

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years there has been an increasing recognition of the importance of stroke in females to both clinical and public health.12 Females have a higher stroke incidence due to their higher life expectancy, since the stroke rate increases dramatically with age.134 Women receive a lower quality of care5 and less frequent use of medication-based guidelines,67 and they are also less likely to receive thrombolysis than men.891011 These sex-related differences might be due to females being, older at onset, having a higher severity of the neurological state, atypical syndromes, delayed time from symptom onset to hospital or from door to needle, greater likelyhood of living alone, or being more unwilling to accept thrombolysis.121314 Many population-based and multicenter studies have shown that women have a longer stroke-related course, worse functional outcome, lower likelihood of being discharged to home, and a lower quality of life than men during the natural course of stroke.151617181920 However, a post-hoc analysis of five pooled randomized clinical trials (RCTs) suggested women can benefit more than men from recombinant tissue plasminogen activator (t-PA) thrombolysis and exhibit a similar outcome to men after thrombolysis independently of other variables.21 A similar conclusion was reached based on post-hoc analysises of the Canadian Alteplase for Stroke Effectiveness Study22 database, Safe Implementation of Treatments in Stroke International Stroke Thrombolysis Register23 study on intravenous t-PA and Prolyse for Acute Cerebral Thromboembolism-224 study on intra-arterial thrombolysis (IAT), and some other studies,2526272829 which included an unadjusted partial meta-analysis that appeared to indicate thrombolysis could nullify or reverse the usual sex effect. In contrast to these findings, there are other reports of worse 3-month functional outcomes in females after thrombolysis, as has also been found for the natural course of stroke.2829 Buijs et al.30 reported that women and men exhibit different prognoses after thrombolysis, with older women appearing to have a worse outcome than men after recombinant t-PA treatment. In contrast, while a recent large cohort study31 also found that a poor functional outcome was more common in women than in men, this difference was not dependent on age.
It therefore remains unclear whether thrombolysis has the potential to eliminate the sex difference in the functional outcome poststroke. In addition, primary randomization is obviously not possible given that sex is a nature-determined factor, and no previous post-hoc-analysis-based or cohort-based meta-analysis has compared outcomes between female and male stroke patients after they received thrombolysis. We therefore conducted a meta-analysis to assess whether sex is a predictor of outcomes in stroke patients after thrombolysis in order to provide useful clinical information for choosing of therapeutic strategies and determining the prognosis following stroke.
METHODS
Search strategy
We performed a computer-based search of PubMed, Embase, and the Cochrane Library for relevant studies up to March 13, 2017 using the following terms: (‘gender’ OR ‘sex’ OR ‘women’ OR ‘men’ OR ‘male’ OR ‘female’) AND (‘thrombolysis’ OR ‘tissue plasminogen activator’). We read the title and abstract of reports that met our search strategy, followed by the full text if the research was identified as being either relevant or unclear. We also reviewed reference lists and citations from these studies to seek additional eligible research. All of the identified references were managed using EndNote.
Outcomes and definitions
The functional outcome at 3 months was categorized using the modified Rankin Scale (mRS) into good (mRS score=0–2), excellent (mRS score=0 or 1), or poor (mRS score=3–6). Recanalization was defined when patients with any thrombolysis had a thrombolysis assessed as myocardial ischemic grades 2 or 3 in computed tomography (CT) or magnetic resonance imaging scans. Symptomatic intracranial hemorrhage (sICH) was defined according to the criteria used in the original studies.
Eligibility and exclusion criteria
Eligible articles described post-hoc analyses of RCTs or original observational cohort studies that investigated the influence of sex difference in the response to thrombolysis in stroke. Included studies were required to have available data on the functional outcome at 3 months. The following exclusion criteria were applied: 1) editorial, case report, systematic review, meta-analysis, pooled analysis, non-original study; 2) retrospective case-control study; or 3) inability to extract relevant data.
Data extraction and quality assessment
Data were independently extracted by two of the authors (Liu and Li) using a standardized criteria with any disagreement resolved by consensus. The extracted data consisted of the study title, year, country, study period, study design, sample size, subject ages, baseline stroke severity, time to treatment, differences in baseline, and main outcome variables. The quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS) with NOS scores of ≥6 points considered to indicate high quality and those of 5 or 6 points considered to indicate moderate quality.
