

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Oxaliplatin is an antineoplastic agent currently indicated for use with 5-fluorouracil (5-FU) and leucovorin (LV) (FOLFOX) for the adjuvant treatment of patients with surgically resected colon cancer.12 The introduction of the FOLFOX regimen has significantly improved overall survival rates for patients diagnosed with colon cancer. However, chronic oxaliplatin-induced peripheral neuropathy (OIPN) is a well-recognized toxicity of oxaliplatin that can require dose reduction or even premature treatment discontinuation.34 The mechanisms involved in OIPN include altered ion-channel and receptor activity, neuronal injury, oxidative stress, and inflammation resulting from the accumulation of oxaliplatin in dorsal root ganglia cells.56 Moreover, OIPN can persist for a prolonged period, including after oxaliplatin therapy has been discontinued.
Despite the widespread use of oxaliplatin, data on the long-term outcomes and predictors of the severe form of OIPN for patients with this condition are inadequate. Given improvements in the survival of patients with colon cancer, persistent neuropathy can seriously impact their quality of life (QoL).7 The present study performed prospective and longitudinal assessments of oxaliplatin-treated patients with the aim of determining the incidence, clinical impact, electrophysiological pattern, and long-term outcome of chronic OIPN at 1 year after chemotherapy discontinuation. This study also explored the predictors of severe OIPN using clinical and electrophysiological variables.
METHODS
Patients
The Institutional Review Board of National Cancer Center approved this protocol, and written informed consent was obtained from all patients prior to study entry (NCCCTS-08-372). We prospectively studied patients with stage III and high-risk stage II colon cancer who were scheduled to receive adjuvant treatment with FOLFOX4 or FOLFOX6 between March 2009 and September 2012. Patients were recruited over a 24-month period at the National Cancer Center in Korea.
The inclusion criteria were 1) histologically confirmed adenocarcinoma, 2) no prior chemotherapy, and 3) adequate hematological, hepatic, and renal functioning. The exclusion criteria included a history of peripheral neuropathy, alcohol abuse, prior exposure to neurotoxic agents, degenerative neurological disorders, or HIV. Five patients who had well-controlled diabetes without neuropathy were included. Among the 100 patients who were initially registered in this study, 31 were lost to follow-up before the end of treatment for reasons of consent withdrawal (n=15), change of treatment (n=5), treatment discontinuation due to chemotherapy-related side effects (7 patients experienced neutropenia and 1 patient experienced severe OIPN), transfer to another hospital (n=2), and death (n=1).
Chemotherapy regimen and dose modification
Patients received the FOLFOX4 or the modified FOLFOX6 regimen. The FOLFOX4 regimen consisted of LV, 200 mg/m2/day given as a 2-hour infusion, followed by a bolus 5-FU, 400 mg/m2, and a 22-hour continuous infusion of 5-FU, 600 mg/m2, repeated for 2 consecutive days. Oxaliplatin, 85 mg/m2, was administered on day 1 only and was given as a 2-hour infusion in 250 mL of dextrose 5%, concurrent with LV. The modified FOLFOX6 regimen included oxaliplatin, 85 mg/m2 in 250 mL of dextrose 5%, concurrent with LV, 400 mg/m2, given as a 2-hour intravenous infusion on day 1, followed by a bolus 5-FU, 400 mg/m2, on day 1 and a continuous 5-FU, 1,200 mg/m2/day, on day 1 and 2 (46-hour continuous infusion of a total 5-FU of 2,400 mg/m2). Cycle repeated every two weeks up to 12 cycles. Dosing was modified according to predefined, toxicity-based guidelines as described in the MOSAIC trial.1 The oxaliplatin dose was reduced by 20% in the presence of persistent or temporary (lasting for at least 14 days) painful paresthesia, dysesthesia, or functional impairment. Along with oxaliplatin dose reductions, we reduced bolus and infusion doses of 5-FU by 20% in the event of grade-3/4 neutropenia or thrombocytopenia (or both), stomatitis, diarrhea, or other grade-3 drug-related adverse effects. If grade-3 neurotoxicity persisted despite the 20% reduction in oxaliplatin dose, subsequent cycles omitted chemotherapy.1 Analgesics with or without antiepileptics could be administered to those with severe OIPN at the discretion of the investigators.
