

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Febrile seizures (FS) are the most common seizures in children younger than 5 years, and they reportedly affect 2–5% of the pediatric population.1 FS are considered benign and self-limiting. Upper airway viral infections rather than gastrointestinal illnesses are the most common triggering factors.23 The reported incidence rates for second and third episodes of FS are 20–30% and 15%, respectively.4 The risk of developing epilepsy after a simple FS episode has been reported as 2–3%.5 Although FS have an excellent prognosis, they are also a source of anxiety for both parents and family members, and so it is therefore important to determine the exact incidence and recurrence rates. The clinical signs of FS have not differed among populations, but the prevalence rate does differ between regions, such as being 8.2% in Fuchu, Japan, 14% in Guam, and 34.0% in Australia.678
No previous investigation has been based on Korean national data, and so this study aimed to determine the incidence and clinical and epidemiological characteristics of Korean patients with FS using a national database.
METHODS
Data acquisition
We analyzed data from the Korea National Health Insurance Review and Assessment Service (HIRA) for 5 years (2009–2013). More than 97% of the South Korean population is enrolled in the Korea National Health Insurance (NHI) program. The HIRA is a government-affiliated organization that performs claims review and quality assessment for NHI. Data for the remaining 3% of the population covered by the Medical Aid Program are also reported to the HIRA.9 Every clinic and hospital in Korea submits patient diagnostic and medical cost data to the HIRA, for reimbursement by the government. This situation means that nearly complete information about the volume and burden of disease in Korea can be obtained from this centralized database, with the exception of procedures that are not covered by insurance, such as cosmetic surgery. Many epidemiological analyses have used this database. According to the Korean Statistical Information Service (http://kosis.kr/), the information for the population younger than 5 years differed only slightly from that covered by NHI. A population-based study could therefore be performed because NHI covers almost all Korean residents.
Extraction of FS data
We extracted data from this national registry for the period from January 1, 2009 to December 31, 2013, and used codes of the International Classification of Diseases (ICD)-10 code to determine the prevalence of febrile convulsions. The following ICD-10 codes were analyzed: R56.0 (FS) combined with G41 (status epilepticus) or R56.8 (convulsions). The study population was divided into those aged up to 10 years and those older than 10 years. The data included the coded patient identity, date of first visit, patient age at last visit in a given year, and sex. Only yearly ages were available, and so monthly ages were not recorded. Patients older than 20 years and those who visited for repeated episodes of FS within 28 days (even to different hospitals) were excluded.
The prevalence rate was analyzed based on the occurrence of FS compared to the mean population younger than 5 years in 2009–2013. The incidence and recurrence rates of FS were analyzed for those born in 2009 to ensure that the first episode of FS was included. Data were collected for the second to fifth visits after the first visit for FS. The study was approved by the Center Institutional Review Board (approval no. KUGH16019).
RESULTS
Study population
The total population recorded in the Korean Statistical Information Service database was compared with the population covered by NHI. The populations were very similar, and the number recorded as being covered by health insurance actually exceeded the total population for some of the years (Supplementary Table 1 in the online-only Data Supplement).