Statistical analysis
Risk ratios (RRs) and related statistics were calculated using Stata (version 12, https://www.stata.com). We calculated RRs and 95% confidence intervals (CIs) either from the total number of events or from the number of events for each outcome when RR was not directly available in original studies. We then pooled the summary effect based on RRs and 95% CIs of outcomes using a fixed-effects models, with p<0.05 regarded as indicative of statistical significance. The chi-squared (χ2) and I-squared (I2) tests were used to evaluate statistical heterogeneity, with a probability value of p<0.05 indicating that significant heterogeneity existed and that I2 values of 25, 50, and 75% indicating low, moderate, and high levels of heterogeneity respectively. Subgroup analysis was conducted to analyze the possible sources of between-study variations. A-priori subgroup analysis was applied to 1) location (Europe, North America, or other), 2) study design (single-center hospital or multiple center hospital; post-hoc analyses of RCTs or original observational cohorts), and 3) subgroup of the method of thrombolysis (intravenous or intra-arterial). A sensitivity analysis was performed by changing the analysis model to random-effects model, sequentially removing individual studies. Publication bias was evaluated using Egger's test and a funnel plot if the number of included studies was sufficient.
RESULTS
Search results and study characteristics
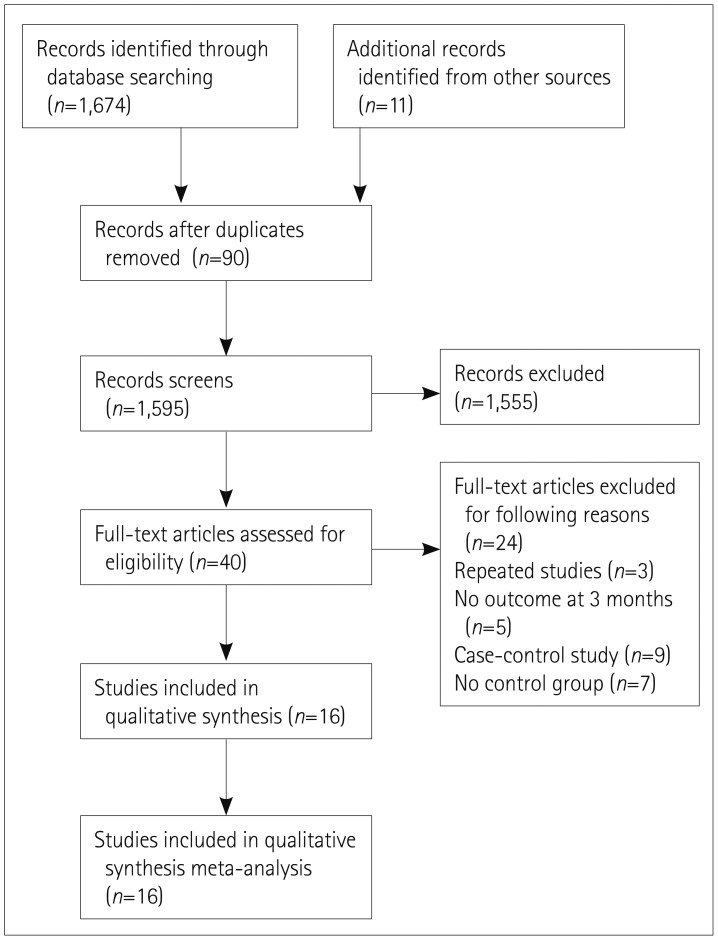
Overall, 1,685 studies were identified and screened for retrieval from the analyzed databases. Careful selection based on the criteria described above identified the following 16 reports involving 60,159 patients as being suitable for inclusion in the meta-analysis: Spaander et al.,31 Buijs et al.,30 Hametner et al.,32 Al-hussain et al.,33 Lasek-Bal et al.,34 Nathanson et al.,35 Lorenzano et al.,23 Martinez-Sanchez et al.,29 Forster et al.,25 Jovanovic et al.,36 Meseguer et al.,26 Kent et al.,22 Gomez-Choco et al.,37 Arnold et al.,27 Elkind et al.,28 Hill et al.24 The flowchart for these studies is shown in Fig. 1.
