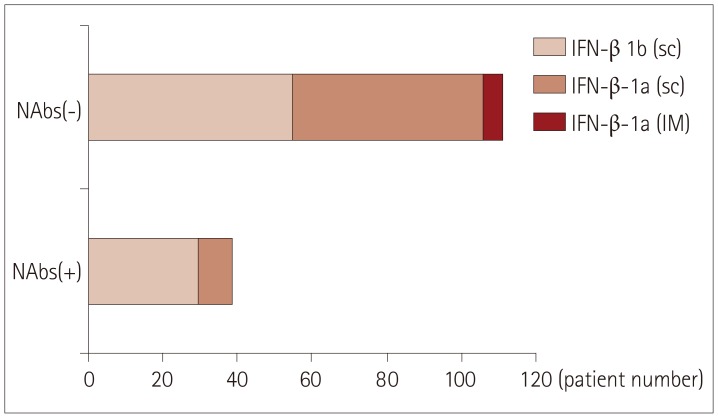
Among 150 Korean MS patients, 226 tests for NAbs were performed, with 39 (26%) patients exhibiting NAb positivity: 30 of the 85 (35%) who were treated with subcutaneous IFN-β-1b, 9 of the 60 (15%) who were treated with subcutaneous IFN-β-1a, and 0 of the 5 (0%) who were treated with intramuscular IFN-β-1a (Fig. 1).
Influence of duration of IFN-β therapy
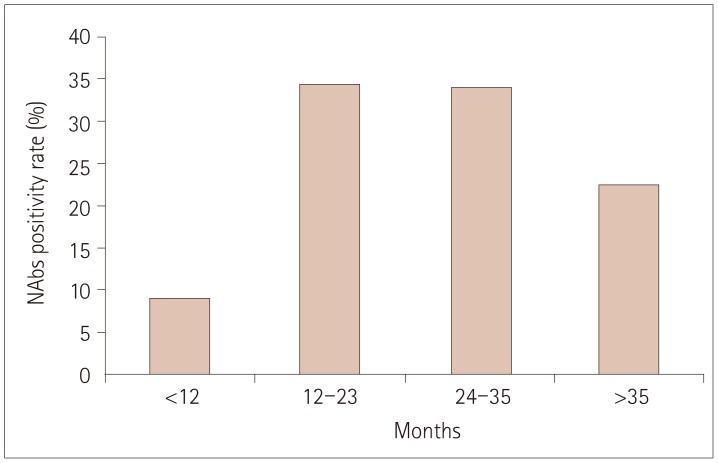
Fig. 2 demonstrates the influence of treatment duration. In the 226 single tests, the positivity rate for NAbs was highest in patients with treatment durations of 12–23 months [22/64 (34.4%)], followed by durations of 24–35 months [15/44 (34.1%)], >35 months [19/85 (22.4%)], and <12 months [3/33 (9.1%)]. The positivity rate for NAbs in patients treated with subcutaneous IFN-β-1b was highest for those treated for 12–23 months (45%), whereas for subcutaneous IFN-β-1a it was highest for those treated for 24–35 months (22.2%).
Association between persistent positivity of NAbs and disease activity
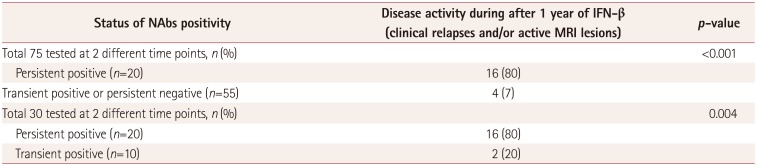
Seventy-five patients with MS were tested for NAbs at 2 different time points at a median interval of 9 months (range 1–102 months), with 20 (26.7%) exhibiting disease activity. Of 39 single-positive NAbs patients, 30 were tested for NAbs at different time points, and 20 patients showed PP of NAbs. Of these 20 patients, 17 were treated with subcutaneous IFN-β-1b, and 3 with subcutaneous IFN-β-1a.
Disease activity was observed more frequently in PP patients than in those with transient positivity (TP) or persistent negativity (PN) for NAbs [16/20 (80%) vs. 4/55 (7%), p<0.001] (Table 2). When disease activity was compared between PP and TP patients, the difference was essentially unchanged and remained statistically significant [16/20 (80%) vs. 2/10 (20%), respectively; p=0.004].
In a sub-analysis of subcutaneous IFN-β-1b treatment, disease activity was observed more frequently in PP than in TP or PN patients [13/17 (76.5%) vs. 3/34 (8.8%), respectively; p<0.001]. When disease activity was compared between PP and TP patients, the difference was unchanged and remained statistically significant [13/17 (76.5%) vs. 1/7 (14.3%), respectively; p=0.009]. Among patients treated with subcutaneous IFN-β-1a, disease activity was observed more frequently in PP than in TP or PN individuals [3/3 (100%) vs. 1/21 (4.8%), respectively; p=0.002]. In these patients, disease activity was observed in 100% (3/3) of PP but 33% (1/3) of TP individuals (p=0.4).