Evaluation of peripheral neuropathy
All subjects underwent clinical examinations and nerve conduction studies (NCS). A clinical examination including the clinical history specifically addressing symptoms of pain, tingling, or numbness, as well as a general neurological examination was performed by two neurologists (S.H.K. and W.K.) at every evaluation. QoL was analyzed using the Korean version (version 3.0) of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C-30 (EORTC QLQ C-30).8 QoL improved with increases in the scores for global health status and on the functional scale, and worsened as the score on the symptoms scale increased. Chronic OIPN was defined as a clinical syndrome characterized by persistent, symmetrical distal painful or nonpainful paresthesia and dysesthesia.9 The incidence and severity of OIPN were graded using version 3.0 of the National Cancer Institute common toxicity criteria (NCI-CTCv3),10 with the severity classified as grade 1, 2, or 3. Patient-reported outcomes were also used to quantify the frequency and severity of OIPN at baseline and at each follow-up visit, using the EORTC QLQ–Chemotherapy-Induced Peripheral Neuropathy 20 module (EORTC QLQ-CIPN20).1112
NCS included analyses of sensory conduction in the median, ulnar (orthodromic technique), and sural (antidromic technique) nerves, with measurements of the peak-to-peak amplitude of the sensory nerve action potential (a-SAP) and the sensory conduction velocity (SCV). Motor conduction in the median, ulnar, common peroneal, and tibial nerves was also recorded, with measurements of the peak-to-baseline amplitude of the compound muscle action potential (CMAP) and motor conduction velocity (MCV).
NCS results were compared with normal age-matched reference data from our laboratory. All of the aforementioned baseline evaluations were repeated 2 weeks after 4, 8, and 12 cycles of chemotherapy, and at 6 months and 1 year after chemotherapy. Among the 69 patients in whom repeated evaluations were performed during treatment, 36 patients completed evaluations at 6 months and 1 year after completing chemotherapy. All 69 patients in whom evaluations were performed after 12 cycles of treatment, and 36 patients in whom evaluations were performed at 6 months and 1 year after chemotherapy completed all of the tests performed in the study (neurological examinations, EORTC QLQ-CIPN20, EORTC QLQ C-30, and NCS).
Statistical analysis
The EORTC QLQ-CIPN20 and NCS results between serial assessments were compared using a two-tailed Student's t-test for paired observations. Bivariate correlation analyses were conducted to assess the associations between each score on EORTC QLQ-CIPN20 and EORTC QLQ C-30 and severity grades 0–3 on the NCI-CTCv3. The NCS results were expressed as percentages with respect to the values at prior assessments for each patient. Receiver operating characteristics analyses were performed to estimate the optimal cutoff in NCS with respect to the grade-3 neuropathy at the end of treatment. Differences in the characteristics among OIPN severity groups were assessed using the t-test and Mann-Whitney test (for continuous variables), one-way ANOVA (for comparisons of continuous variables between three groups), or the χ2 test and Fisher's exact test (for categorical variables). The relationships between factors and severe OIPN (grade-3 neuropathy) were evaluated using a logistic regression model. Univariate analyses were first conducted separately for potentially related factors, and then variables for which p<0.2 were included in the multivariate model to predict the probability of developing severe OIPN. The final model was determined using a backward variable selection method with an entry criterion of p<0.05. SAS software (version 9.3, SAS Institute, Cary, NC, USA) was used for all analyses. Two-sided p values of <0.05 were considered statistically significant.