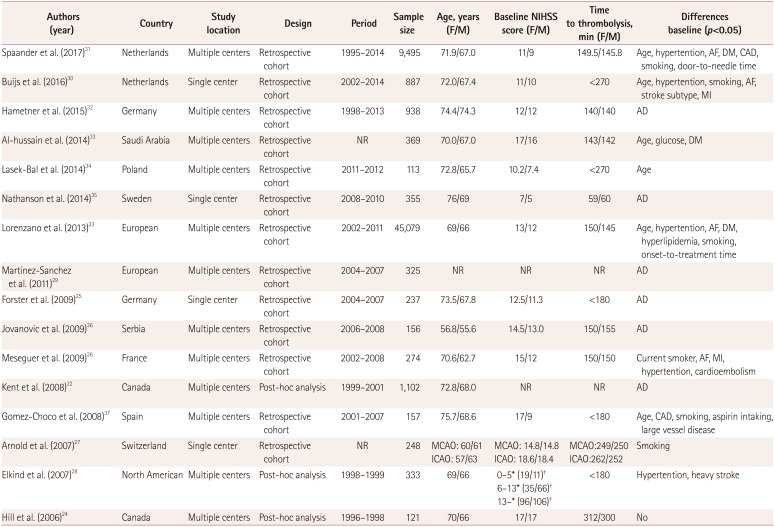
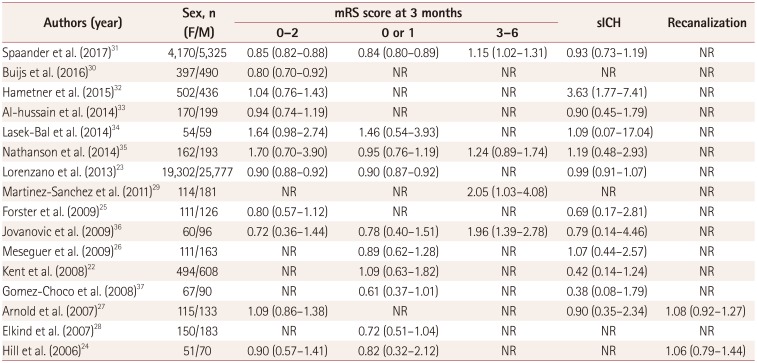
Three of the included researches222428 were post-hoc analyses of RCTs and the other 13 were observational cohort studies. The patients were from Europe in 12 studies, North America in 3 studies,222428 and Saudi Arabia in 1 studies.33 The definition of sICH differed slightly with two studies2235 defining it as a hemorrhage that was not seen on a previous CT scan, with a subsequently been a decline in neurological functional status as defined in the National Institute of Neurological Disorders and Stroke trial,38 five studies2326313236 defining it as an intracranial hemorrhage on a CT scan with a decrease in the score on the National Institutes of Health Stroke Scale of at least 4 or more points as applied by the European Cooperative Acute Stroke Study trial,39 and one studies37 was defining it in accordance with the Safe Implementation of Thrombolysis in Stroke trials.40 sICH was not defined in the reports for the remaining studies.25273334 The detailed individual characteristics of the studies are tabulated in Table 1, while particularly interesting outcomes obtained in the meta-analysis are listed in Table 2.
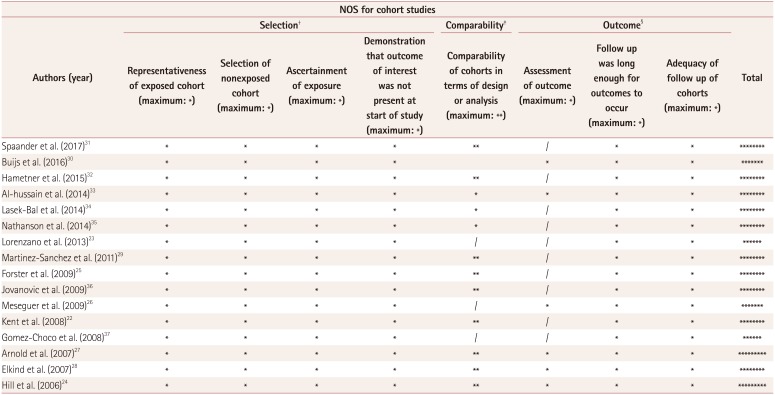
The NOS score was 9 points for two studies, 8 points for ten studies, 7 points for two studies, and 6 points for two studies (Table 3). According to the criteria described above, all of the cohort studies were of high quality, which indicated that all of the included studies were reliable.