FS prevalence
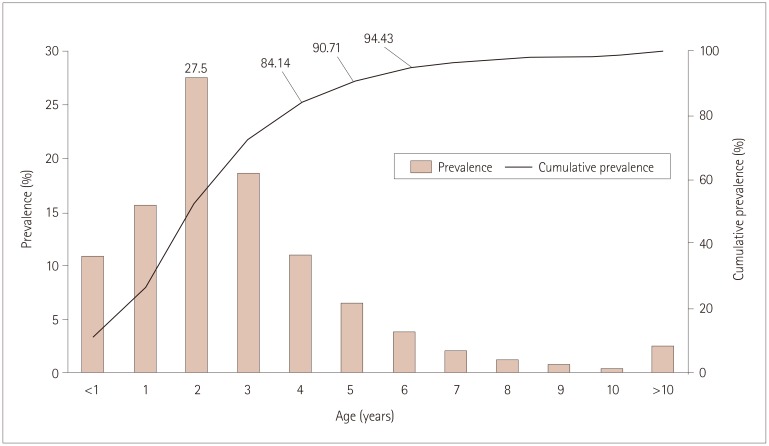
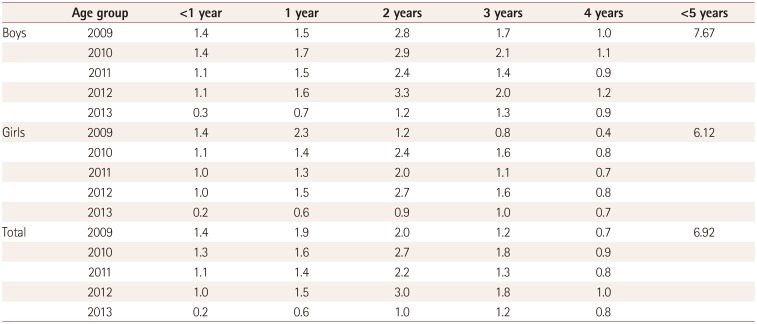
The number of patients with FS younger than 10 years was 38,659 in 2009, 43,522 in 2010, 34,888 in 2011, 45,624 in 2012, and 23,173 in 2013. The prevalence of FS in Korea in those younger than 5 years was 69.2/1,000 (76.7/1,000 for boys and 61.2/1,000 for girls) (Table 1). The prevalence peaked among children who were aged 2 years on the last day of each calendar year, and so the age range of the peak prevalence included those aged 18–30 months (Fig. 1). The occurrence rates in children younger than 4, 5, and 6 years were compared with the total occurrence rate in children younger than 10 years; these were 84.1, 90.7, and 94.4%, respectively (Fig. 1).
Incidence and recurrence rates
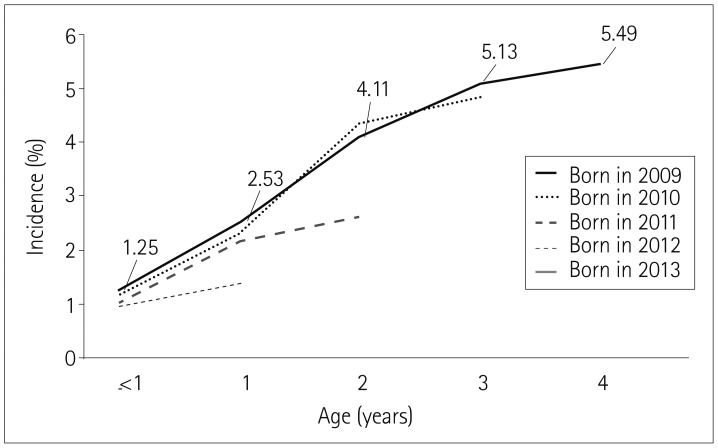
To determine the exact incidence of FS, we analyzed 5-year data for children born after 2009. The incidence of FS in Korea was 54.9/1,000 children among those aged 4 years (age range 42–54 months) (Fig. 2). Among those younger than 5 years, the FS prevalence was 84.1% of all those with FS who were younger than 10 years, and so the estimated incidence of FS was 65.3/1,000.
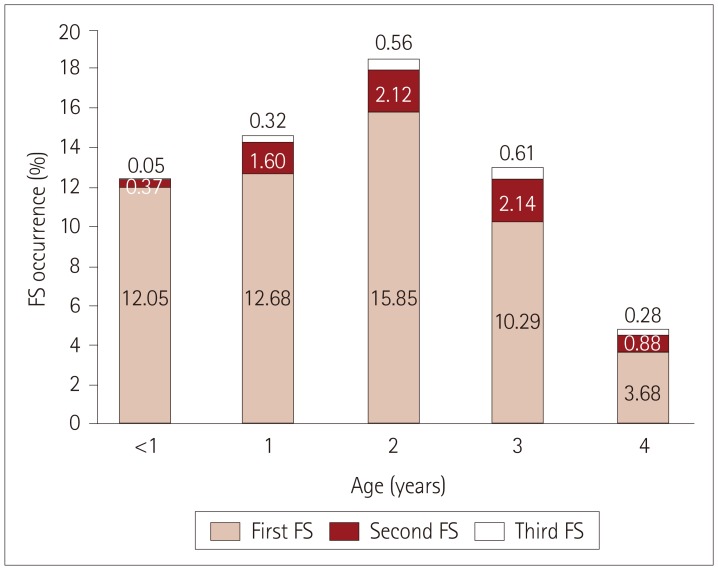
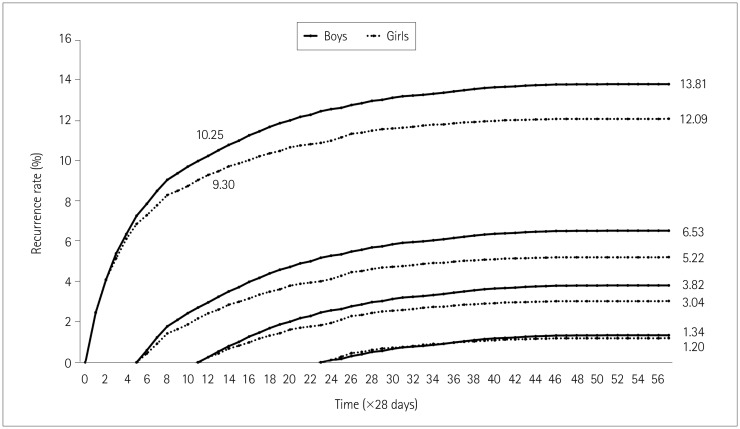
The age at which the first episode of FS occurred must often was also 18–30 months. The recurrence rate of FS peaked among those aged 3 years (age range 30–42 months) (Fig. 3). The overall incidence rates for the second, third, fourth, and fifth episodes of FS in children younger than 5 years were 13.04, 3.35, 1.08, and 0.43%, respectively. The recurrence rate for FS was higher (Fig. 4). In one year after first episode of FS the recurrence rate was 10.25% in boys and 9.30% in girls. However, if there was no recurrence of FS in the 6 months following the first episode of FS, the recurrence rate was more than halved, to 6.53% in boys and 5.22% in girls (Fig. 4).
DISCUSSION
This study has provided accurate population information based on analysis of the NHI database. FS is not a disabling diagnosis; it is usually benign and is not stigmatized, which is likely to result in a high reporting rate. Moreover, there are fewer overlapping ICD-10 codes for FS. These characteristics mean that the results are relatively reliable, in contrast with those for other narrow-spectrum diseases that are difficult to diagnose, or broad-spectrum diseases that appear in many ICD-10 codes. Very few of the patients in this study had codes for both status epilepticus and FS. The definitions of status epilepticus include durations from 30 minutes to 5 minutes, and approximately 5% of FS are known to last 30 