RESULTS
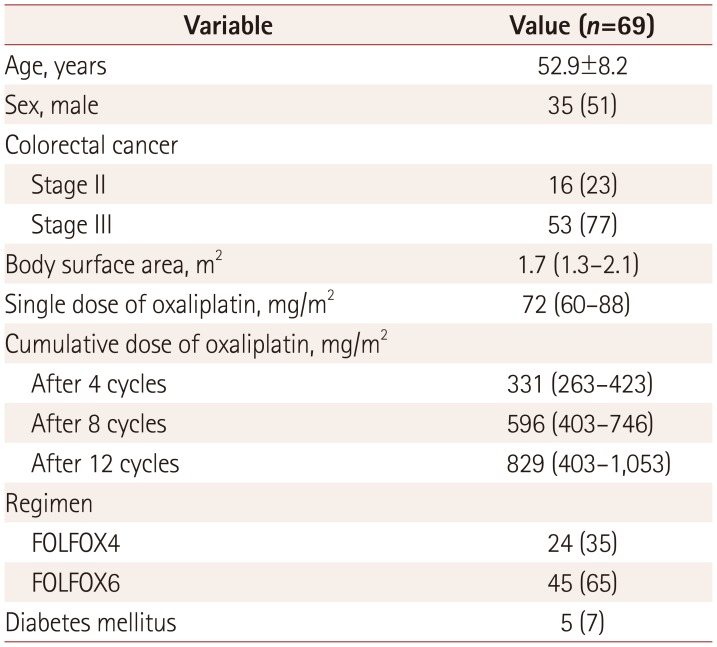
Serial evaluations were completed in 69 patients after 12 cycles of treatment. The baseline characteristics of the 69 patients are listed in Table 1. The median cumulative dose of oxaliplatin was 829 mg/m2 (range, 403 to 1,053 mg/m2). Dose reduction of oxaliplatin was performed in 49 (71%) patients, and this was applied due to neurotoxicity in 9% of the patients.
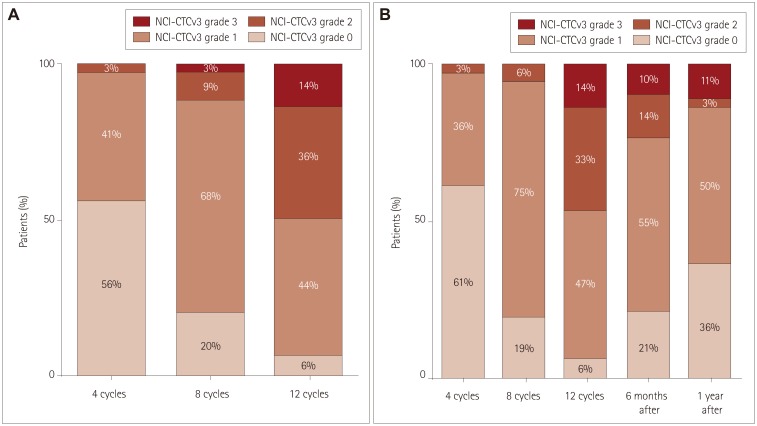
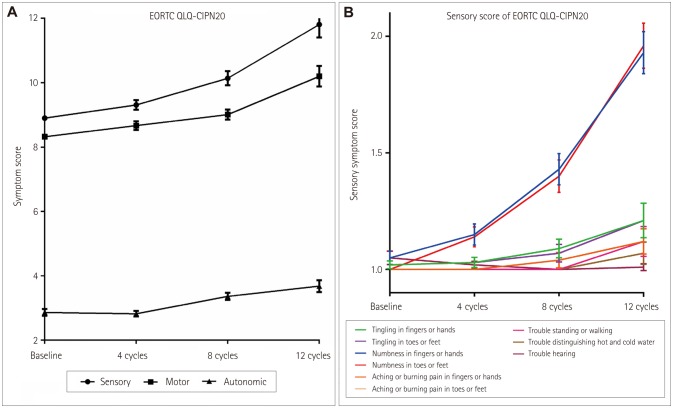
Chronic OIPN was present in 65 (94%) of the 69 patients at the completion of chemotherapy. The severity of cumulative OIPN, as graded using the NCI-CTCv3, worsened during the treatment. The frequency of chronic OIPN with a severity greater than grade 2 was increased in 3, 12, and 50% of patients after 4, 8, and 12 cycles of treatment, respectively. At the end of therapy, OIPN of grades 1, 2, and 3 was present in 30 (44%), 25 (36%), and 10 (14%) patients, respectively (Fig. 1A). All sensory, motor, and autonomic scores on EORTC QLQ-CIPN20 increased with repeated cycles of treatment (Fig. 2). Among sensory symptoms, the incidence of numbness in the fingers and hands/toes and feet increased more than the other symptoms of tingling, aching, and burning pain. Higher grades of OIPN at the end of treatment were associated with higher sensory (r=0.596, p<0.001), motor (r=0.671, p<0.001), and autonomic (r=0.416, p<0.001) scores on EORTC QLQ-CIPN20. Higher OIPN grades were also associated with worse global health (r=−0.430, p<0.001), functional (r=−0.570, p<0.001), and symptomatic (r=0.421, p<0.001) scores on EORTC QLQ C-30.