Good functional outcome at 3 months
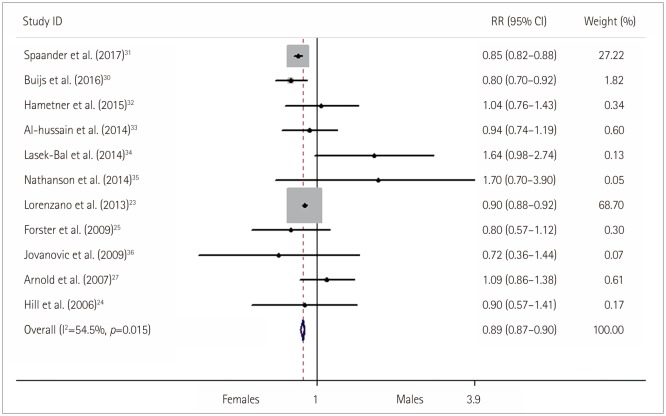
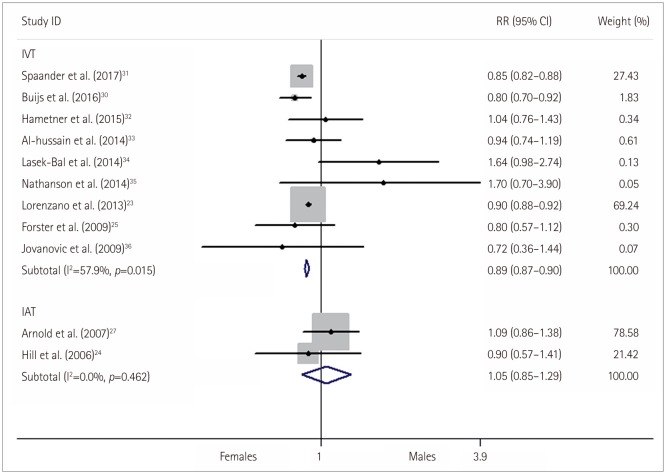
Statistical analysis was applied to 11 studies for which the reported good functional outcome was good (mRS score=0–2) at 3 months. The meta-analysis revealed that the probability of a good functional outcome after administering intravenous thrombolysis (IVT) in acute ischaemic stroke (AIS) was significantly lower among female patients than male patients (RR=0.89, 95% CI=0.87–0.90, p<0.001) (Fig. 2). A moderate heterogeneity was found (p=0.02, I2=54.50%) at the 5% level, but the sources of heterogeneity were not revealed by subgroup analyses of the location, study design or method of thrombolysis. The result for the IAT group was of not significant (RR=1.05, 95% CI=0.85–1.29, p=0.67) (Fig. 3), while the IVT group still showed a statistically significant difference in the subgroup analysis of the method of thrombolysis.
The sensitivity analysis was performed in three aspects: 1) changing the analysis model to a random-effects model, which also producted similar results (RR=0.89, 95% CI=0.84–0.94, p<0.001), 2) sequentially removing individual studies, which produced minor changes in the results only for the study of Lorenzano et al.23 (Supplementary Fig. 1 in the onlineonly Data Supplement); however, the significant difference in the combined RR and CI was still present after removing the that study (RR=0.86, 95% CI=0.83–0.89, p<0.001), which indicated that the conclusion were reliable; and 3) removing studies with small samples,243436 which also produced similar results (RR=0.89, 95% CI=0.87–0.90, p<0.001).
Excellent functional outcome at 3 months
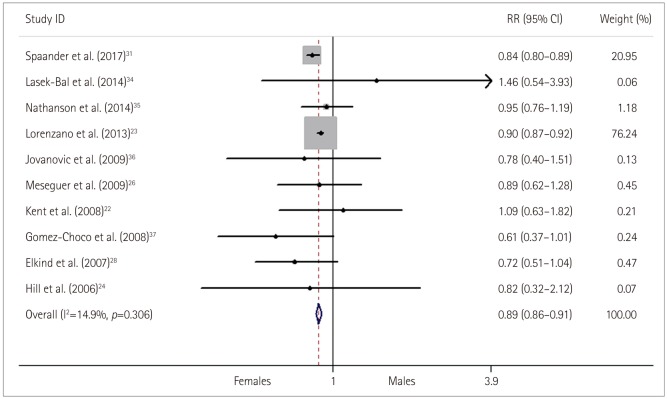
The functional outcome at 3 months was excellent in 10 studies. The combined RR was calculated to be 0.89 (95% CI=0.86–0.91, p<0.001) (Fig. 4), with the likelihood of an excellent functional outcome at 3 months after receiving thrombolysis being significantly lower in females than in males. No significant heterogeneity was found (p=0.31) and so a fixed-effects model was applied (Fig. 4). The sensitivity analysis was performed by changing the analysis model to a random-effects model, which produced the same results (RR=0.88, 95% CI= 0.84–0.92, p<0.001), while sequentially removing individual studies produced minor changes in the results again only for the study of Lorenzano et al.23 (Supplementary Fig. 2 in the online-only Data Supplement). However, the conclusions were consistent, because when removing that study there was still a significant difference in the combined RR and CI (RR=0.84, 95% CI=0.80–0.89, p<0.001).