minutes.10 A single diagnosis conforms with the requirements for reporting to the HIRA, and so physicians might not report multiple codes, thus potentially making it difficult to accurately estimate the incidence of febrile status epilepticus. The HIRA provides administrative data, not research data, which could introduce bias into the estimates. Moreover, the prevalence and incidence of FS might have been underestimated with the exception of recurrent FS within 28 days. This study was limited by the insufficiency of data on patient characteristics such as seizure types, duration of seizures, and patient and family histories, and by being restricted to children younger than 5 years for the determination of incidence and recurrence rates.
This 5-year study found that the annual prevalence of FS in Korean children younger than 5 years ranged from 3.8% to 8.3% during 2009–2013, with the annual prevalence being lowest in 2013. Further studies are needed of the prevalence rates of other endemic infections. The 5-year prevalence of FS in Korea was 6.92%, which was higher than the reported mean prevalence of 2–5%.1 Both the prevalence and incidence rates for FS were higher in boys than girls, and the male/female ratio was 1.25:1, which was consistent with previous studies.11 However, in contrast with the present study, there are reports of no significant sex-related differences.12 The incidence of FS was previously reported to peak at 18 months,13 which is similar to our estimated results. The HIRA did not release accurate monthly ages or birth dates due to privacy concerns, and so we used age ranges based on the age at the end of the calendar year.
The reported recurrence rate of FS has ranged from 30% to 40%,414 which is much higher than the rate observed in the present study. This discrepancy might have been due to our exclusion of recurrent seizures within 28 days, missed hospital visits, and only including those younger than 5 years. Only 3.35% of the FS children included in this study experienced a third episode of FS, and previous studies have found rates of three occurrences of FS from 4.1% to 9%.415 Recurrent FS is a risk factor for developing epilepsy after FS, and third episodes of FS are relatively rare, so a child with a third episode of FS needs to be monitored carefully and assessed for the possibility of recurrence and epilepsy.
The HIRA released data for 2009. Although not considered a form of epilepsy, FS can represent the first sign of subsequent epilepsy. Future population-based cohort studies should determine the prevalence of subsequent seizures, medication, and incidence of epilepsy in patients with FS.
 XML Download
XML Download