NAbs and IFN-β biomarkers
Among 90 serum samples from 45 PN patients and 40 serum samples from 20 PP patients, an available total of 114 (79 PN and 35 PP) sera were tested for both CXCL10 and sTRAIL. The level of IFN-β-inducible biomarkers did not differ significantly between PN and PP patients: median 156 pg/mL (range 12–2,636 pg/mL) vs. 97.3 pg/mL (10–1,317 pg/mL), respectively (p=0.156), for CXCL10; and median 100 pg/mL (range 2–1,522 pg/mL) vs. 88 pg/mL (27–1,909 pg/mL), respectively (p=0.491), for sTRAIL (Fig. 3). Excluding three samples from PN patients and seven from PP patients with clinical relapse status, similar results were observed {CXCL10 [median 148.3 pg/mL (range 12–2,636 pg/mL) vs. 122.7 pg/mL (20–1,317 pg/mL), respectively; p=0.349] and sTRAIL [median 98 pg/mL (range 2–1,522 pg/mL) vs. 92.5 pg/mL (27–1,909 pg/mL), respectively; p=0.311]}.
DISCUSSION
Twenty-six percent of Korean MS patients in our cohort exhibited NAb positivity: 35% for subcutaneous IFN-β-1b, 15% for subcutaneous IFN-β-1a, and 0% for intramuscular IFN-β-1a. The positivity rate for NAbs was highest (34.4%) in patients with treatment durations of 12–23 months. Disease activity was present in 80% of PP patients, whereas only 7% of TP or PN patients exhibited disease activity (p<0.001). The difference between PP and TP patients remained statistically significant in the presence of disease activity (80% vs. 20%, respectively; p=0.004).
The frequency of NAb positivity in previous studies has varied due to differences in NAb assay methodologies, varying durations of IFN-β treatment, and diverse cohort characteristics. The reported ranges for the rate of NAb positivity have generally been 27–53% in patients treated with subcutaneous IFN-β-1b, 15–35% in those treated with subcutaneous IFN-β-1a, and 2–19% in those treated with intramuscular IFN-β-1a.1415 Our results are comparable with those of previous studies investigating subcutaneous IFN-β-1b and IFN-β-1a, which have been prescribed in Korea since 1998 and 2000, respectively. The prescription of intramuscular IFN-β-1a for MS patients in Korea was approved very recently (2013); therefore, only five patients undergoing this particular treatment could be enrolled in the current study; none of them exhibited NAb positivity.
Cytopathic effect assays to measure myxovirus resistance protein A (MxA), which is stimulated by IFN-β, have been applied in previous investigations.416 ELISA for MxA protein or real-time polymerase chain reaction for MxA messenger RNA have also been used previously.1718 However, the current study used a luciferase reporter gene assay because this is less time-consuming and more cost-efficient, and has demonstrated lower inter-laboratory variability compared with the previously used methods.141920
The emphasis on therapeutic monitoring of NAbs in the decision-making process for switching therapy differs between guidelines from Europe and North America, but an association between NAbs and a reduction in therapeutic efficacy of IFN-β is generally recognized.2122232425 The European guidelines recommend that patients treated with IFN-β should be tested for NAbs after 1 and 2 years of treatment, and altering therapy should be considered when high-titer PP for NAbs in repeated measurements at 3 to 6 months was observed.21222324 Due to the retrospective design of the current study, we could not unify the time points for testing NAbs. Nevertheless, we observed that the positivity rate for NAbs was only 9.1% after <1 year of IFN-β therapy, but >34% for a therapeutic period of 1 to 3 years. More importantly, we reconfirmed that PP for NAbs was associated with disease activity in MS patients treated with IFN-β therapy. Repeated measurement of NAbs may therefore represent an additional indicator that could promote optimal therapeutic decision-making in Korean patients with MS.
CXCL10 is involved in the recruitment of leukocytes and sTRAIL inhibits autoreactive and antigen-specific T cells, and previous studies have found that the levels of these IFN-β-inducible biomarkers were diminished in the presence of NAbs.782627 A recent study found CXCL10 and sTRAIL to be promising potential biomarkers for the response to IFN-β therapy in a longitudinal follow-up.7 Although the mean values of these markers were higher in PN than PP patients in the current study, we did not observe statistically significant differences. This discrepancy could be explained by the limited measurement of IFN-β biomarkers in the only available samples, the uncontrolled timing of assessment due to the retrospective study design. Further prospective longitudinal studies are needed to clarify the clinical implications of IFN-β-inducible biomarkers in Korean MS patients.
The irregular sampling interval of the repeated NAbs measurements and the absence of NAbs titers were additional limitations of the current study. Nevertheless, the reliable assays used in this real-world, multi-center cohort investigation further confirmed that the proportion of patients exhibiting disease activity was significantly higher in PP patients than in TP or PN patients. In an era of various treatment options for MS, identifying suboptimal responders to first-line disease-modifying agents is crucial in clinical practice. Integrating the results of NAb testing with clinical and radiological information may be helpful for establishing optimal individualized therapeutic strategies.

 XML Download
XML Download