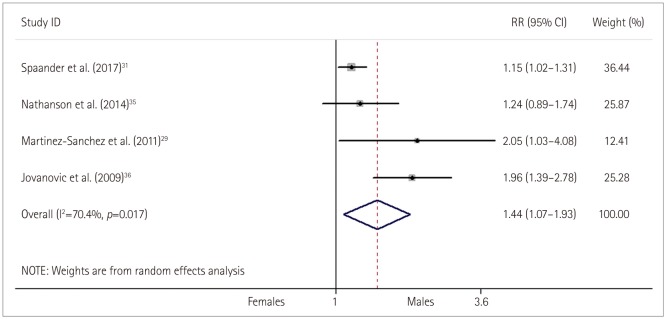
Poor functional outcome at 3 months
On the basis of four studies, a poor functional outcome at 3 months was more likely in females than in males (RR=1.44, 95% CI=1.07–1.93, p<0.001) (Fig. 5). Moderate significant heterogeneity was found (p=0.02, I2=70.40%) and so a random-effects model was applied.
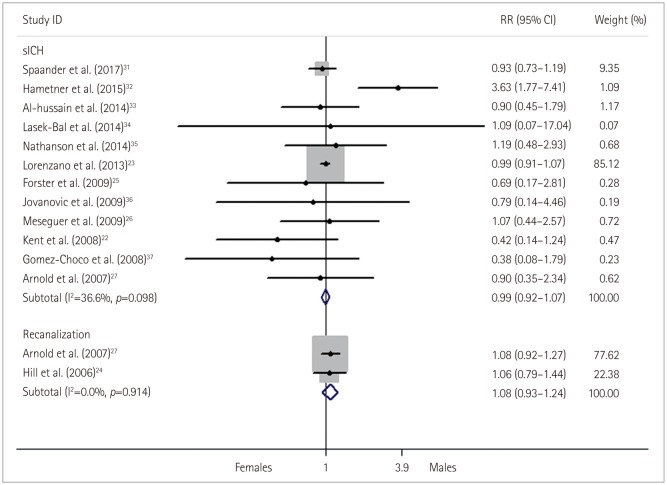
Symptomatic intracranial haemorrhage
The incidence of sICH was reported for 12 studies. The risk of sICH did not differ significantly between female and male stroke patients after thrombolysis treatment (RR=0.99, 95% CI=0.92–1.07, p=0.81) (Fig. 6). No significant heterogeneity was found (p=0.10) and so a fixed-effects model was applied.
Recanalization
Recanalization was reported for two IAT studies. There was no significant difference in the recanalization rate was demonstrated between female and male stroke patients who received IAT (RR=1.08, 95% CI=0.93–1.24, p=0.12) (Fig. 6). No significant heterogeneity was found (p=0.91, I2=0.00%) and so a fixed-effects model was applied.