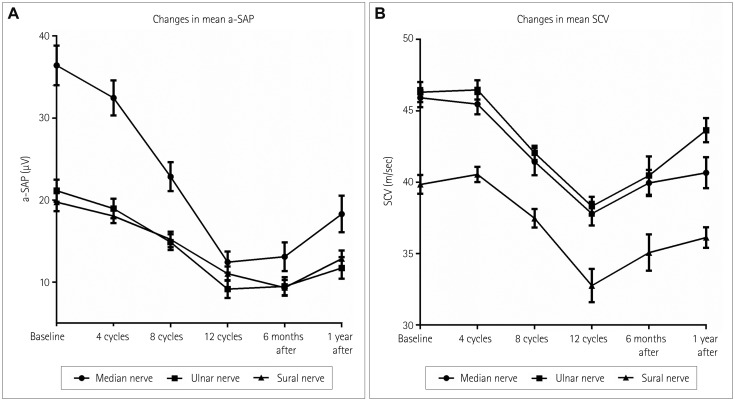
The neurophysiological examinations revealed that the mean values of the a-SAP and SCV in the sural, median, and ulnar sensory nerves reduced significantly during the treatment. Significant reductions of the a-SAP in the median, ulnar, and sural nerves (p=0.029, 0.013, and 0003, respectively) and of the SCV in the median nerve began after four cycles of treatment (p=0.025). Changes in the SCV in the ulnar and sural nerves were significant at eight cycles of treatment compared with the baseline values (p<0.001 and p<0.001, respectively). The mean values of CMAP and MCV in the median, ulnar, tibial, and peroneal nerves did not change significantly during the treatment. The frequency of any abnormalities in the a-SAP or SCV in the median, ulnar, or sural nerves compared with normative age-matched controls was 14, 42, and 83% after 4, 8, and 12 cycles of treatment, respectively. Abnormalities in the SCV in the median nerve were observed most frequently after four cycles of treatment (7%) and during the treatment (up to 68%), while abnormalities in the a-SAP in the sural nerve were observed least frequently at the end of treatment (14%).
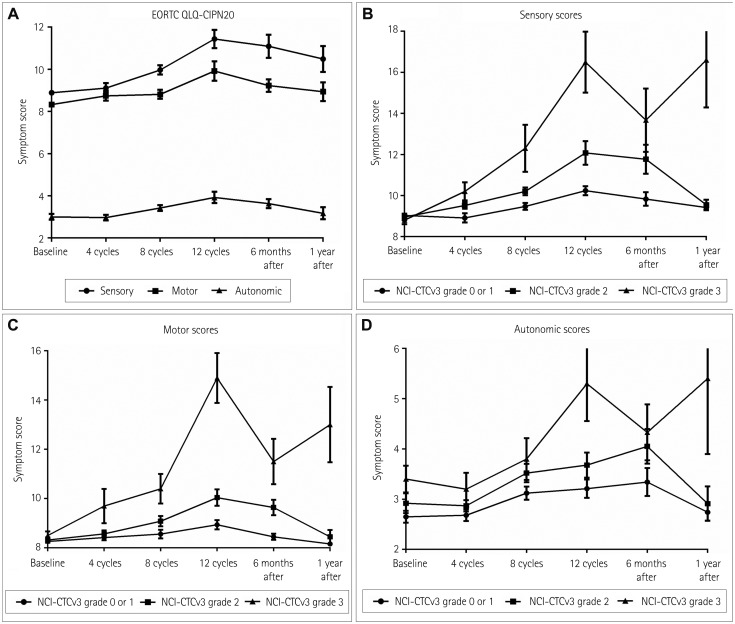
We applied subgroup analysis to the 36 patients who completed the follow-up at 1 year after the end of treatment. This revealed grade-3 neuropathy in 14% of these patients, which was the same proportion as that for the entire cohort of 69 patients (Fig. 1B). At 1 year after the end of treatment, OIPN of grades 1, 2, and 3 was observed in 50, 3, and 11% of the patients, respectively. There was a significant correlation between higher grades of neuropathy at the end of treatment and 1 year after treatment (p<0.001). The mean scores on all sensory, motor, and autonomic scales of EORTC QLQ-CIPN20 decreased gradually after the end of treatment (Fig. 3). However, the mean scores for sensory symptoms at 1 year after the end of treatment were still higher than those at baseline (p=0.015). We compared the EORTC QLQ-CIPN20 scores at 1 year after the cessation of chemotherapy between patients with different NCI-CTCv3 grades at the end of treatment. Patients with OIPN of grades 0–2 showed significant reductions of sensory, motor, and autonomic scores at 1 year after the end of treatment compared with those at the end of treatment (p=0.001, 0.001, and 0.001, respectively), whereas patients with grade-3 OIPN did not show significantly improved sensory, motor, and autonomic scores even at 1 year after the end of treatment. Functional and symptomatic scores on EORTC QLQ C-30 at 1 year after treatment were significantly worse in patients with grade-3 neuropathy than in those with neuropathy of grades 0–2 (p<0.001 and p<0.001, respectively). NCS revealed recovery of the a-SAP and SCV in sensory nerves after the end of treatment (Fig. 4). There was a notable recovery in the NCS SCV in the median nerves (p<0.001) at 6 months after the end of treatment. However, up to this point, the mean a-SAP in the sural nerve continued to worsen (p=0.001). At 1 year after the end of treatment, significant recovery of the mean a-SAP and SCV in all of the examined sensory nerves was found compared to after 12 cycles of treatment. Nevertheless, the mean a-SAP and SCV in all of the examined sensory nerves were still significantly reduced at 1 year after the end of treatment compared with the baseline values.
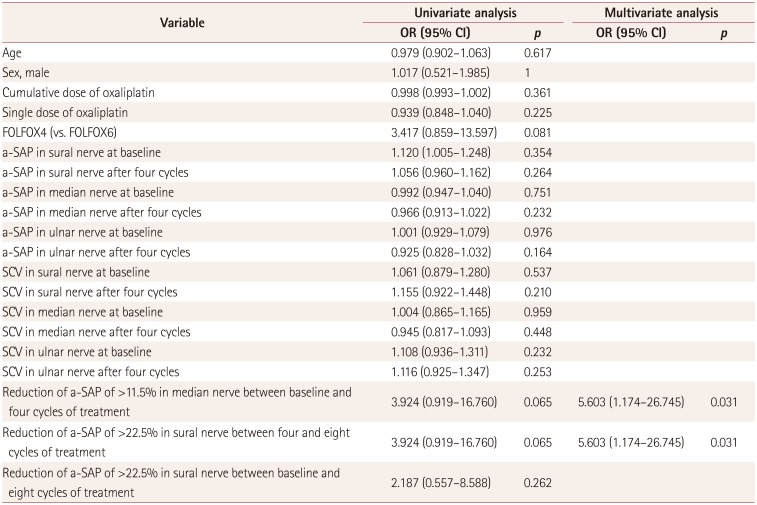
To investigate the potential predictors of grade-3 neuropathy after 12 cycles of treatment, we compared demographic factors, treatment regimens, frequency of diabetes, and NCS results between patients with OIPN of grade 3 and grades 0–2 at the end of treatment. There were no differences in the mean age, sex ratio, frequency of diabetes, cumulative doses, dose intensity, use of the FOLFOX6 vs. FOLFOX4 regimens, and NCS results between the two groups. Multivariate logistic analyses revealed that grade-3 OIPN during the treatment was independently associated with reductions of the a- SAP of >11.5% in the median nerve between baseline and four cycles of chemotherapy (odds ratio=5.603, 95% confidence interval=1.174–26.745; p=0.031). Grade-3 OIPN was also associated with reductions of the a-SAP of >22.5% in the sural nerve between four and eight cycles of chemotherapy (odds ratio=5.603, 95% confidence interval=1.174–26.745; p=0.031) (Table 2).
DISCUSSION
This longitudinal study found that chronic OIPN was present in 94% and 64% of colon cancer patients at the end of oxaliplatin treatment and 1 year after treatment, respectively. The main clinical characteristics of cumulative OIPN were distal numbness and tingling in the fingers and hands/toes and feet, and these symptoms tended to worsen as the cumulative dose of oxaliplatin increased during the 12 FOLFOX treatment cycles. Grade-3 neuropathy was identified in 0, 3, and 14% of patients after 4, 8, and 12 cycles of treatment, respectively. These results are consistent with previous studies finding chemotherapy-induced neuropathy in 80–92% of the patients who were treated with the FOLFOX regimen, in which 8–15% of the neuropathies were grade 3.11314 Changes in the electrophysiological test results were consistent with the clinical symptoms worsening during the treatment. The mean a-SAP and SCV in the sural, median, and ulnar sensory nerves worsened during the treatment. However, the frequency of abnormalities in a-SAP or SCV in sensory nerves compared with age-matched references was a less sensitive predictor of the development of clinical neuropathy; for example, the a-SAP in the sural nerve was within the normal range in 86% of our patients by the end of treatment.