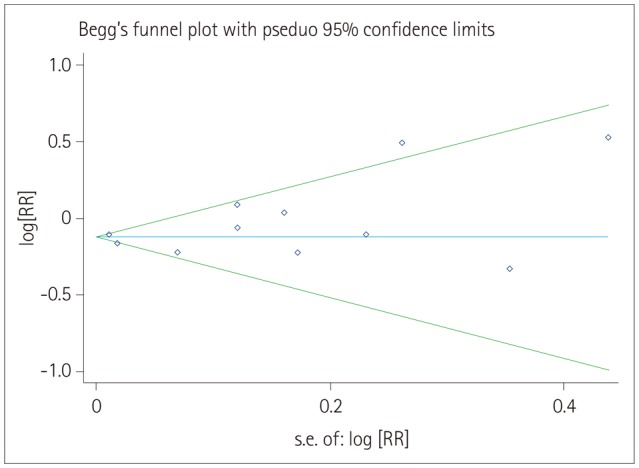
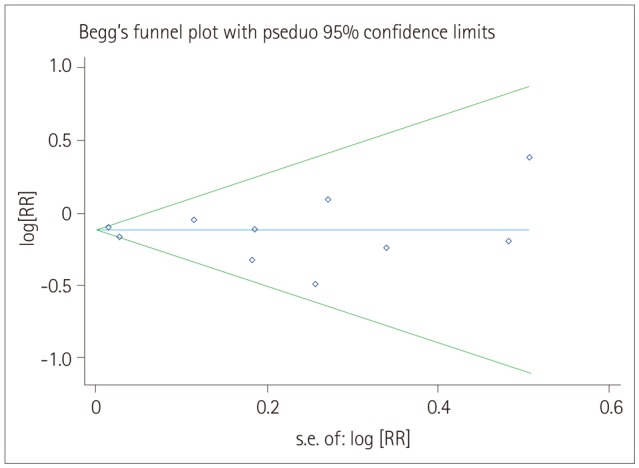
Publication bias evaluation
Overall, no significant publication bias was detected by Egger's test (p=0.42) and Begger's test (p=0.76) for a good functional outcome or for an excellent functional outcome (p=0.59 and p=0.72, respectively). Moreover, there was no obvious asymmetry in the shape of the funnel plot on visual inspection respectively (Figs. 7 and 8). However, insufficient studies were available to test for funnel-plot asymmetry for the other outcomes.
DISCUSSION
It is widely accepted that stroke is a common cause of death and disability and that functional outcome is worse for females than males during the natural course of stroke. However, whether there is a sex disparity in the response to intravenous or IAT in AIS is still controversial. The present meta-nalysis based on 3 post-hoc analyses of RCTs and 13 cohort studies comparing the sex disparity in the functional outcomes of stroke patients who received pharmacological thrombolysis treatment produced the following main findings: 1) a good or excellent functional outcome was less likely and a poor functional outcome was more likely after IVT in females than in males, 2) the rates of a good functional outcome and recanalization after IAT did not differ between females and males, and 3) the rate of sICH did not differ between females and males after they received thrombolysis treatment.
Our finding that females had poor functional outcomes more often than males after receiving thrombolysis is consistent with the findings of several other studies.28293031 One possible explanation of is sex disparities in fibrinolytic factors. Kain et al.4142 reported that the level of plasminogen activator inhibitor-1 (PAI-1) was significantly higher in females than in males with acute stroke, while Ribo et al.43 found PAI-1 to be an independent predictor of thrombolysis resistance. However, female experience more cardioembolic strokes, which are characterized by uniform fibrin-rich and smaller volume embolic clots and therefore a higher affinity for t-PA, making them prone to faster and more frequent recanalization compared with atherosclerotic strokes of the platelet-rich and larger volume occlusions that typically occur in males after IVT.12544 Nevertheless, atrial fibrillation and cardioembolic strokes are associated with worse outcomes including severe neurological impairment and mortality.61517 Thus, whether the advantage of recanalization based on thrombolysis in females can eliminate or reverse the poor outcome of the natural course of stroke is still uncertain. In addition, reperfusion (the goal of thrombolysis) is impacted not only by the recanalization status, but also by other factors such as collateralization and flow changes in communicating arteries.45 Recanalization is associated with good outcomes, but the time from symptom onset to recanalization is also a better predictor of a good clinical outcome.46474849 However, female stroke patients usually experience delay in the time from symptom onset to hospital or from door to needle.121314 To some extent all of these features support the findings of the present study.