As described above, neuropathic symptoms improved overall after the end of chemotherapy. Previous clinical trials have suggested that OIPN is reversible based on the incidence of grade-3 neuropathy decreasing from 8.2–12.5% during treatment to 0.6–1.3% at a 1-year follow-up.11415 Nevertheless, we found long-standing severe neurotoxicity in a substantial proportion of our patients, with grade-3 OIPN present in 11% of patients at 1 year after treatment cessation. The course of neuropathic symptoms and QoL in patients with grade-3 neuropathy at the end of treatment is less favorable up to 1 year after the end of chemotherapy than in patients with neuropathy of grades 0–2. Recent studies evaluating long-term outcomes of chronic OIPN713161718192021 have also suggested that this condition is not reversible in certain patients up to 11 years after chemotherapy discontinuation. At 1 year after completing chemotherapy, significant recovery of the a-SAP and SCV in all of the examined sensory nerves was found compared with after 12 cycles of treatment; however, the a-SAP and SCV in the sensory nerves did not return to baseline values. These results are consistent with previous reports of sensory nerve deficits persisting for years after the cessation of oxaliplatin therapy.1319 The present study found that a-SAP in the sural nerve continued to worsen for 6 months after completing the chemotherapy; this is often referred to as “coasting,” which is a well-described phenomenon when taking cisplatin2223–at least 6 months may be required before recovery can be observed.
Considering the less favorable clinical course of patients with grade-3 neuropathy, it is important to identify those at risk of this condition. The risk of severe OIPN increased with the cumulative oxaliplatin dose in this study, which is consistent with previous studies.1824 This situation has prompted recent studies to evaluate if the number of FOLFOX cycles could be reduced in order to lessen the risk of neurotoxicity while preserving the survival effect of treatment.2526 Nevertheless, the cumulative dose does not always predict grade-3 neuropathy at an individual level. In our study, 3% of patients already exhibited grade-2 neuropathy after 4 treatment cycles, whereas approximately half of all patients were normal or had only grade-1 neuropathy after completing 12 treatment cycles. The relationship between dose and neurotoxicity might not be linear before reaching a cumulative dose level beyond which the toxicity becomes dose-dependent.24 Recent pharmacogenetic studies have investigated target genes in the oxaliplatin metabolism, detoxification, or excretion pathways to predict severe OIPN.272829 The present study identified reductions of the a-SAP of >11.5% in the median nerve between baseline and four cycles (p=0.031) and of >22.5% in the sural nerve between four and eight cycles (p=0.031) as early predictors of the development of severe OIPN at the end of treatment. These findings are similar to a >30% decrease in the a-SAP from the baseline value in the radial and dorsal sural nerves mid-treatment being associated with severe OIPN at the end of treatment.24 Thus, serial assessments of sensory nerves using NCS during oxaliplatin treatment can be useful to predict severe OIPN.
This study was limited by the smallness of its sample. Other potential limitations relate to the use of the NCI-CTCv3 scale as the main end point of the study–this scale has been criticized for exhibiting interobserver inconsistencies when scoring chemotherapy-induced peripheral neuropathy, and for tending to underscore its severity.30 Nevertheless, the NCI-CTCv3 scale is the most widely used scale in clinical trials, and our grading of neuropathy using the NCI-CTCv3 scale exhibited a strong correlation with patient-reported outcomes.
In conclusion, the present analysis confirmed that OIPN persists for up to 1 year after chemotherapy discontinuation, especially in patients with grade-3 neuropathy. Our results can also potentially be used to identify a subgroup of patients at an increased risk of developing severe OIPN in the early phase of treatment, which is important for identifying patients who require dose modification. Further studies involving larger numbers of patients are needed to confirm the present preliminary data and validate the use of our identified predictors for severe OIPN.
 XML Download
XML Download