Another possible mechanism underlying the worse outcome after IVT in women could be the change in endogenous estrogen levels with increasing age. Animal studies have shown that estrogen is neuroprotective to the severity of ischemia and brain injury,5051 while human research has shown that applying estrogen replacement therapy sooner after menopause decreased the incidence of vascular events.52 These findings indicate that higher estrogen levels exert a neuroprotective effect. Estrogen can also alter the balance between coagulation and fibrinolysis by lowering the level of platelet activator 1, which is a serine protease inhibitor that could decrease the efficacy of IVT. Shahar et al.53 found the levels of PAI-1 was lower in those receiving hormone replacement therapy (HRT), and similarly Gebara et al.54 reported that premenopausal females with high estrogen levels and postmenopausal females receiving HRT had lower PAI-1 levels than males as well as postmenopausal female not receiving HRT. Therefore, the benefit from IVT in females will decline as their endogenous estrogen levels decrease with the increasing age. This is consistent with Buijs et al.30 finding that women have a better outcome in middle age after IVT but a worse outcome in old age. Furthermore, Spaander et al.31 showed that the turning point from a good functional outcome to a poor functional outcome occurred at around the age of 40 years although women had a worse functional outcome than men was independently of age. These mechanisms support our finding that females more often had worse outcomes than males after IVT, since the patients in all of the included studies were older and so estrogen had a lesser effect.
The conclusions from previous studies of the relationship between sex differences and functional outcome after IVT were controversial. Our analysis reveals that this could be due to the following reasons. Firstly, several studies did not adjust for many baseline differences between females and males, such as age, stroke severity, time to treatment, stroke subtype, size and position of embolus, and comorbidities. Even though some researches adjusted for these baseline differences using conventional methods (restriction and multivariable regression) or even new methods (propensity score adjustment and the instrumental variable approach), the confounding factors were still not adequately controlled, leaving the possibility of residual confounding.55565758 Secondly, the prestroke status, sociodemographics, living situation, family background poststroke care, and poststroke complications were not recorded or assessed in almost all previous studies, and these characteristics that could influence the functional outcome might differ between females and males. Lastly, the discrepancies in the conclusions might also attributable to differences in study designs and populations of interest and, in some cases, to the smallness of the included samples.23 Thus, a further studies with large-scale cohorts and that address the aforementioned imperfections are needed to confirm these findings.
The present study found no significant difference in outcomes or recanalization after IAT between the two sexes. This is consistent with some previous studies,242759 but it contrasts with the results for IVT in our study. It is well known that IVT is administered in a fixed-dose fashion while IAT is administered in a flexible-dose fashion, with infusion continuing until recanalization is achieved or a maximum dose is reached. The higher local concentrations of fibrinolytic agent achieved by IAT may overwhelm the hemostatic and thrombus volume differences and even modest differences between females and males, permitting equal recanalization rates and outcomes between the sexes. The other finding of no difference in sICH between females and males after IVT indicated that thrombolysis is equally safe in both sexes.
As far as we are aware, this is the first meta-analysis to have systematically determined the relationship between outcomes after thrombolysis treatment and sex. Although the method of thrombolysis varied somewhat between the studies, this was not the source of interstudy heterogeneity. Our subgroup analysis produced different results for IVT and IAT. In addition, the large sample, sufficient observational outcomes (good, excellent, and poor functional outcomes, recanalization, and sICH) and absence of publication bias also represent considerable strengths of the present study.
However, some limitations should also be mentioned before generalizing the present findings. Firstly, the included studies were observational studies, which are particularly prone to selection bias and confounding the real relationship between two sexes, various comparative cohort observational designs are now the most appropriate research methods for exploring whether sex is a predictor of outcome after thrombolysis. Secondly, the RR and CI values for some of the included studies were not adjusted for baseline characteristics, which might have resulted in confounding bias. This cannot be adjusted for in logistic regression analysis or multiple regression analysis due to the nonavailability of data for individual patients. Thirdly, heterogeneity was present between the studies. Although, we were unable to identify the sources of this heterogeneity in subgroup analysis, our conclusions were not changed when we performed sensitivity analysis. Fourthly, only 369 patients received IAT in the subgroup analysis of thrombolysis methods. The smallness of this samples means that caution is required when attempting to draw conclusions, and hence further studies with large-scale cohorts are needed to confirm our findings regarding IAT.
CONCLUSION
This study has demonstrated that females appear to often exhibit worse outcomes than males after IVT, while there are no relevant sex differences in outcomes and recanalization after IAT, with equivalently safety regarding hemorrhage complications from thrombolysis for both sexes. However, our findings should be interpreted with caution regarding whether females should receive additional therapy after IVT or change to thrombolytic treatment strategies (e.g. females receive IAT primarily after admission or dosing adjustment according to clot size in IVT). Thus, IVT should not be withheld from female stroke patients by physicians solely based on their sex before further large-scale cohorts research confirms the present findings.
 XML Download
XML Download